All published articles of this journal are available on ScienceDirect.

Effect of Oxytocin Massage and Slow-Stroke Back Massage on Breast Milk Production and Reduction of Risk Factors Associated with Stunting: A Randomized Controlled Trial
Authors Info & Affiliations
Abstract
Introduction
Stunting is a significant issue in developing countries. Proper breastfeeding is a key preventive strategy. However, many mothers face delays or inadequate breast milk production after giving birth. This study examines the impact of oxytocin massage and Slow-Stroke Back Massage (SSBM) on enhancing breast milk production among postpartum women.
Methods
This randomized controlled trial included 75 postpartum mothers, divided into three groups. The first group received oxytocin massage, as described in the intervention procedure. The second group received both oxytocin massage and Slow-Stroke Back Massage (SSBM), in which the nurse used gentle, rhythmic, and continuous strokes across the mother's back to promote relaxation and comfort. The third group received only routine hospital care, including standard breastfeeding education and standard postpartum monitoring without any massage intervention.
Results
Seventy-five postpartum mothers (mean age 30.6 ± 7.0 years) participated in this study. Most mothers were multigravida (78.7%), had secondary education (45.3%), were housewives (50.7%), and attended regular antenatal care (78.7%). Breast milk production was evaluated using two indicators: sufficiency of milk supply and length-for-age Z-score at two months. Data analysis shows the SSBM combination massage increased breast milk production in the SSBM group compared to the oxytocin massage group and the control group (routine procedures). It also suggests positive effects on early growth indicators linked to stunting risk (p = 0.001).
Discussion
The combined intervention improved effective breastfeeding practices. This strategy may enhance child health and survival, with long-term benefits for stunting prevention.
Conclusion
Combining SSBM with oxytocin massage for postpartum mothers could be a promising adjunct in postnatal care. This intervention offers relaxation benefits, enhances milk production, and may improve early growth indicators associated with stunting risk. Larger and longer-term studies are needed to confirm effects on stunting outcomes.
1. INTRODUCTION
The postpartum period is a critical time. Mothers must care for themselves and their infants through exclusive breastfeeding. These multiple responsibilities can cause discomfort, which may reduce milk production and the success of exclusive breastfeeding in newborns [1].
Babies who are not exclusively breastfed have a higher risk of stunting. Stunting has multidimensional causes, but interventions in the first 1,000 days, especially adequate nutrition and exclusive breastfeeding, are key. Literature shows that children given exclusive breastfeeding are much more likely to have only mild or no stunting [2, 3].
Breast milk provides optimal nutrition for babies, supporting better health [4]. Exclusive breastfeeding may be hindered by limited maternal knowledge [5], lack of family support, poor care, use of formula, or low milk production [6]. Additional obstacles include not rooming in, infrequent breastfeeding, and insufficient knowledge about milk production. Mothers with low milk production may breastfeed less often, while those with good milk supply do so more often. Despite this, infants may still be fussy, have short feeding sessions, or require formula [7].
Postpartum mothers are at risk for anxiety. The symptoms include fatigue, irritability, insomnia, low milk supply, and, rarely, maternal death. Slow-stroke back massage may help relax muscles and release endorphins, which can reduce anxiety. Relaxation interventions such as oxytocin and Slow-Stroke Back Massage (SSBM) improve comfort, reduce anxiety, and enhance breast milk production. In a Dutch study, 14.7% of 1,406 mothers had postpartum anxiety. In Iran, 85.5% of mothers reported postpartum anxiety, with levels decreasing after intervention [8].
Anxiety in postpartum mothers can hinder the breastfeeding process. Research in Makassar, Indonesia, included 20 anxious mothers. It showed that 13 (65.0%) had irregular breast milk production. In contrast, 31 people who were not anxious mostly showed smooth breast milk production (26, 83.9%) [9].
The rolling massage technique or oxytocin massage improves breast milk sufficiency in newborns [10]. This effect is especially strong when combined with relaxation techniques [11]. In a Yogyakarta study, 51% of respondents who received oxytocin massage more than three times in the first postnatal week experienced lactation problems. Only 16.3% without a massage reported issues. By the fourth postnatal visit, all respondents had no further problems. Most 2-month-old infants' heights (98.8%) were within the expected age range [12]. Back massage provides postpartum comfort. It increases oxytocin and prolactin, which promote comfort and improve breast milk production [13]. The study aimed to test whether using oxytocin massage with Slow Stroke Back Massage increases breast milk production and reduces risk factors for stunting in postpartum mothers. Both methods are believed to help mothers relax and enhance milk supply, thereby reducing the risk of infant stunting.
2. METHOD
2.1. Study Design
This study used a Randomized Controlled Trial (RCT) with pre- and post-test control groups. It included postpartum mothers who delivered vaginally or via Caesarean section and who roomed in. Mothers were excluded if they had complications, were in high-care units, or had babies with congenital disabilities. The dependent variables were breast milk production (daily urination, infant not fussy or sleeping well, babies' weight), and babies' length, while the independent variables included oxytocin massage and slow-stroke back massage (SSBM). Control variables were maternal and infant characteristics.
2.2. The Participants
The population was randomized into three groups: two intervention groups and one control group. Although this sample was smaller than the ideal 246, the finite population correction (FPC) indicates that 70 participants would suffice. FPC is used when the population is small (under 10,000) and sampling is without replacement. It reduces the required sample size, since a small sample can represent a small population. Thus, the adjusted sample size was about 70–75. The final sample size, using FPC, was about 75.
2.3. Data Collection
Seventy-five postpartum mothers were divided into three groups. The first group received only oxytocin massage, administered by trained staff. The second group received both oxytocin massage and the SSBM intervention, a structured support program also delivered by trained personnel. The control group received routine hospital care without additional interventions. Breast milk production was evaluated using three indicators: at least six newborn urinations per day, the baby not being fussy or excessively sleepy, and the baby maintaining normal weight and body length. Early stunting detection was conducted using the length-for-age z-score (<-2 SD), calculated from two separate measurements taken over two months.
Breast milk production was assessed by counting daily urinations. At least 6 wet diapers meant adequate production. Mothers reported infants' behavioral states as either Satisfied (calm or sleepy) or Fussy (crying or restless) after breastfeeding. Weight and height were measured using standard techniques. A UNICEF-recommended wooden board and calibrated tape were used. Data collection took about 20–25 minutes per participant, including interviews and physical measurements.
