All published articles of this journal are available on ScienceDirect.

Determinants of Electronic Nursing Documentation Adoption using an Integrated HOT-fit and Net Benefit Analysis: a path analysis
Abstract
Introduction
Electronic nursing documentation supports continuity of care, patient safety, and legal accountability, yet adoption remains inconsistent due to socio-technical barriers. Evidence is limited on how Human–Organization–Technology fit (HOT-fit) factors influence adoption through perceived Net Benefit. To examine determinants of electronic nursing documentation adoption using an integrated HOT-fit and perceived Net Benefit framework tested through path analysis.
Methods
A cross-sectional analytic study was conducted among 266 registered nurses from three hospitals in Indonesia. Eligible participants provided direct care or ward-level leadership and had used the electronic nursing documentation system (ENDS) for ≥6 months. Data were collected via a validated HOT-fit–based questionnaire assessing human, organizational, and technological factors, perceived Net Benefit, and adoption behavior (5-point Likert scale). Construct validity was evaluated using confirmatory factor analysis, followed by path analysis in AMOS.
Results
Human (β = 0.28), organizational (β = 0.34), and technological factors (β = 0.31) significantly predicted perceived Net Benefit (all p < .001). Perceived Net Benefit strongly predicted adoption behavior (β = 0.46, p < .001). HOT-fit domains also had significant direct effects on adoption (β = 0.12–0.18). Perceived Net Benefit partially mediated the effects of human (β = 0.13), organizational (β = 0.16), and technological factors (β = 0.14) on adoption (all p < .001). The model explained 62% of the variance in Net Benefit and 58% in adoption.
Discussion
The findings highlight that perceived Net Benefit plays a central mediating role in electronic nursing documentation adoption, indicating that nurses are more likely to use the system when they recognize its practical value in improving efficiency, safety, and workflow integration.
Conclusion
Adoption is primarily driven by perceived Net Benefit shaped by organizational support, usability, and human readiness, underscoring the need for leadership-enabled workflow optimization and competency-based training.
1. INTRODUCTION
Electronic nursing documentation has become a fundamental element of modern healthcare systems, supporting continuity of care, legal accountability, patient safety, and effective communication among healthcare professionals. The growing digital transformation of nursing records has been stimulated by the need for standardized documentation practices, immediate access to patient information, and improved coordination of care among multidisciplinary teams [1, 2]. For nurses, documentation in electronic systems represents more than a technological obligation; it is embedded within routine clinical activities and significantly affects workload distribution, workflow efficiency, and the overall quality of patient care.
Although these benefits are widely acknowledged, the implementation and use of electronic nursing documentation remain inconsistent across healthcare environments. Many nurses encounter obstacles such as limited system usability, an increased burden of documentation tasks, interruptions in clinical workflow, and insufficient institutional support [3, 4]. Complicated data-entry procedures, poorly designed interfaces, and inadequate alignment between digital systems and nursing practices often reduce acceptance and limit effective utilization [1]. These ongoing challenges indicate that the successful adoption of electronic documentation systems depends not only on their availability but also on how well they correspond to the professional needs of nurses and the organizational context in which they operate.
The Human–Organization–Technology fit (HOT-fit) framework offers a comprehensive socio-technical perspective for assessing the implementation of health information systems by emphasizing the interaction among human factors, organizational conditions, and technological attributes [2, 5]. Within nursing practice, studies evaluating health information systems using the HOT-fit framework have highlighted the importance of staff competence, leadership support, technological usability, and adequate infrastructure in facilitating successful system implementation [1, 6]. Nevertheless, much of the existing research has concentrated on system performance, implementation experiences, or user satisfaction, while comparatively little attention has been given to the sustained adoption of electronic documentation as part of everyday nursing workflows.
