All published articles of this journal are available on ScienceDirect.

Pathways Linking Self-Directed Learning, Self-Efficacy, and Clinical Competence in Nursing Students: A Cross-Sectional Study
Abstract
Background
Nursing education needs to support students not only in developing clinical performance but also in managing and directing their own learning. Self-directed learning (SDL) has been identified as a key factor associated with clinical competence. This study aimed to examine the mediating effect of self-efficacy on the relationship between SDL ability and clinical competence among nursing students.
Methods
The study was conducted with 138 nursing students who had clinical practice experience in general hospitals. Data were collected using validated instruments measuring SDL ability, clinical competence, and self-efficacy. Data were summarized descriptively, and associations among variables were examined using Pearson correlation coefficients. The mediation effect was tested using Hayes’ PROCESS macro (Model 4) and bootstrapped confidence intervals.
Results
Among the 138 participants, 73.9% were female, 77.5% were aged 20–24 years, and 51.4% were fourth-year students. Nearly half had more than 8 weeks of clinical practice experience (47.1%), and most reported satisfaction with clinical practice (71.0%). Clinical competence showed significant positive correlations with SDL ability (r = .44, p < .001) and self-efficacy (r = .46, p < .001). Self-efficacy partially mediated the relationship between SDL ability and clinical competence, and the indirect effect was statistically significant (indirect = 0.13, 95% CI: 0.05–0.32). The model's explanatory power increased from 20% to 29% when self-efficacy was included.
Discussion
The results suggest that self-efficacy is an important psychological mechanism linking SDL ability to clinical competence.
Conclusion
SDL ability had direct and indirect relationships with clinical competence, mediated by self-efficacy. Educational strategies should combine opportunities for independent learning with experiences that help students build confidence in clinical practice.
1. INTRODUCTION
As healthcare settings become more technologically advanced and patient care becomes increasingly complex, nursing graduates are expected to enter practice with stronger clinical readiness [1]. As a result, nurses are expected to apply theoretical knowledge, practical skills, and clinical judgment flexibly across varied care situations. Accordingly, nursing education has increasingly emphasized the development of learners’ autonomy and adaptability [2]. Clinical competence refers to the capacity to apply knowledge, skills, judgment, and professional attitudes appropriately in real clinical situations [3].
Previous studies have suggested that clinical competence is not solely acquired through exposure to clinical environments but is developed through active learning processes and reflective practice [4]. In this context, self-directed learning (SDL) has emerged as a critical factor in nursing education. SDL involves learners taking responsibility for identifying what they need to learn, choosing appropriate learning strategies, monitoring their progress, and evaluating the outcomes of their learning [5]. Students with stronger SDL ability are likely to participate more actively in academic programs and to report higher levels of competencies related to problem-solving and professional growth [6]. Self-efficacy is another psychological factor that may influence students’ learning and clinical performance. It reflects a person’s confidence in carrying out required actions successfully [7]. From the perspective of social cognitive theory, perceived capability affects how learners approach tasks, sustain effort, and perform in challenging situations. In nursing education, students with high self-efficacy tend to engage more confidently in clinical practice and achieve better outcomes [8].
However, empirical evidence on the mechanisms underlying the relationship between SDL and clinical competence remains limited. While previous studies have shown relationships among SDL, self-efficacy, and clinical competence, most have focused on direct associations [8]. Recent studies have also emphasized the importance of self-efficacy as a key psychological mechanism associated with clinical competence, skill performance, and academic outcomes among nursing students [9, 10]. Accordingly, this study explored how SDL ability is linked to clinical competence and whether self-efficacy explains part of this association.
2. METHODS
2.1. Study Design
This study used an observational cross-sectional design to examine whether self-efficacy explains the association between SDL ability and clinical competence. The manuscript was prepared in accordance with the STROBE guidelines for reporting research.