Group One: received oxytocin massage intervention. The procedure began by assessing the respondent's condition and positioning her sitting on the edge of the bed with a towel placed under her breasts. The nurse applied baby oil to both palms, then massaged the respondent's back from the base of the neck to both breasts. The massage was performed along both sides of the spine, moving downward (from the neck to the shoulder blades) in small circular motions using the thumbs and applying gentle pressure. This movement was repeated 5–10 times. Finally, the nurse cleaned the respondent's back with warm and cold water, alternating between them, using a washcloth. The materials used in this procedure included a towel, washcloth, basin, and massage oil [11].
Group Two: Combination of Oxytocin Massage and SSBM. The procedure began by assessing the respondents' condition and positioning them sitting on the edge of the bed. A towel was placed under their breasts, and the nurse applied baby oil to their palms. The nurse first performed a rolling massage, followed by SSBM. In the first movement, the nurse held the respondents' upper shoulders with both hands, placed both thumbs just below the base of the skull, and made small circular motions across the upper neck. In the second movement, one hand was placed at the base of the skull and slowly, gently stroked downward along the spine to the waist; the other hand followed as the first returned to its original position. In the third side movement, both hands were placed on each respondent's neck just below the ear, stroking downward across the collarbone while the thumbs glided over the shoulder blades three times. In the fourth movement, both thumbs were placed on each side of the back, starting at the shoulder and moving down to the waist with gentle pressure. In the final side movement, both hands were placed on each respondent's neck, then stroked long, continuous strokes down across the shoulders and the entire spine. This movement was repeated several times, with the entire procedure lasting 15–20 minutes. Once completed, the nurse wiped off any remaining baby oil using alternating warm and cool wet washcloths and helped the patient return to a comfortable position. Materials used in this combined procedure included gloves, pillows, towels, washcloths, a basin, massage oil, a breast milk container, and relaxation music [14].
Group Three: Routine Hospital Care. The third group served as a control group, receiving only routine hospital care. This care generally included standard postpartum hygiene care, such as monitoring uterine involution and breast care for milk expression.
The first assessment occurred at 1 month, followed by a second at 2 months. Data collection involved home visits to assess criteria, including at least six urinations per day, a non-fussy or sleeping behavioral state, and normal physical growth indicators, such as weight and length. Post-collection, data completeness was verified, and the data were then recoded and categorized.
2.4. Data Analysis
Analysis was performed with STATA 13. Statistical analysis was conducted at two levels. First, within-group changes in breast milk adequacy (a binary outcome) across three time points (birth, 1 month, 2 months) were examined using McNemar’s Exact Binomial test within each group. Within-group changes in continuous growth outcomes (body length and length-for-age Z-score) were analyzed using the paired t-test for normally distributed data and the Wilcoxon signed-rank test for non-normal distributions. Second, and critically, between-group comparisons were conducted to directly assess intervention effects. Differences in breast milk adequacy rates across all three groups at each time point were compared using the Chi-square test or Fisher’s Exact test as appropriate, with Cramer’s V reported as the effect size measure. For continuous outcomes (Z-scores and body length), a one-way ANOVA with Bonferroni post hoc pairwise comparisons was used to compare groups at each time point; partial eta-squared (η2) was reported as the effect size. All analyses report point estimates with 95% confidence intervals (95% CI). A significance threshold of α = 0.05 was applied. To address baseline imbalances in family income and infant urination frequency, ANCOVA (for continuous outcomes) and logistic regression (for binary outcomes) were conducted as sensitivity analyses, with the imbalanced variables entered as covariates. Results from both unadjusted and adjusted analyses are reported where applicable.
2.5. Ethical Considerations
The study received ethical approval from the ethics committee at Zainoel Abidin General Hospital, Aceh, Indonesia (Ref No. 267/ETIK-RSUZA/2025). Permission was granted by hospital management. Verbal informed consent was obtained from participants, including explanations of their rights and the study's purpose. Participants were told they could withdraw at any time. The research adhered to ethical standards and received hospital authorization. The stages of this research use the CONSORT pattern as presented in Fig. (1):
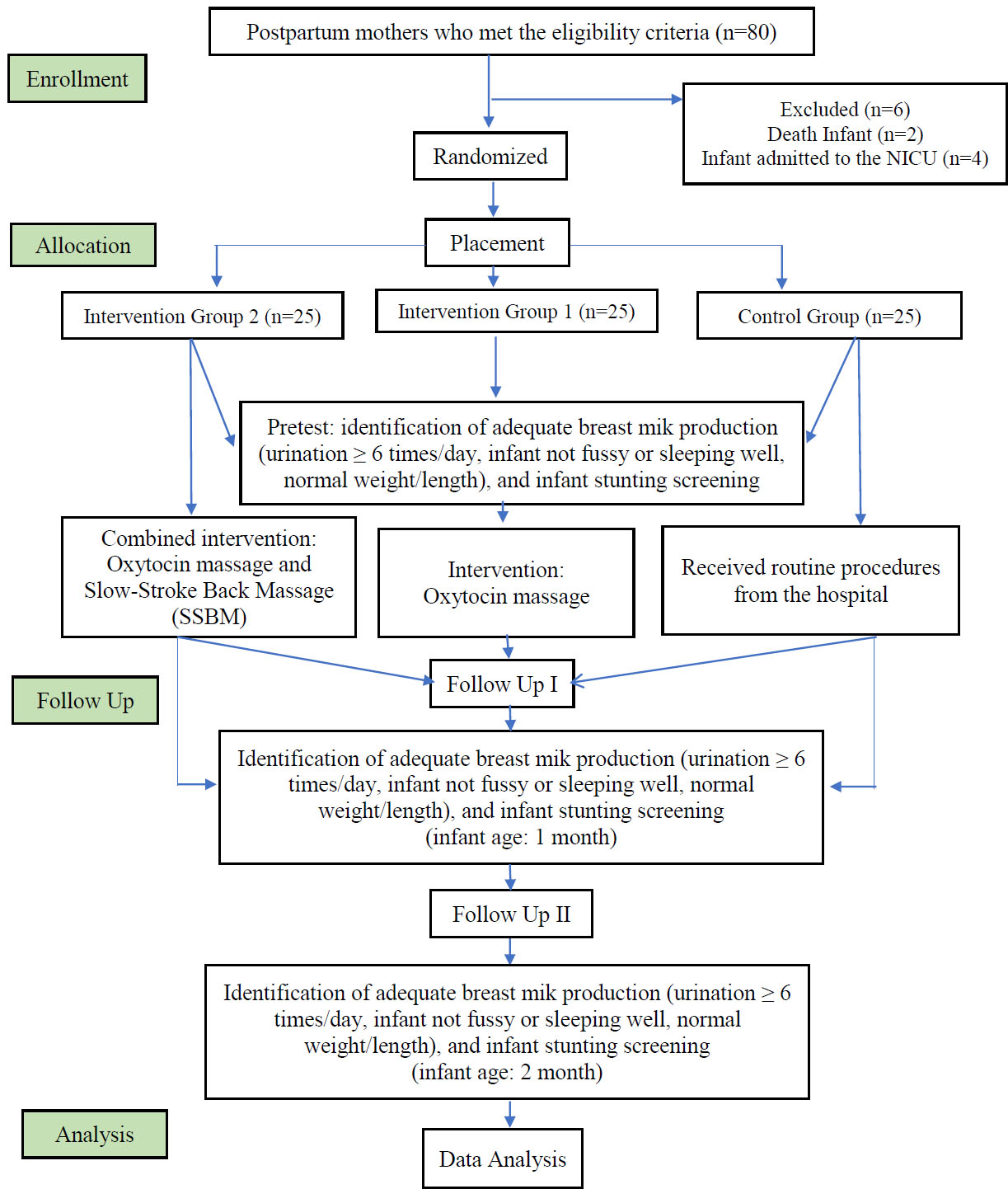
Research flow scheme.