Human-related factors, including professional attitudes toward technology, informatics skills, and exposure to educational programs, play a substantial role in influencing nurses’ acceptance of electronic documentation systems [4]. Insufficient training during the implementation of electronic health records has been linked to lower staff well-being, increased stress, and a greater perception of potential clinical errors. Conversely, structured training initiatives can strengthen user confidence and support smoother integration of digital documentation into clinical routines [7]. Organizational aspects are also highly influential. Leadership commitment, clear governance structures, and supportive institutional culture have consistently been identified as essential contributors to successful EHR implementation [8]. In particular, supportive nursing leadership has been associated with greater engagement and higher utilization of digital documentation systems among nursing staff [9].
Technological features, especially system usability and compatibility with existing workflows, further influence adoption behavior. In acute care settings, the burden associated with documentation is strongly related to how well electronic systems correspond with nursing tasks and clinical processes [3]. Poorly designed systems may increase cognitive demands and contribute to professional burnout, highlighting the importance of user-centered design principles in health information technology [10]. Systems that reduce repetitive data entry, simplify documentation procedures, and provide dependable technical assistance tend to be used more consistently by nurses in daily clinical practice.
Another dimension that has received comparatively limited attention is the concept of perceived net benefit. This concept refers to the extent to which nurses perceive improvements in efficiency, documentation quality, patient safety, and coordination of care when using electronic systems. Observable advantages such as quicker access to clinical data, fewer documentation errors, and improved interdisciplinary communication can encourage continued use of electronic documentation tools [2, 3]. However, in many studies, net benefit is treated primarily as an outcome rather than as a mechanism that explains nurses’ adoption decisions. Emerging research indicates that perceived benefits are influenced by factors such as system–workflow compatibility, the adequacy of training, and leadership support [7, 8], suggesting that perceived net benefit may function as an important mediator within the adoption process.
Although the HOT-fit framework has been widely applied to evaluate hospital and nursing information systems, prior studies have largely relied on descriptive or cross-sectional designs focusing on implementation experiences, usability concerns, or user satisfaction [1, 2]. Empirical evidence specifically examining electronic nursing documentation adoption as a routine behavioral component of nursing practice remains limited, despite its central role in maintaining patient safety, ensuring continuity of care, and fulfilling legal documentation requirements. Furthermore, the mediating influence of perceived net benefit in connecting human, organizational, and technological factors with nurses’ adoption behavior has not been thoroughly investigated. Only a limited number of studies have employed analytical approaches such as path analysis to examine the complex relationships underlying nurses’ engagement with electronic documentation systems [10]. This gap is particularly significant for nursing managers and healthcare leaders responsible for enhancing workforce performance and advancing digital transformation initiatives. Without a comprehensive explanatory model, managerial strategies may overlook the key determinants that promote sustained use of electronic systems in clinical practice. Therefore, the present study aims to analyze the determinants of electronic nursing documentation adoption using an integrated HOT-fit and perceived net benefit framework through path analysis.
2. METHODS
2.1. Study Design and Setting
This study applied an analytic cross-sectional design to investigate factors associated with the adoption of electronic nursing documentation. The analysis was guided by an integrated framework combining the Human–Organization–Technology fit (HOT-fit) model and the concept of perceived Net Benefit, which was examined using path analysis. Data were collected from hospitals categorized as Type A, B, and C in Indonesia, representing varying levels of healthcare service capacity and complexity.
All participating hospitals had implemented electronic nursing documentation within their electronic health record (EHR) systems. The digital documentation platform had been routinely utilized for key nursing activities such as patient assessment, care planning, progress documentation, and handover reporting. Importantly, the system had been in operation for more than two years before the study was conducted, ensuring that nurses involved in the research had adequate familiarity and practical experience with the system.
2.2. Participants and Sampling
Eligible participants were registered nurses who met the following criteria: (1) actively provided direct patient care or held ward-level supervisory or leadership positions, (2) had used the electronic nursing documentation system (ENDS) for a minimum of six months, and (3) were willing to participate in the study. Nurses undergoing orientation programs, interns, student nurses, and personnel assigned to purely administrative roles were excluded. Staff members who were on extended leave during the study period were also not included.