2.2. Participants and Data Collection
Participants were nursing students who had completed clinical practice in general hospitals and voluntarily agreed to take part after receiving information about the study's purpose and procedures. The clinical practice sites were general hospitals located in Daegu and Gyeongbuk, South Korea. These hospitals were accredited as suitable institutions for clinical practice education for nursing students and had at least 300 beds. The inclusion criteria were as follows: nursing students who were enrolled in a nursing program, had completed clinical practice in a general hospital, understood the purpose of the study, and voluntarily agreed to participate. Students were excluded if they had no clinical practice experience. The required sample size was estimated using G*Power 3.1.9.2. For a multiple regression analysis with 10 predictors, a significance level of .05, statistical power of .85, and a medium effect size of .15 were used. This calculation indicated that at least 131 participants were needed. To allow for an anticipated dropout rate of approximately 10%, 146 students were recruited. After excluding incomplete responses, the final analysis included data from 138 participants. Data were collected from July 10, 2021, to September 15, 2021, using a web-based questionnaire. Recruitment notices containing QR codes were posted for nursing students participating in clinical practice as part of the curriculum at hospitals. Students who accessed the survey through the QR code first reviewed the study explanation and eligibility criteria. Only those who provided informed consent were able to proceed to the questionnaire.
2.3. Measures
2.3.1. Self-directed Learning Ability
SDL ability was assessed using a scale developed by Bae and Lee [11]. This 21-item instrument evaluates seven aspects of SDL ability, including learning motivation, self-concept, management of learning processes, outcome evaluation, continuity of learning, resource use, and creation of learning environments. In this study, the total mean score was used to represent overall SDL ability, rather than analyzing each subdimension separately. Higher scores indicate greater SDL ability. Each item is rated on a 5-point Likert scale ranging from 1 to 5, with higher scores meaning greater SDL ability. The Cronbach’s α was 0.88 in the study.
2.3.2. Clinical Competence
Clinical competence was assessed using the Clinical Competence Tool developed by Kun-Ja et al. [12]. The tool includes 16 questions covering assessment, diagnosis and planning, implementation, evaluation, and professional attitude. Scores are rated on a 5-point Likert scale, with higher scores indicating higher levels of clinical competence. The Cronbach’s α in this study was 0.94.
2.3.3. Self-efficacy
Self-efficacy was measured using the instrument developed by Sherer et al. [13], with the Korean version translated and adapted by Park et al. [14]. This scale includes 23 items covering both general and social aspects of self-efficacy. Responses are scored on a 5-point Likert scale, and higher total scores indicate a higher level of perceived self-efficacy. In the present study, Cronbach’s α was 0.87.
2.4. Data Analysis
All statistical analyses were performed using IBM SPSS Statistics version 24.0 (IBM Corp., Armonk, NY, USA). Participant characteristics and study variables were summarized using descriptive statistics, including means, standard deviations, frequencies, and percentages. Differences in clinical competence according to participants’ characteristics were identified using independent t-tests and one-way analysis of variance (ANOVA). Data normality was evaluated based on skewness and kurtosis. Pearson’s correlation analysis was conducted to examine the relationships among SDL ability, self-efficacy, and clinical competence. The mediation model was analyzed using Hayes’ PROCESS macro Model 4 [15, 16]. A bootstrapping procedure with 5,000 replications was used to estimate the indirect effect. The mediating effect was considered significant when 0 was not included in the 95% bias-corrected confidence interval.
2.5. Ethical Considerations
This study was reviewed and approved by the Institutional Review Board of Keimyung University (protocol code 202105-016-001). Prior to participation, all students were provided with an explanation of the study purpose, procedures, the voluntary nature of participation, and their rights as participants. Written informed consent was obtained before data collection began. Participants were informed that the collected data would be used only for research purposes and that their personal information would remain confidential. They were also assured that they could withdraw from the study at any time without penalty or disadvantage. As a token of appreciation, participants received a small mobile beverage coupon after participation.