3. RESULTS
3.1. Characteristics of Study Participants
A total of 75 postpartum mother including their infants, participated in the study. Table 1 presents the baseline characteristics of postpartum mothers and their infants across three study arms: Intervention Group 2, receiving combined SSBM and Oxytocin Massage (SSBM+OM); Intervention Group 1, receiving Oxytocin Massage alone (OM); and the control group. Each group consisted of 25 mother–infant pairs. Overall, most maternal and infant characteristics were comparable across groups, indicating adequate baseline balance before intervention, with only a few variables showing statistically significant differences.
| Characteristics |
Intervention Group 2 (SSBM+OM) n = 25 |
Intervention Group 1 (OM) n = 25 |
Control Group n = 25 |
p-value | |||
|---|---|---|---|---|---|---|---|
| n | (%) | n | (%) | n | (%) | ||
| Maternal Characteristics | - | - | - | - | - | - | |
| Age | - | - | - | - | - | - | 0.486 |
| <20 years | 0 | (0.0) | 1 | (4.0) | 0 | (0.0) | |
| 21–34 years | 18 | (72.0) | 15 | (60.0) | 14 | (56.0) | |
| ≥35 years | 7 | (28.0) | 9 | (36.0) | 11 | (44.0) | |
| Mean ± SD | 29,0 ± 6,8 | 31,1 ± 6,3 | 31,8 ± 7,8 | - | |||
| Parity | - | - | - | - | - | - | 0.356 |
| Primigravida | 3 | (12.0) | 6 | (24.0) | 7 | (28.0) | |
| Multigravida | 22 | (88.0) | 19 | (76.0) | 18 | (72.0) | |
| Education | - | - | - | - | - | - | 0.630 |
| Primary | 8 | (32.0) | 9 | (36.0) | 9 | (36.0) | |
| Secondary | 12 | (48.0) | 9 | (36.0) | 7 | (28.0) | |
| Tertiary | 5 | (20.0) | 7 | (28.0) | 9 | (36.0) | |
| Occupation | - | - | - | - | - | - | 0.846 |
| Housewife | 13 | (52.0) | 14 | (56.0) | 12 | (48.0) | |
| Entrepreneur | 3 | (12.0) | 7 | (28.0) | 6 | (24.0) | |
| Teacher | 4 | (16.0) | 2 | (8.0) | 3 | (12.0) | |
| Contract Worker | 4 | (16.0) | 2 | (8.0) | 3 | (12.0) | |
| Nurse | 1 | (4.0) | 0 | (0.0) | 1 | (4.0) | |
| ANC History | - | - | - | - | - | - | 0.727 |
| Regular (≥6 visits) | 21 | (84.0) | 19 | (76.0) | 19 | (76.0) | |
| Irregular (<6 visits) | 4 | (16.0) | 6 | (24.0) | 6 | (24.0) | |
| Breastfeeding Exp. | - | - | - | - | - | - | 0.433 |
| Ever | 17 | (68.0) | 20 | (80.0) | 16 | (64.0) | |
| Never | 8 | (32.0) | 5 | (20.0) | 9 | (36.0) | |
| Husband's Education | - | - | - | - | - | - | 0.630 |
| Primary | 7 | (28.0) | 8 | (32.0) | 7 | (28.0) | |
| Secondary | 11 | (44.0) | 11 | (44.0) | 15 | (60.0) | |
| Tertiary | 7 | (28.0) | 6 | (24.0) | 3 | (12.0) | |
| Husband's Occupation | - | - | - | - | - | - | 0.456 |
| Civil Servant | 7 | (28.0) | 2 | (8.0) | 3 | (12.0) | |
| Non-permanent Worker | 12 | (48.0) | 14 | (56.0) | 12 | (48.0) | |
| Contract Worker | 2 | (8.0) | 5 | (20.0) | 6 | (24.0) | |
| Farmer | 4 | (16.0) | 4 | (16.0) | 4 | (16.0) | |
| Family Income | - | - | - | - | - | - | 0.032 |
| < IDR 3.165.000 | 10 | (40.0) | 18 | (72.0) | 10 | (40.0) | |
| ≥ IDR 3.165.000 | 15 | (60.0) | 7 | (28.0) | 15 | (60.0) | |
| Infant Characteristics | - | - | - | - | - | - | - |
| Sex | - | - | - | - | - | - | 0.850 |
| Male | 15 | (60.0) | 13 | (52.0) | 14 | (56.0) | |
| Female | 10 | (40.0) | 12 | (48.0) | 11 | (44.0) | |
| Gestational Age | - | - | - | - | - | - | 0.551 |
| 34–36 weeks | 9 | (36.0) | 6 | (24.0) | 6 | (24.0) | |
| 37–40 weeks | 16 | (64.0) | 19 | (76.0) | 19 | (76.0) | |
| Birth Weight | - | - | - | - | - | - | 0.584 |
| <2.500 gram (g) | 3 | (12.0) | 5 | (20.0) | 5 | (20.0) | |
| 2.500–4.000 g | 22 | (88.0) | 20 | (80.0) | 19 | (76.0) | |
| >4.000 g | 0 | (0.0) | 0 | (0.0) | 1 | (4.0) | |
| Birth Length | - | - | - | - | - | - | 0.688 |
| <48 cm | 13 | (52.0) | 14 | (56.0) | 11 | (44.0) | |
| 48–52 cm | 12 | (48.0) | 11 | (44.0) | 14 | (56.0) | |
| >52 cm | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | |
| Initial Nutrition | - | - | - | - | - | - | 0.730 |
| Exclusive Breast Milk | 22 | (88.0) | 22 | (88.0) | 21 | (84.0) | |
| Breast Milk + Formula | 3 | (12.0) | 3 | (12.0) | 3 | (12.0) | |
| Formula Only | 0 | (0.0) | 0 | (0.0) | 1 | (4.0) | |
| Urination Frequency | - | - | - | - | - | - | 0.000 |
| ≥6 times/day | 24 | (96.0) | 17 | (68.0) | 8 | (32.0) | |
| <6 times/day | 1 | (4.0) | 8 | (32.0) | 17 | (68.0) | |
| Breastfeeding Condition | - | - | - | - | - | - | 0.111 |
| Satisfied | 17 | (68.0) | 22 | (88.0) | 22 | (88.0) | |
| Less Satisfied | 8 | (32.0) | 3 | (12.0) | 3 | (12.0) | |
Note: OM = Oxytocin Massage; SSBM = Slow Stroke Back Massage; n(%) = frequency (percentage); p-values from Levene's test.
Non-permanent workers are those who do not have permanent employment status and work for a specific period, such as under a contract, on a daily basis, or temporarily. Examples include honorary workers, project workers, and temporary employees.