A stratified consecutive sampling strategy was used to obtain representation from various inpatient clinical areas, including medical wards, surgical units, critical care units, and specialty departments. Nurse managers assisted in identifying eligible staff members during routine shift briefings. Participation was voluntary, and no incentives were provided.
The required sample size was estimated using G*Power version 3.1 for multiple regression analysis, which provides a conservative approximation for structural equation modelling (SEM) sample requirements [11]. Assuming a significance level of 0.05, statistical power of 0.80, and a medium effect size (f2 = 0.15), the minimum required sample was calculated to be 138 participants [12]. Considering the complexity of the proposed path model, including multiple predictors and mediation pathways, the target sample size was increased by approximately 90% to ensure adequate statistical stability and reliable estimation of indirect effects [13, 14]. Ultimately, 266 nurses completed the survey, exceeding the minimum requirement and providing sufficient statistical power for the SEM analysis.
2.3. Instrument
Data were gathered using a structured self-administered questionnaire developed based on the Human–Organization–Technology fit (HOT-fit) framework and the concept of Net Benefit. The measurement tool was adapted from previous studies examining nursing information systems using the HOT-fit model, particularly the mixed-methods investigation reported in the study [2], which demonstrated reliable assessment of human, organizational, technological, and system outcome dimensions.
The final questionnaire comprised five domains. Human-related factors were assessed using 12 items that measured attitudes toward digital technology, informatics skills, and the adequacy of training received. Organizational factors were represented by 10 items addressing leadership support, clarity of institutional policies, and organizational culture. Technological characteristics were evaluated through 12 items measuring system usability, reliability, quality of information generated by the system, and availability of technical support. Perceived Net Benefit was measured using eight items capturing perceived improvements in work efficiency, documentation accuracy, patient safety, and coordination of care. Adoption behavior was assessed with six items reflecting the routine use of electronic documentation within daily nursing workflows.
All questionnaire items were rated on a five-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree), with higher scores indicating stronger agreement with each construct.
The instrument was administered in Bahasa Indonesia. A forward–backward translation procedure was applied to maintain linguistic accuracy. Initially, two bilingual experts independently translated the questionnaire from English into Indonesian. Subsequently, a separate bilingual review panel performed back-translation into English to verify semantic equivalence. The translated version was reviewed by experts to ensure that terminology related to electronic documentation and nursing practice was culturally appropriate and aligned with the Indonesian clinical context.
Content validity was evaluated by a panel of five specialists in nursing informatics, nursing management, and clinical documentation. Revisions were made based on their feedback regarding clarity, relevance, and contextual suitability. Prior to the main study, the questionnaire was pilot-tested with 30 nurses to assess clarity of wording, feasibility of administration, and average completion time.
Internal consistency reliability in the main survey demonstrated acceptable to excellent levels across all constructs. Cronbach’s alpha values were 0.89 for human factors, 0.87 for organizational factors, 0.91 for technological factors, 0.88 for perceived Net Benefit, and 0.85 for adoption behavior. These reliability coefficients are comparable to those reported in previous studies employing the HOT-fit framework in nursing information system research [2].
2.4. Study Procedure and Ethics
Ethical approval for the study was granted by the Institutional Review Board of Universitas Hang Tuah Pekanbaru, Indonesia (Approval No. 562/KEPK/UHTP/ VIII/2025). Authorization to conduct the research was also obtained from the nursing management of the participating hospitals.
Prior to participation, eligible nurses received written information describing the objectives of the study, the voluntary nature of participation, procedures for maintaining confidentiality, and assurance that participation would not influence employment status. Informed consent was obtained from all participants.
Data collection took place between August and September 2025 using a secure online survey platform that could be accessed through a QR code. In addition to the structured questionnaire, participants were given the opportunity to provide optional written comments regarding perceived barriers and facilitators related to the use of electronic nursing documentation. These qualitative remarks were used descriptively to enrich the interpretation of the quantitative results.
2.5. Data Analysis
Prior to analysis, the dataset was screened for missing responses, extreme values, and distributional assumptions. Less than 5% of responses were missing and were addressed using mean substitution. Descriptive statistics were calculated to summarize participants’ demographic characteristics as well as the distribution of each study variable.