3. RESULTS
3.1. Clinical Competence of Participants’ Characteristics
The demographic and practice-related characteristics of the participants are presented in Table 1. No significant differences in clinical competence were found according to gender, age, grade, clinical practice duration, or satisfaction with clinical practice; therefore, these variables were not included as covariates in the mediation analysis.
| Variables | Categories | N (%) | Clinical Competence | ||
|---|---|---|---|---|---|
| M±SD | t/F (p) | ||||
| Gender | Female | 102(73.9) | 3.55±0.83 | 1.66(.082) | |
| male | 36(26.1) | 3.21±0.46 | - | ||
| Age (years) | 20-24 | 107(77.5) | 3.43±0.78 | 0.57(.676) | |
| 25-29 | 31(22.5) | 3.39±0.96 | - | ||
| Grade | 3rd | 67(48.6) | 3.41±0.81 | 1.24(.361) | |
| 4th | 71(51.4) | 3.53±0.96 | - | ||
| Clinical practice period (weeks) | 4> | 31(22.5) | 3.41±1.01 | 1.79(.201) | |
| 4-8 | 42(30.4) | 3.48±0.83 | - | ||
| 8< | 65(47.1) | 3.45±0.66 | - | ||
| Clinical practice satisfaction | Satisfaction | 98(71.0) | 3.52±0.42 | 2.21(.114) | |
| Moderate | 33(23.9) | 3.46±0.83 | - | ||
| Dissatisfaction | 7(5.1) | 3.27±0.96 | - | ||
3.2. Descriptive Statistics of SDL Ability, Clinical Competence, and Self-efficacy
The SDL ability’s mean score was 3.53 ± 0.68, clinical competence’s score was 3.47 ± 0.51, and self-efficacy was 3.29 ± 0.82. Skewness ranged from 0.02 to 0.21, and kurtosis ranged from −0.21 to 0.38, showing that all variables met the assumption of normality (Table 2).
| Variables | Range | M±SD | Min | Max | Skewness | Kurtosis |
|---|---|---|---|---|---|---|
| SDL ability | 1-5 | 3.53±0.68 | 2.42 | 5 | 0.05 | 0.01 |
| Clinical competence | 1-5 | 3.47±0.51 | 1 | 5 | 0.21 | 0.38 |
| Self-efficacy | 1-5 | 3.29±0.82 | 1.28 | 5 | 0.02 | -0.21 |
3.3. Correlation between Subjects' SDL Ability, Clinical Competence, and Self-efficacy
Clinical competence was positively correlated with SDL ability (r = .44, p < .001) and self-efficacy (r = .46, p < .001). SDL ability was also positively correlated with self-efficacy (r = .37, p < .001) (Table 3).
| Variables | SDL Ability | Clinical Competence | Self-efficacy |
|---|---|---|---|
| r(p) | |||
| SDL ability | 1 | - | - |
| Clinical competence | .44(<.001) | 1 | - |
| Self-efficacy | .37(<.001) | .46(<.001) | 1 |
3.4. The Mediating Effect of Self-efficacy on the Relationship between SDL Ability and Clinical Competence
Mediation analysis was conducted using Hayes’ PROCESS macro Model 4 [16]. As shown in Figure 1, SDL ability had a significant positive effect on self-efficacy (β = .37, p < .001). SDL ability also had a significant total effect on clinical competence (β = .44, p < .001). When both SDL ability and self-efficacy were included in the model, self-efficacy remained a significant predictor of clinical competence (β = .32, p < .001), and the direct effect of SDL ability on clinical competence remained significant but decreased (β = .33, p < .001). This pattern indicates a partial mediating effect of self-efficacy. The model's explanatory power increased from 20% to 29% after self-efficacy was included. The detailed mediation results are presented in Table 4.
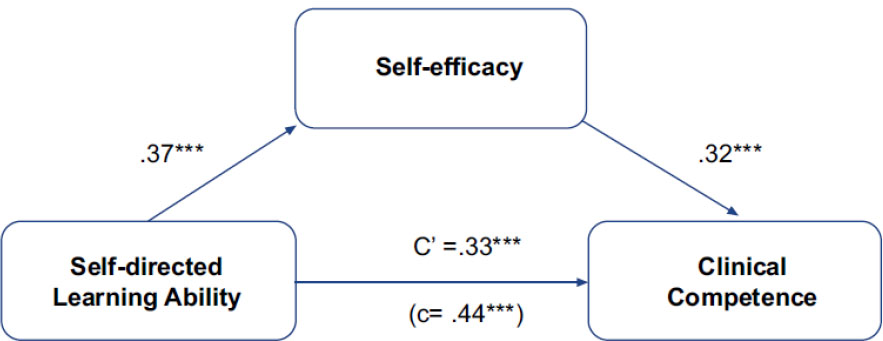
Conceptual mediation pathway from SDL ability to clinical competence through self-efficacy.