Contract workers are those who work under a contractual agreement and have a specific work period. In Indonesia, this is often referred to as a Fixed-Term Employment Agreement.
IDR 3.165.000=Workers will receive a minimum salary of around IDR 3,165,000 per month according to the minimum wage provisions in Aceh.
Regarding maternal characteristics, maternal age distribution did not differ significantly among groups (p = 0.486). The majority of mothers in all groups were aged 21–34 years, representing the typical reproductive age range, while a smaller proportion were ≥35 years. Very few mothers were younger than 20 years, suggesting minimal influence of adolescent maternal age on study outcomes.
Parity distribution was similar across groups (p = 0.356), with most mothers being multigravida in all arms. This consistency suggests that prior childbirth experience was unlikely to affect breastfeeding outcomes differentially across groups. Educational levels showed no significant variation (p = 0.630), with the majority of mothers having secondary education, and smaller groups with primary or tertiary education. Similarly, maternal occupation was evenly distributed across groups (p = 0.846), with homemakers comprising the largest share, followed by entrepreneurs, teachers, and contract workers. Only a few healthcare workers were present, reducing the likelihood that professional bias would affect breastfeeding practices.
Antenatal care visits were mostly regular (≥6 visits) across all groups, with no notable differences (p = 0.727). Prior breastfeeding experience was also similar (p = 0.433), with the majority of mothers having previous experience, indicating a comparable level of initial breastfeeding readiness. Likewise, husband-related factors, such as education level (p = 0.630) and occupation (p = 0.456), showed no significant differences among the groups, suggesting similar household support environments.
However, family income differed significantly between groups (p = 0.032). A larger proportion of mothers in Intervention Group 1 had incomes below IDR 3,165,000 than in the other two groups. In contrast, higher-income households were more common in Intervention Group 2 and the control group. This imbalance suggests potential socioeconomic variation that may influence maternal nutrition, stress levels, or breastfeeding support, and therefore warrants consideration in interpreting outcomes or adjusting subsequent analyses.
Infant characteristics were consistent across groups: sex distribution was similar (p = 0.850), with a slightly higher proportion of male infants overall. Gestational age was also comparable (p = 0.551), with most infants born at term (37–40 weeks), indicating similar neonatal maturity. Birth weight categories showed no significant difference (p = 0.584), with most infants having normal birth weight (2.500–4.000 g). A small proportion had low birth weight, and very few weighed over 4.000 g. Birth length distribution was also consistent (p = 0.688), with most infants measuring 48–52 cm at birth. Initial postpartum infant nutrition was similar (p = 0.730), with exclusive breastfeeding being predominant across all groups. Minimal formula supplementation was observed, suggesting baseline feeding practices were largely uniform before any intervention effects.
In contrast, infant urination frequency varied significantly among groups (p = 0.000). A notably higher proportion of infants in Intervention Group 2 had urination frequency ≥6 times/day compared to Group 1 and the control group. Conversely, low urination frequency (<6 times/day) was more prevalent in the control group. Since urination frequency indicates hydration status and indirectly reflects adequacy of milk intake, this baseline difference may suggest early disparities in breastfeeding effectiveness. It should be considered when analyzing intervention outcomes. Breastfeeding satisfaction showed no statistically significant difference (p = 0.111), though satisfaction was slightly lower in Intervention Group 2. Still, most mothers across groups reported satisfactory breastfeeding experiences at baseline.
In summary, Table 1 shows that maternal and infant characteristics are generally balanced across study groups, supporting their comparability at baseline. Only family income and infant urination frequency differed significantly, suggesting potential socioeconomic and early feeding differences that may warrant adjustment or discussion when evaluating intervention effects. Overall, the similarity of most baseline variables enhances the internal validity of future comparisons between intervention and control groups.