Construct validity of the measurement model was assessed through confirmatory factor analysis before testing the structural relationships among variables. Model fit was evaluated using several commonly recommended indices, including the Comparative Fit Index (CFI), Tucker–Lewis Index (TLI), Root Mean Square Error of Approximation (RMSEA), and Standardized Root Mean Square Residual (SRMR), in accordance with current structural equation modelling guidelines [15].
Convergent validity was examined using the Average Variance Extracted (AVE), while discriminant validity was assessed using the Fornell–Larcker criterion. After establishing measurement validity, path analysis was conducted to examine the hypothesized relationships among the HOT-fit components-human, organizational, and technological factors-perceived Net Benefit, and electronic documentation adoption behavior.
Both direct and indirect pathways were estimated in order to evaluate potential mediation effects. Indirect effects were tested using bias-corrected bootstrapping with 5,000 resamples, which is considered a robust approach for estimating mediation effects in structural equation models [13].
All statistical analyses were performed using AMOS version 26. Statistical significance was determined at a threshold of p < 0.05. Findings were reported as standardized path coefficients accompanied by 95% confidence intervals and explained variance values. Reporting of this study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
3. RESULTS
A total of 266 nurses completed the survey and were included in the analysis. Participants had a mean age of 36.81 years (SD = 6.68), suggesting that most respondents were in the mid-career stage of their professional development. Female nurses constituted the majority of the sample (80.8%). In terms of educational attainment, most respondents held a Bachelor of Nursing degree accompanied by professional Ners certification (67.2%). The majority of participants were employed in Type A hospitals (95.1%). Furthermore, most nurses reported that they had previously attended training or orientation sessions related to the use of electronic medical record (EMR) systems (86.4%). Detailed demographic information is presented in Table 1.
| Characteristic | n | % |
|---|---|---|
| Age (years), Mean ± SD | 36.81 ± 6.68 | |
| Gender | ||
| Female | 215 | 80.8 |
| Male | 51 | 19.2 |
| Education Level | ||
| Diploma in Nursing | 82 | 30.8 |
| Bachelor of Nursing and Ners | 179 | 67.3 |
| Other Health Degree | 5 | 1.9 |
| Hospital Type | ||
| Type A | 253 | 95.1 |
| Type B | 2 | 0.8 |
| Type C | 11 | 4.1 |
| Received EMR Training | ||
| Yes | 230 | 86.5 |
| No | 36 | 13.5 |
Descriptive statistics for the main constructs are presented in Table 2. Overall, nurses expressed moderately positive perceptions across all dimensions of the HOT-fit framework as well as the perceived Net Benefit construct. Among these variables, perceived Net Benefit recorded the highest mean value (M = 3.33, SD = 0.46), indicating that respondents generally recognized advantages of electronic documentation systems, particularly in relation to work efficiency, documentation quality, and patient safety. Human factors also showed relatively positive perceptions (M = 3.31, SD = 0.42), suggesting that many nurses reported favorable attitudes toward the system and felt reasonably competent in its use, although the variability observed implies that training experiences may not have been equally distributed.
| Construct | Mean |
Abbreviation: SD = Standard Deviation |
1 | 2 | 3 | 4 |
|---|---|---|---|---|---|---|
| 1. Human Factors | 3.31 | 0.42 | 1 | |||
| 2. Organizational Factors | 3.30 | 0.43 | 0.52 | 1 | ||
| 3. Technological Factors | 3.29 | 0.43 | 0.49 | 0.57 | 1 | |
| 4. Perceived Net Benefit | 3.33 | 0.46 | 0.55 | 0.60 | 0.63 | 1 |
Note: All correlations significant at p < 0.01 (2-tailed). Higher scores indicate stronger perceptions of each construct.