Note: Values are standard coefficients (β). Path c is the total effect; path c' is the direct effect. Indirect effect 0.13, 95% confidence interval [.05, .32], ***p<.001.
| Model | Variables | B | β | t(p) | R2 | F(p) |
|---|---|---|---|---|---|---|
| Model 1 | SDL ability → Self-efficacy | .41 | .37 | 4.50(<.001) | .14 | 17.13(<.001) |
| Model 2 | SDL ability → Clinical competence | .45 | .44 | 5.42(<.001) | .20 | 20.48(<.001) |
| Model 3 | SDL ability → Clinical competence | .34 | .33 | 3.88(<.001) | .29 | 19.52(<.001) |
| Self-efficacy → Clinical competence | .31 | .32 | 4.21(<.001) | |||
| Effect decomposition | Effect | Boot SE | 95% CI | |||
| SDL → Self-efficacy → Clinical competence | 0.13 | .041 | .05 to .32 | |||
4. DISCUSSION
This study examined the relationships among SDL ability, self-efficacy, and clinical competence among nursing students, with a focus on the mediating effect of self-efficacy. The findings showed that SDL ability was positively associated with both self-efficacy and clinical competence, and that self-efficacy partially mediated the relationship between SDL ability and clinical competence. These results suggest that clinical competence may be influenced not only by students’ ability to manage their own learning but also by their confidence in applying nursing knowledge and skills in clinical situations [3, 4, 17].
SDL ability was significantly related to clinical competence. This finding is consistent with previous studies showing that SDL is an important factor in nursing students’ learning outcomes, clinical performance, and readiness for professional practice [2, 5, 6, 8, 11, 18]. A possible reason for this consistency is that clinical practice requires students to identify their learning needs, seek relevant information, connect theoretical knowledge with patient care, and reflect on their own clinical experiences. Students with high SDL ability may be more likely to prepare actively for clinical practice, use feedback, and evaluate their performance. These learning behaviors may help them respond more effectively to complex and changing clinical situations.
Self-efficacy was also positively associated with clinical competence. Students who have confidence in their ability to perform clinical tasks may participate more actively in practice, persist when facing difficulties, and apply learned skills more effectively. This finding is consistent with social cognitive theory, which emphasizes the role of perceived capability in motivation, effort, persistence, and performance [19]. It is also supported by previous studies reporting that self-efficacy is closely related to nursing students’ clinical competence, clinical learning experiences, and skill performance [7, 9, 10, 17]. Therefore, self-efficacy should be considered an important psychological factor supporting clinical competence in nursing students [7, 9, 17].
The partial mediating effect of self-efficacy indicates that SDL ability is linked to clinical competence both directly and indirectly. Students who manage their learning effectively may gain successful learning experiences through goal setting, self-monitoring, feedback use, and reflection. These experiences may strengthen their confidence and contribute to better clinical performance. This finding extends previous studies by showing a possible pathway through which SDL contributes to clinical competence [8, 10, 17, 20, 21]. In other words, SDL may be associated with clinical competence not only through students’ independent learning behaviors but also through enhanced beliefs that they can successfully perform clinical tasks. The finding that self-efficacy had a partial, rather than complete, mediating effect also requires interpretation. SDL ability continued to have a direct effect on clinical competence even after self-efficacy was included in the model. This may be because SDL abilities include practical learning behaviors, such as resource use, learning management, and outcome evaluation, which can directly support clinical competence regardless of students’ confidence levels. In addition, clinical competence may be influenced by other factors, including the clinical learning environment, quality of supervision, opportunities for hands-on practice, and time management skills [17, 22]. Therefore, self-efficacy appears to be an important but not exclusive mechanism explaining the relationship between SDL ability and clinical competence. However, SDL ability alone may not always lead to higher clinical competence, particularly when students have limited opportunities for hands-on practice, insufficient supervision, or an unsupportive clinical learning environment. This suggests that the relationship between SDL ability and clinical competence may depend on students' ability to translate autonomous learning into confident clinical action. In this context, self-efficacy may serve as a psychological bridge that helps students apply what they have learned in uncertain or unfamiliar clinical situations.