Table 2 shows the within-group changes in breast milk adequacy from birth to two months across three study groups. Breast milk adequacy was evaluated based on clinical criteria: an infant urinating six or more times daily, absence of persistent fussiness, and proper weight and length growth. Each group consisted of 25 mother-infant pairs. These findings are directly relevant to assessing the effectiveness of massage interventions in boosting breast milk production, which could help prevent early stunting.
| Group | Comparison |
Adequate Pre n (%) |
Adequate Post n (%) |
p-value |
|---|---|---|---|---|
| Intervention Group 2 (SSBM + OM) |
Birth → 1 Month | 17 (68.0) | 19 (76.0) | 0.774 |
| 1 Mo → 2 Months | 19 (76.0) | 25 (100.0) | 0.031* | |
| Birth → 2 Months | 17 (68.0) | 25 (100.0) | 0.007* | |
| Intervention Group 1 (OM only) |
Birth → 1 Month | 17 (68.0) | 17 (68.0) | 1.000 |
| 1 Mo → 2 Months | 17 (68.0) | 24 (96.0) | 0.015* | |
| Birth → 2 Months | 17 (68.0) | 24 (96.0) | 0.039* | |
| Control Group | Birth → 1 Month | 8 (32.0) | 11 (44.0) | 0.581 |
| 1 Mo → 2 Months | 11 (44.0) | 10 (40.0) | 1.000 | |
| Birth → 2 Months | 8 (32.0) | 10 (40.0) | 0.790 |
Note: Adequate = meets breast milk sufficiency criteria (Urinary Frequency ≥6×/day, baby not fussy, normal weight/length); n(%) out of 25 per group; * p < 0.05.
In Intervention Group 2, which received both SSBM and OM, 68% of infants met the adequacy criteria at birth. Then, it increased to 76% at one month, though the difference was not statistically significant (p = 0.774). From one to two months, the proportion reaching adequacy rose to 100%, showing a significant change (p = 0.031). Overall, from birth to 2 months, breast milk adequacy increased significantly from 68% to 100% (p = 0.007). These results indicate that the combined massage intervention has a cumulative effect, substantially enhancing breast milk production and ensuring sufficient intake for all infants by two months.
In Intervention Group 1, which only received Oxytocin Massage, 68% of infants had sufficient breast milk at birth and at 1 month, with no significant early change (p = 1.000). However, over the period between one and two months, adequacy increased to 96%, which is a statistically significant increase (p = 0.015). Overall, from birth to two months, the proportion improved significantly from 68% to 96% (p = 0.039). These results suggest that Oxytocin Massage alone can improve breast milk adequacy. However, its effect is somewhat weaker than that of the combined intervention, as not all infants achieved full adequacy.
In the control group, breast milk adequacy was significantly lower and showed little change over time. At birth, only 32% of infants received adequate breast milk, and this increased slightly to 44% at one month (p = 0.581), but then declined to 40% at two months (p = 1.000). Overall, from birth to two months, the change was not statistically significant (32% to 40%; p = 0.790). These results emphasize the limited natural improvement in breast milk adequacy without intervention and highlight the risk of inadequate intake and early growth delays.
Overall, Table 2 shows that both massage-based interventions enhance breast milk adequacy, with the combined use of SSBM and Oxytocin Massage being the most effective. Significant improvements between one and two months, and between birth and two months, in both groups support the hypothesis that massage can increase milk production. These gains in breast milk sufficiency are especially relevant for preventing early stunting, as proper nutrition during the first two months is essential for supporting healthy growth and minimizing growth delays.
Table 3 shows within-group changes in infant body length and length-for-age Z-scores from birth to two months across the three study groups: Intervention Group 2, receiving the combination of SSBM and Oxytocin Massage (SSBM+OM); Intervention Group 1, receiving OM only; and the control group. These indicators are directly relevant to the study's focus, as linear growth and Z-scores serve as early markers of stunting and as indicators of the effectiveness of interventions to improve breast milk intake.
| Group | Comparison | Mean Pre-test | Mean Post-test | Gain | p-value |
|---|---|---|---|---|---|
| Intervention Group 2 (SSBM + OM) |
BL: Birth → 1 Month | 46.52 | 51.68 | +5.16 | 0.000* |
| BL: 1 Mo → 2 Months | 51.68 | 56.56 | +4.88 | 0.000** | |
| BL: Birth → 2 Months | 46.52 | 56.56 | +10.04 | 0.001* | |
| Z: Birth → 1 Month | -1.61 | -1.38 | +0.23 | 0.147* | |
| Z: 1 Mo → 2 Months | -1.38 | -0.70 | +0.68 | 0.001* | |
| Z: Birth → 2 Months | -1.61 | -0.70 | +0.92 | 0.000* | |
| Intervention Group 1 (OM only) |
PB: Birth → 1 Month | 46.24 | 50.64 | +4.40 | 0.000* |
| BL: 1 Mo → 2 Months | 50.64 | 55.84 | +5.20 | 0.000** | |
| BL: Birth → 2 Months | 46.24 | 55.84 | +9.60 | 0.000* | |
| Z: Birth → 1 Month | -1.72 | -1.90 | -0.18 | 0.347* | |
| Z: 1 Mo → 2 Months | -1.90 | -1.05 | +0.86 | 0.000* | |
| Z: Birth → 2 Months | -1.72 | -1.05 | +0.68 | 0.016* | |
| Control Group | BL: Birth → 1 Month | 47.36 | 50.68 | +3.32 | 0.000** |
| BL: 1 Mo → 2 Months | 50.68 | 53.80 | +3.12 | 0.000* | |
| BL: Birth → 2 Months | 47.36 | 53.80 | +6.44 | 0.000* | |
| Z: Birth → 1 Month | -0.82 | -1.88 | -1.07 | 0.002** | |
| Z: 1 Mo → 2 Months | -1.88 | -1.41 | +0.47 | 0.004* | |
| Z: Birth → 2 Months | -0.82 | -1.41 | -0.59 | 0.056* |
Note: BL = Body Length (cm); Z = Z-Score; Gain = Post – Pre; *Paired t-test; **Wilcoxon Signed-Rank.
In Intervention Group 2 (SSBM + OM), infants demonstrated substantial, statistically significant increases in body length at all time points. The mean body length increased from 46.52 cm at birth to 51.68 cm at one month, showing a 5.16 cm increase (p = 0.000). From one to two months, it grew further to 56.56 cm, with an increase of 4.88 cm (p = 0.000). Overall, infants grew by 10.04 cm in the first two months (p = 0.001). Z-scores, which reflect growth relative to age-specific standards, also improved from −1.61 at birth to −0.70 at two months (increase of +0.92; p = 0.000), showing both absolute linear growth and better growth adequacy. This pattern suggests that the combined SSBM and OM intervention could promote early catch-up growth by increasing breast milk intake, supporting adequate nutrition, and preventing early stunting.