Organizational factors demonstrated a comparable mean score (M = 3.30, SD = 0.43), reflecting a generally supportive organizational environment, including leadership support and institutional policies, though variations across clinical units were apparent. Technological factors yielded a similar mean value (M = 3.29, SD = 0.43), indicating moderate levels of satisfaction with system usability, information reliability, and technical support. These findings suggest that while the system is broadly accepted, further optimization may be needed to better align the technology with clinical workflows.
Correlation analysis revealed moderate to strong positive relationships among the constructs. Each HOT-fit domain was positively associated with perceived Net Benefit, with correlation coefficients ranging from r = 0.55 to r = 0.63. This pattern suggests that higher levels of staff readiness, stronger organizational support, and better system usability were linked with stronger perceptions of the benefits derived from the electronic documentation system. Additionally, organizational and technological factors were strongly correlated (r = 0.57), indicating that institutional support and system performance may be closely interconnected in shaping user experience.
To assess the validity of the measurement model, confirmatory factor analysis (CFA) was conducted before examining the structural relationships among variables. The CFA results indicated that the measurement model demonstrated satisfactory fit to the data. The Comparative Fit Index (CFI) was 0.93, and the Tucker–Lewis Index (TLI) was 0.92, both exceeding the commonly recommended threshold of 0.90. In addition, the Root Mean Square Error of Approximation (RMSEA) was 0.056, suggesting an acceptable level of model approximation, while the Standardized Root Mean Square Residual (SRMR) was 0.048, reflecting a good correspondence between the observed and estimated covariance matrices. These indices indicate that the measurement model achieved an acceptable level of construct validity (Table 3).
| Fit Index | Recommended Cut-off | Obtained Value | Interpretation |
|---|---|---|---|
| CFI (Comparative Fit Index) | ≥ 0.90 | 0.93 | Good fit |
| TLI (Tucker–Lewis Index) | ≥ 0.90 | 0.92 | Good fit |
| RMSEA (Root Mean Square Error of Approximation) | ≤ 0.08 | 0.056 | Acceptable fit |
| SRMR (Standardized Root Mean Square Residual) | ≤ 0.08 | 0.048 | Good fit |
Note: Model fit was evaluated based on recommended structural equation modelling criteria (Xia & Yang, 2019). Values meeting or exceeding these thresholds indicate acceptable construct validity.
Convergent validity was supported for all constructs. Average variance extracted (AVE) values ranged from 0.54 to 0.60, exceeding the recommended threshold of 0.50. Composite reliability (CR) values were also satisfactory, all exceeding 0.86, which indicates strong internal consistency among the measurement items. Discriminant validity was evaluated using the Fornell–Larcker criterion. The square root of the AVE for each construct (0.73–0.77) was greater than the correlations with other constructs, confirming that each construct was empirically distinct (Table 4).
| Construct | CR | AVE | Human | Organization | Technology | Net Benefit | Adoption |
|---|---|---|---|---|---|---|---|
| Human Factors | 0.90 | 0.56 | 0.75 | 0.52 | 0.49 | 0.55 | 0.50 |
| Organizational Factors | 0.88 | 0.54 | 0.52 | 0.73 | 0.57 | 0.60 | 0.53 |
| Technological Factors | 0.91 | 0.58 | 0.49 | 0.57 | 0.76 | 0.63 | 0.58 |
| Perceived Net Benefit | 0.92 | 0.60 | 0.55 | 0.60 | 0.63 | 0.77 | 0.66 |
| Adoption Behavior | 0.86 | 0.55 | 0.50 | 0.53 | 0.58 | 0.66 | 0.74 |
Note: Values in bold on the diagonal represent the square root of AVE for each construct. Discriminant validity is supported when the square root of AVE is greater than the correlations with other constructs (Fornell–Larcker criterion). CR = composite reliability; AVE = average variance extracted.