These results have practical implications for nursing education. Educational programs should not focus only on promoting autonomous learning but should also help students build confidence in clinical practice. Strategies such as goal setting, reflection, self-assessment, simulation-based learning, repeated skills practice, constructive feedback, and supportive clinical supervision may help students strengthen both SDL ability and self-efficacy [10, 19, 21]. In particular, educators and clinical preceptors should provide students with opportunities for successful performance experiences and specific feedback, because these experiences may help students translate autonomous learning into competent clinical practice. Additionally, clinical competence did not differ significantly across participants’ general characteristics, suggesting that learning-related factors may be more important than demographic characteristics or clinical exposure alone [4, 22, 23]. Although some previous studies have emphasized the influence of clinical exposure or educational experience on competence, the present result may be explained by the participants' relatively similar educational backgrounds, all of whom had completed clinical practice in general hospitals. Therefore, simply increasing clinical practice experience may not be sufficient unless students are also supported to engage actively in learning and to develop confidence in performing clinical tasks. Local nursing associations may also support students by connecting them with experienced clinical nurse mentors and providing structured mentorship opportunities.
This study has some limitations. Because of the cross-sectional design, causal relationships among SDL ability, self-efficacy, and clinical competence cannot be confirmed. The use of convenience sampling and self-reported questionnaires may also limit the generalizability and objectivity of the findings. Future studies should use longitudinal or experimental designs and include objective measures of clinical performance to further examine these relationships [22, 24-26]. In addition, future research should consider other contextual factors, such as clinical learning environment, preceptor support, simulation experience, and academic motivation, to provide a more comprehensive understanding of clinical competence development.
In conclusion, the study highlights the potential role of self-efficacy as a psychological mechanism linking SDL ability to clinical competence. Nursing education may be more effective when it supports both students’ autonomous learning and their confidence in performing clinical tasks. Such an approach may help nursing students develop the competence needed for complex clinical environments [8, 10, 17, 26].
CONCLUSION
This study identified significant associations among SDL ability, self-efficacy, and clinical competence in nursing students. In particular, self-efficacy partially mediated the relationship between SDL ability and clinical competence, indicating that students’ confidence in their ability to perform clinical tasks may help explain how SDL contributes to clinical competence.
These findings suggest that nursing education should support not only students’ independent learning behaviors but also the development of confidence in applying knowledge and skills in clinical settings. Educational strategies that encourage goal setting, reflection, active participation, and self-monitoring may strengthen SDL ability. At the same time, learning experiences that provide repeated practice, constructive feedback, simulation-based training, and successful clinical experiences may help enhance students’ self-efficacy.
Therefore, nursing curricula may benefit from an integrated educational approach that links autonomous learning with confidence-building experiences. Such an approach may help students translate what they learn into competent clinical performance. Given the cross-sectional design and self-reported data in this study, longitudinal or experimental studies are needed to confirm causal relationships and to examine whether educational interventions targeting both SDL and self-efficacy can improve clinical competence in the future.
AUTHOR’S CONTRIBUTIONS
The author confirms sole responsibility for the following: study conception and design, data collection, analysis and interpretation of results, and manuscript preparation.
LIST OF ABBREVIATIONS
| SDL | = Self-directed learning |
| CI | = Confidence interval |
| ANOVA | = Analysis of variance |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Institutional Review Board (IRB) of Keimyung University, Republic of Korea (Approval Reference Number: 202105-016-001).
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
DATA AVAILABILITY STATEMENT
The data supporting the findings of the article is available from the corresponding author [H.Y.K] upon reasonable request.
ACKNOWLEDGEMENTS
Declared none.