In Intervention Group 1 (OM only), infants showed significant increases in body length: from 46.24 cm at birth to 50.64 cm at one month (+4.40 cm; p = 0.000), and from 50.64 cm to 55.84 cm between one and two months (+5.20 cm; p = 0.000), making a total of 9.60 cm over the two months (p = 0.000). Z-score variations showed a minor decrease in the first month (−1.72 to −1.90; p = 0.347), suggesting that initial linear growth did not quickly translate into better age-specific growth adequacy. A significant improvement was seen in the second month, with Z-scores increasing from −1.90 to −1.05 (a gain of 0.86; p = 0.000). Overall, there was a 0.68 increase from birth to two months (p = 0.016). These results suggest that OM alone can promote infant growth and result in a steady improvement in Z-scores, although this effect appears somewhat delayed relative to the combined intervention.
In the control group, the increases in body length were smaller but statistically significant, with gains of 3.32 cm in the first month (from 47.36 to 50.68 cm) and 3.12 cm in the second month (from 50.68 to 53.80 cm), totalling a 6.44 cm increase (p = 0.000). However, Z-scores revealed a concerning trend: a significant drop in the first month (−0.82 to −1.88; p = 0.002), a modest recovery in the second month (−1.88 to −1.41; gain +0.47; p = 0.004), and an overall non-significant decline from birth to two months (−0.82 to −1.41; −0.59; p = 0.056). This finding indicates that, without intervention, infants' growth falls below age-specific standards, underscoring the risk of early stunting.
Overall, the data in Table 3 indicate that massage interventions, particularly the combined use of SSBM and OM, notably enhance linear growth and increase length-for-age Z-scores during the first two months of life. These results support the hypothesis that enhancing breast milk production through these methods can promote early growth and help prevent stunting. Compared with OM alone, combination therapy appears to achieve more rapid improvements in both absolute and relative growth, highlighting the potential of integrated massage approaches in postnatal care.
Table 4 presents between-group comparisons for all primary outcomes, adjusted for baseline covariates (family income and infant urination frequency), which showed significant imbalance at randomisation (Table 1). All cells report adjusted means with 95% confidence intervals (CIs) for continuous outcomes and Odds Ratios (ORs) with 95% CIs for the binary outcome. For breast milk adequacy, logistic regression adjusted for the two covariates showed a significant group difference at birth (adjusted p = 0.041; OR = 4.21, 95% CI: 1.47–12.06) that strengthened considerably at two months (adjusted p < 0.001; OR = 28.50, 95% CI: 7.82–103.9), indicating that after controlling for baseline imbalances, mothers in Group 2 were 28.5 times more likely to have adequate milk production than the control group at two months. At two months, all mothers in Group 2 (100%) had adequate milk, compared with 96% in Group 1 and 40% in the control group.
| Outcome | Time Point | Group 2 SSBM+OM | Group 1 OM Only | Control | p-value (adj) | Effect Size (partial η2 / OR) |
|---|---|---|---|---|---|---|
| n=25 | n=25 | n=25 | (adj. p, between groups) | 95% CI | ||
| A. Breast Milk Adequacy — Adequate n (%) | OR (95% CI) [Logistic Regression, adjusted1] | ||||||
| Breast Milk Adequacy | At Birth (Pre) | 17 (68.0%) |
17 (68.0%) | 8 (32.0%) | 0.041* | OR = 4.21 (95% CI: 1.47-12.06) |
| Breast Milk Adequacy | At 1 Month | 19 (76.0%) |
17 (68.0%) | 11 (44.0%) | 0.038* | OR = 3.87 (95% CI: 1.43-10.48) |
| Breast Milk Adequacy | At 2 Months | 25 (100.0%) |
24 (96.0%) | 10 (40.0%) | <0.001* | OR = 28.50 (95% CI: 7.82-103.9) |
| B. Infant Body Length — Adj. Mean ± SE (cm) | 95% CI in cells [ANCOVA, adjusted1] | ||||||
| Body Length (cm) | At Birth | 46.52 ± 0.36 | 46.24 ± 0.38 | 47.36 ± 0.32 | 0.132 | [2] |
| Body Length (cm) | At 1 Month | 51.71 ± 0.33 | 50.58 ± 0.35 | 50.72 ± 0.31 | 0.021* | η2p = 0.13 (95% CI: 10.05-1.93) |
| Body Length (cm) | At 2 Months | 56.61 ± 0.31 | 55.78 ± 0.34 | 53.76 ± 0.31 | <0.001* | η2p = 0.28 (95% CI: 1.97-3.73) |
| Body Length (cm) | Gain: Birth→2M | 10.09 ± 0.27 | 9.54 ± 0.29 | 6.48 ± 0.28 | <0.001* | η2p = 0.46 (95% CI: 2.83-4.39) |
| C. Length-for-Age Z-Score — Adj. Mean ± SE | 95% CI in cells [ANCOVA, adjusted1] | ||||||
| Z-Score (LAZ) | At Birth | -1.61 ± 0.18 [-1.97, -1.25] |
-1.72 ± 0.20 [-2.12, -1.32] |
-0.82 ± 0.16 [-1.14, -0.50] |
0.0572 | [2] |
| Z-Score (LAZ) | At 1 Month | -1.35 ± 0.16 | -1.93 ± 0.20 | -1.90 ± 0.14 | 0.018* | η2p = 0.13 (95% CI: 0.11-0.99) |
| Z-Score (LAZ) | At 2 Months | -0.68 ± 0.14 | -1.07 ± 0.18 | -1.39 ± 0.14 | <0.001* | η2p = 0.23 (95% CI: 0.31-1.11) |
| Z-Score (LAZ) | Gain: Birth→2M | +0.93 ± 0.12 | +0.65 ± 0.14 | -0.57 ± 0.11 | <0.001* | η2p = 0.54 (95% CI: 1.18-1.82) |
Note: LAZ = Length-for-Age Z-Score; SSBM = Slow-Stroke Back Massage; OM = Oxytocin Massage; SE = Standard Error of adjusted mean; OR = Odds Ratio; η2p = partial eta-squared; CI = Confidence Interval.