Following validation of the measurement model, path analysis was performed to examine the structural relationships among the variables. Results indicated that human, organizational, and technological factors were all significant predictors of perceived Net Benefit, with standardized coefficients ranging from β = 0.28 to β = 0.34 (p < .001). Perceived Net Benefit, in turn, showed a strong positive effect on adoption behavior (β = 0.46, p < .001). In addition to these indirect pathways, each HOT-fit dimension also demonstrated significant direct effects on adoption behavior, suggesting that both perceived benefits and broader socio-technical conditions contribute to nurses’ use of electronic documentation systems (Table 5).
| Path | β | 95% CI | p-value |
|---|---|---|---|
| Human Factors → Net Benefit | 0.28 | 0.18 – 0.37 | < .001 |
| Organizational Factors → Net Benefit | 0.34 | 0.25 – 0.43 | < .001 |
| Technological Factors → Net Benefit | 0.31 | 0.22 – 0.40 | < .001 |
| Net Benefit → Adoption | 0.46 | 0.37 – 0.55 | < .001 |
| Human Factors → Adoption | 0.12 | 0.03 – 0.21 | .012 |
| Organizational Factors → Adoption | 0.18 | 0.09 – 0.27 | < .001 |
| Technological Factors → Adoption | 0.15 | 0.06 – 0.24 | .002 |
Note: Model Explained Variance (R2): Net Benefit = 0.62; Adoption Behavior = 0.58; β = standardized path coefficient; CI = confidence interval; All estimates were obtained using AMOS with bias-corrected bootstrapping (5,000 resamples).
The analysis also examined indirect relationships to determine whether perceived Net Benefit mediated the relationship between HOT-fit domains and adoption behavior. Results from the bootstrapping analysis showed that all three domains produced statistically significant indirect effects through perceived Net Benefit (β = 0.13–0.16, p < .001). These findings indicate partial mediation, suggesting that perceived system benefits function as an important mechanism through which human readiness, organizational support, and technological quality influence nurses’ adoption of electronic documentation (Table 6).
| Indirect Path | β | 95% CI | p-value | Mediation |
|---|---|---|---|---|
| Human → Net Benefit → Adoption | 0.13 | 0.07 – 0.20 | < .001 | Partial |
| Organizational → Net Benefit → Adoption | 0.16 | 0.10 – 0.23 | < .001 | Partial |
| Technological → Net Benefit → Adoption | 0.14 | 0.08 – 0.21 | < .001 | Partial |
Overall, the structural model indicates that human, organizational, and technological conditions contribute to the adoption of electronic nursing documentation both directly and indirectly through perceived Net Benefit. The model explained 62% of the variance in perceived Net Benefit and 58% of the variance in adoption behavior, demonstrating strong explanatory capacity (Fig. 1).
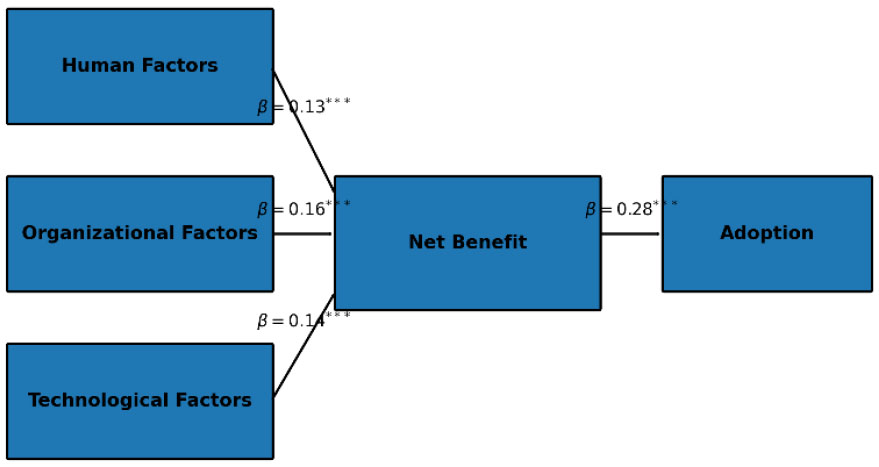
Structural path model illustrating the relationships between human, organizational, and technological factors, perceived Net Benefit, and electronic nursing documentation adoption. Standardized path coefficients (β) are presented. All displayed paths are statistically significant (p < 0.05).
4. DISCUSSION
This study explored factors associated with nurses’ adoption of electronic nursing documentation by integrating the Human–Organization–Technology fit (HOT-fit) framework with the concept of perceived Net Benefit in Indonesian hospitals. The results indicate that human, organizational, and technological conditions all contributed to nurses’ perceptions of the benefits generated by the system, and these perceived benefits were strongly linked to actual adoption behavior. In addition, perceived Net Benefit served as a partial mediator between the HOT-fit domains and documentation use, suggesting that nurses’ evaluation of the practical value of the system plays a central role in determining whether it becomes integrated into routine clinical practice [16].
Among the variables examined, perceived Net Benefit demonstrated the strongest direct relationship with adoption behavior (β = 0.46). This suggests that nurses are more inclined to consistently use electronic documentation when they clearly perceive improvements in work efficiency, quality of care, and patient safety outcomes. These findings are consistent with previous studies indicating that continued use of electronic health records is influenced by users’ experiences with system usability, workflow integration, and perceived benefits in clinical practice [10, 17]. Prior research has also shown that when digital systems are viewed as supporting workflow efficiency and lowering cognitive workload, healthcare professionals report lower levels of task burden and burnout [10]. In contrast, systems that are difficult to use or poorly aligned with clinical tasks can reduce user engagement even when the technological infrastructure is already available [18]. Taken together, these findings reinforce the importance of perceived Net Benefit as a key proximal factor influencing adoption.
Within the HOT-fit domains, organizational factors exerted the most substantial influence on perceived Net Benefit (β = 0.34). This indicates that leadership support, institutional policies, and the overall work environment shape how nurses interpret the usefulness and value of electronic documentation systems. Previous evidence has demonstrated that supportive nursing work environments are associated with higher levels of perceived EHR usability as well as improved nurse-reported quality of care [19]. Organizational readiness, including active managerial involvement and participatory implementation approaches, has also been linked to stronger acceptance of health information technologies among nurses [9]. Studies applying the HOT-fit model during nursing information system transitions similarly emphasize the importance of organizational alignment and institutional commitment in determining implementation success [2]. In the Indonesian healthcare context, where leadership structures often follow hierarchical patterns, organizational support may have an even stronger influence on nurses’ perceptions and technology use.
Technological characteristics also played an important role in shaping both perceived Net Benefit and adoption behavior. Elements such as system usability, reliability, and the availability of technical assistance were associated with how nurses evaluated the value of electronic documentation. Although respondents generally expressed moderate satisfaction with the system, the results suggest that improvements in workflow integration remain necessary. Previous research consistently indicates that poor usability in EHR systems can increase workload and contribute to professional burnout among healthcare workers [10]. When electronic documentation platforms do not align with everyday clinical processes, nurses may experience greater documentation burden and reduced efficiency. Qualitative studies further reveal that nurses often continue adapting to digital systems long after their initial implementation, and unresolved usability challenges may influence professional identity and the quality of care delivery [18]. For this reason, technological improvements should not focus solely on system functionality but also on reducing workflow interruptions and cognitive demands.
Human factors-including nurses’ competencies, attitudes toward digital systems, and exposure to training-were also found to influence both perceived Net Benefit and adoption behavior. However, their effects were relatively smaller compared with organizational and technological influences. This pattern suggests that although digital literacy and positive attitudes are important prerequisites, they alone may not guarantee sustained use of electronic documentation systems. The broader organizational environment appears to determine how effectively individual capabilities translate into routine practice. Evidence from previous research supports this view; for example, leadership style has been shown to significantly affect nurses’ acceptance of EHR technologies [9]. These findings imply that human readiness must be complemented by supportive institutional structures and system design.