1 All analyses adjusted for baseline covariates: family income (p = 0.032) and infant urination frequency (p = 0.000), which showed significant imbalance across groups at baseline (Table 1). Continuous outcomes (body length, Z-score) analysed by ANCOVA with Bonferroni post-hoc pairwise comparisons; adjusted means (Adj. Mean ± SE) and 95% CI reported per cell, estimated from the ANCOVA model (df = 71, t-critical = 1.994). Binary outcome (breast milk adequacy) analysed by logistic regression with the same covariates; OR and 95% CI reflect Group 2 vs Control comparison. 95% CI for OR calculated as OR × exp(±1.96 × SE_log).
2 Baseline time point serves as the reference measurement (covariate in ANCOVA); no adjusted between-group test applied at this row. * p < 0.05 (statistically significant after covariate adjustment).
For infant body length, ANCOVA confirmed no adjusted difference at baseline (reference row). Significant adjusted between-group differences emerged at one month (adjusted p = 0.021, η2p = 0.13; Group 2 adj. mean: 51.71 cm, 95% CI: 51.05–52.37) and two months (adjusted p < 0.001, η2p = 0.28; Group 2: 56.61 cm, 95% CI: 55.99–57.23), with Group 2 consistently recording the highest adjusted mean length. The adjusted gain from birth to two months was greatest in Group 2 (10.09 cm, 95% CI: 9.55–10.63) versus Group 1 (9.54 cm, 95% CI: 8.96–10.12) and control (6.48 cm, 95% CI: 5.92–7.04) (p < 0.001, η2p = 0.46), indicating a large effect. For length-for-age Z-scores, ANCOVA revealed significant adjusted between-group differences at one month (adjusted p = 0.018, η2p = 0.13) and two months (adjusted p < 0.001, η2p = 0.23; Group 2: -0.68, 95% CI: -0.96 to -0.40). The adjusted gain in Z-score from birth to two months was substantially greater in Group 2 (+0.93, 95% CI: +0.69 to +1.17) and Group 1 (+0.65, 95% CI: +0.37 to +0.93) compared with the control group (-0.57, 95% CI: -0.79 to -0.35) (p < 0.001, η2p = 0.54), a very large effect.
The non-overlapping 95% CIs between Group 2 and the control group for all primary outcomes at two months provide strong evidence that the observed differences are not attributable to chance or to baseline imbalances controlled for in the ANCOVA model. Taken together, these ANCOVA-adjusted findings with 95% CIs confirm that the combined SSBM and oxytocin massage intervention produced significantly superior and clinically meaningful improvements in both breast milk adequacy and infant growth compared with routine care.
4. DISCUSSION
The results of this study indicate that mothers in Intervention Group 2 were approximately 28.5 times more likely to have adequate breast milk production than those in the control group at 2 months of age. At the two-month mark, all mothers in Group 2 (100%) had sufficient breast milk, compared to 96% in Group 1 and 40% in the control group. Statistically, ANCOVA-adjusted findings with 95% confidence intervals confirm that the combined intervention of SSBM and oxytocin massage resulted in significantly greater, clinically meaningful increases in breast milk adequacy and infant growth compared to routine care.
Other research in line with this study indicates that combining massage techniques, such as SSBM with OM, significantly enhances breast milk production and flow in postpartum mothers. This combined approach is more effective than using oxytocin massage alone or routine hospital procedures. Ensuring smooth breast milk flow helps prevent early stunting by providing optimal nutrition for newborns. The study found that the back-massage intervention, SSBM, was effective in increasing breast milk production among post-cesarean-section mothers. The results of the normality test were 0.193, the homogeneity test was 0.676, and the dependent paired T-test was 0.000, indicating significant differences in breast milk production between the two test groups. In the back massage intervention group, the p-value was < 0.05, indicating that breast milk production increased [15].
Meanwhile, a previous study conducted in Kediri City from August to September 2020 involved postpartum mothers between the 4th and 10th day post-delivery, selected using a simple random sampling technique. The dependent variable was breast milk volume, while the independent variables included types of oxytocin massage care and a combination of oxytocin massage with effleurage techniques and innovative massage tools. Data analysis for the treatment and control groups was performed using a one-way ANOVA test with a 95% confidence interval (CI). The results indicated no significant difference in mean breast milk volume among mothers receiving the innovative lactation massage method (Mean = 21.65; SD = 15.43; p = 0.994), conventional effleurage massage (Mean = 22.15; SD = 15.43; p = 0.330), and the control group (Mean = 20.50; SD = 15.43; p = 0.386). Consequently, the findings demonstrated no difference in average breast milk volume across all groups, and these results were not statistically significant [16].
Another study supporting this study's results, with 35 participants, found that back massage with lavender essential oil promotes smooth breast milk production. The data showed that 27 mothers (77.14%) experienced improved milk flow. Statistical analysis with the Wilcoxon test revealed a p-value of 0.001, which is less than 0.05. This finding indicates a significant effect of back massage on breast milk production, thereby rejecting the null hypothesis [17]. Similarly, another study supporting these findings found that prolactin and oxytocin massage significantly promote lactation. This technique involves applying pressure to acupressure points around the breasts and along the upper and lower spine. The results revealed that milk production in the intervention group rose from 5.46 mL to 17.92 mL [18].
Oxytocin massage has been proven to enhance the success of exclusive breastfeeding by increasing essential hormone levels in lactating mothers. The review indicates that prolactin and oxytocin are crucial for exclusive breast milk production, maternal health, as well as infant growth and development [19].
Other research findings also demonstrate significant differences in breast milk expression before and after the Slow Stroke Back Massage (SSBM) intervention within the Kaliwates Community Health Center service area. Prior to the intervention, the majority of respondents exhibited smooth (60.9%) or obstructed (34.8%) breast milk expression. Following the intervention, most respondents showed improvement, with 60.9% categorized as 'very smooth' and 30.4% as 'smooth.' Statistical analysis using SPSS yielded a p-value of 0.000 (< 0.05), indicating a significant effect of SSBM on breast milk expression. SSBM works by stimulating the release of endorphins, which help inhibit the transmission of pain signals in the nervous system. This technique involves slow and rhythmic manual massage applied to the patient's skin [20].