The mediation analysis further confirmed that perceived Net Benefit partially explained the relationships between the HOT-fit components and adoption behavior. In other words, favorable human, organizational, and technological conditions promote system use not only directly but also by shaping nurses’ perceptions of the system’s value. From a methodological perspective, the structural model demonstrated acceptable fit according to widely recognized SEM criteria [15], indicating that the theoretical pathways proposed in this study are empirically supported. By explicitly examining adoption behavior rather than focusing solely on system satisfaction or implementation outcomes, the present findings extend earlier HOT-fit research in the context of nursing information systems [2, 19, 20].
4.1. Clinical Implication
Several practical implications emerge from these findings. First, hospital leadership should actively communicate the tangible benefits of electronic documentation systems by sharing performance indicators related to efficiency, documentation quality, and patient safety outcomes. Evidence suggests that positive work environments can strengthen nurses’ perceptions of EHR usability and contribute to better care quality [19]. Second, strengthening organizational support is essential. Leadership involvement, clear documentation policies, and participatory implementation strategies can enhance nurses’ perceptions of system value and facilitate adoption [2, 9]. Third, efforts to improve system usability should focus on aligning electronic documentation with existing clinical workflows and minimizing unnecessary documentation burden. Enhancing usability has been associated with reduced workload and lower levels of burnout among healthcare professionals [10]. Finally, training programs should remain an important component of implementation strategies. However, training alone may not be sufficient; it should be integrated with organizational support mechanisms and continuous system improvement to maximize its effectiveness.
5. STUDY LIMITATIONS
Several limitations should be considered when interpreting these results. The cross-sectional design restricts the ability to draw causal conclusions regarding the relationships between HOT-fit factors, perceived Net Benefit, and adoption behavior. In addition, the study relied on self-reported data, which may introduce response bias despite the acceptable validity and reliability of the measurement instruments. Although the sample included nurses from hospitals categorized as Type A, B, and C, most participants were employed in Type A hospitals. This distribution may limit the generalizability of the findings to smaller hospitals or settings with fewer resources. Participation was also voluntary, which may have introduced a degree of selection bias. Future research could address these limitations by employing longitudinal designs and incorporating objective system-use metrics to strengthen causal interpretation and measurement accuracy.
CONCLUSION
The findings of this study indicate that nurses’ use of electronic nursing documentation is strongly influenced by their perception of the system’s benefits. These perceptions are shaped by a combination of organizational support, technological usability, and individual readiness. Organizational factors emerged as the most influential predictor of perceived value, while perceived Net Benefit showed the strongest association with adoption behavior. These results highlight the importance of ensuring that digital health technologies are aligned with clinical workflows, supported by effective leadership, and capable of demonstrating clear improvements in performance outcomes. Strengthening these elements may support more sustainable adoption of electronic documentation systems in hospital environments. Future studies should consider longitudinal approaches and objective usage indicators to explore how adoption patterns evolve over time and to better understand the interaction between organizational, technological, and human factors across diverse healthcare settings. These findings should be interpreted within the limitations of cross-sectional design.
AUTHORS’ CONTRIBUTIONS
The authors confirm contribution to the paper as follows: S.M.S., F.M.S.: Study conception and design; S.M.S.: Data collection: S.M.S.: Analysis and interpretation of results; S.M.S, F.M.S.: Draft manuscript; S.M.S.: Critical revision of the manuscript; F.M.S. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| HOT-fit | = Human–Organization–Technology Fit |
| EHR | = Electronic Health Record |
| EMR | = Electronic Medical Record |
| SEM | = Structural Equation Modelling |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval was obtained from the Institutional Review Board of Universitas Hang Tuah Pekanbaru, Indonesia (Approval No. 562/KEPK/UHTP/VIII/2025).
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Written informed consent was obtained from all participants prior to their participation in the study. No identifiable personal information, photographs, audio, or video materials of participants are included in this manuscript.
AVAILABILITY OF DATA AND MATERIALS
The datasets generated and analyzed during the current study are available from the corresponding author [S.M.S] upon reasonable request. The data are not publicly available because they contain information that could compromise participant confidentiality.
ACKNOWLEDGEMENTS
The authors would like to thank the nursing management teams and all participating nurses from the involved hospitals for their valuable time, cooperation, and contributions to this research.