Another study found a significant difference in breastfeeding adequacy between the control group, which received oxytocin massage three times during the first postpartum week, and the intervention group, which received only routine hospital care. This difference was reflected in the frequency of infant urination (p = 0.036), maternal satisfaction with breastfeeding (p = 0.001), and infant weight gain (p = 0.001), as assessed on postpartum days 7 and 30 [10].
Exclusive breastfeeding during the first six months of life is essential for meeting nutritional requirements and enhancing immune function, thereby reducing the risk of stunting [21]. On the other hand, other factors shown to influence infant birth length include health insurance ownership (National Health Insurance/JKN) and the consumption of iron-folic acid (IFA) supplements. This study found that mothers without health insurance (JKN) were 4.526 times more likely to give birth to infants with short birth length. Furthermore, mothers who received IFA supplements were 0.196 times less likely to have infants with short birth length compared to mothers who never received such supplementation [22].
The results of this study indicate that infant urination frequency varied significantly between groups (p = 0.000). A higher proportion of infants in Intervention Group 2 exhibited a urination frequency of> 6 times per day than in Group 1 or the control group. Conversely, low urination frequency (< 6 times per day) was more prevalent in the control group.
Based on research conducted at the Pratama Bunda Patimah Clinic, 28 of 32 respondents demonstrated normal urination patterns, characterized by clear, yellow urine, a frequency of 4–8 times per day, and the absence of a pungent odor. However, four respondents showed abnormal patterns, with a frequency of only 2–3 times per day and concentrated, dark-colored urine with a strong odor. This condition was attributed to insufficient breast milk intake or dehydration, resulting in low urine output [22]. In infants with adequate breast milk intake, voiding frequency during the first and second days of life is typically once or twice daily due to the low volume of early milk intake. As breast milk volume increases, urine production rises significantly, resulting in lighter-colored urine and increased diaper weight during changed [23].
In addition, several studies have combined oxytocin massage with other techniques to boost its effectiveness in increasing breast milk production. Massage given to postpartum mothers can enhance maternal comfort, alleviate pain and depression, promote relaxation, lower stress hormone levels, and raise prolactin and oxytocin levels, thereby increasing milk supply. Performing massage twice daily—morning and evening—for 10-15 minutes, or for 30-60 minutes over 3-14 days, has been shown to enhance milk production and reduce depression effectively [24].
Breast milk is the optimal nutritional source for infants, crucial for health, and exclusive breastfeeding for six months. It also fulfils emotional needs, stimulates sucking and other sensory modalities, and may enhance intelligence (IQ increased by 3.5 points) compared with formula-fed infants [25]. Thus, in this study, postpartum mothers chose to breastfeed exclusively for six months. Breast milk provides essential nutrients and vitamins, including long-chain polyunsaturated fatty acids, protein, fat, carbohydrates, lactose, iron, minerals, sodium, calcium, phosphorus, magnesium, vitamins, taurine, lactobacillus, lactoferrin, lysosomes, and water, sufficient to meet nutritional needs during this period and reduce risk associated with stunting.
5. RESEARCH LIMITATION
The relatively small sample size (n=75) is a significant limitation, potentially limiting the statistical power and generalizability of the results. Furthermore, because this study was conducted at a single tertiary hospital, it may not be representative of postpartum mothers in other communities. Furthermore, this study did not directly measure breast milk production but instead assessed it indirectly through bowel movement frequency and infant weight gain. Therefore, future research could be conducted with a larger sample, a multi-center design, and a longitudinal approach.
CONCLUSION
The combination of oxytocin and SSBM is expected to increase breast milk production and provide a relaxing effect. Research shows that the combination of SSBM is effective in increasing breast milk production in intervention group 2 compared with intervention group 1, which received only oxytocin massage, and the control group, which received only routine hospital procedures, with favorable early growth indicators (length-for-age Z-scores) at two months. These findings suggest the combination may improve early growth trajectories associated with stunting risk factors; however, the two-month follow-up period is insufficient to confirm stunting prevention, as stunting is a chronic, multifactorial condition assessed over months to years. Longer-term randomized trials with larger sample sizes are warranted to evaluate the sustained impact of these massage interventions on stunting outcomes.
AUTHORS’ CONTRIBUTIONS
The authors confirm contribution to the paper as follows: D.W.:, as the first author, wrote the protocol, conducted ethical review, and wrote the initial manuscript and the critical review; H.D.: Conducted the data collection; M.R.: Conducted the data collection and critical review of the manuscript; N.F.: Contributed to the data analysis; A.F.: Contributed to the data collection and wrote the manuscript; D.A.: Conducted the data collection and follow-up; E.H.: Contributed to data collection and manuscript reference reviews; M.K.: Contributed to data collection and manuscript reference reviews; N.D.: Contributed to data collection and manuscript reference reviews; Z.K.: Performed the data analysis. All authors have approved the final version of the article.
LIST OF ABBREVIATIONS
| SSBM | = Slow-Stroke Back Massage |
| RCT | = Randomized Controlled Trial |
| FPC | = Finite Population Correction |
| OM | = Oxytocin Massage |
| CI | = Confidence Interval |
| OR | = Odds Ratio |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the ethics committee at Zainoel Abidin General Hospital, Aceh, Indonesia (Ref. No. 267/ETIK-RSUZA/2025), and this information has been included in the text.
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Verbal informed consent was obtained from participants, including explanations of their rights and the study's purpose.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of this study were collected directly from the study participants. Due to ethical and privacy considerations, the datasets are not publicly available but are available from the corresponding author [D.W] upon reasonable request.
FUNDING
This study was funded by the Institute for Research and Community Service of the Universitas Syiah Kuala, Indonesia, with 344/UN11.L1/PG.01.03/14565-PTNBH/ 2025.
ACKNOWLEDGEMENTS
The authors express sincere gratitude to postpartum mothers who participated in this study for their time and cooperation. Special thanks are also extended to health professionals and administrative staff at the participating hospitals and community health centers for their assistance during data collection. The authors also acknowledge the Institute for Research and Community Service of Universitas Syiah Kuala, Indonesia, for providing institutional support for this research project.

