All published articles of this journal are available on ScienceDirect.

Effect of Utilizing Health Belief Model on Knowledge, Beliefs, and Behaviour of Visually Impaired Women toward Breast Self-examination
Authors Info & Affiliations
Abstract
Background:
Breast self-examination is the most important first step in early breast cancer detection. The study aimed to measure the effectiveness of utilizing a health belief model on knowledge, beliefs, and behaviour of visually impaired women toward breast self-examination.
Methods:
A quasi-experimental design (pre/posttest) was utilized in the current study conducted at Al Nour Wal Amal Association for visually impaired women in Cairo governorate, Egypt. A purposive sample of 42 visually impaired women was included in the study. Three tools were used for the purpose of data collection, namely (I): Structured interviewing knowledge questionnaire, (II): A breast self-examination checklist, and (III): Health beliefs assessment scale.
Results:
The findings revealed a highly statistically significant difference in visually impaired women's total knowledge, total practice, and total health beliefs scores for breast self-examination before and after the program. The women's total knowledge, behaviors, and beliefs improved in the posttest compared to the pretest.
Conclusion:
The study results concluded that there was an improvement in knowledge, practice, and health beliefs regarding breast self-examination among visually impaired women after program implementation, which emphasized that educational programs based on the health beliefs model have a significant positive effect in improving women’s knowledge, practice, and health beliefs toward breast self-examination. It is recommended to establish educational programs to raise awareness about breast cancer and breast self-examination among visually impaired women through special schools and community associations. Moreover, community health nurses play a crucial role in educating women about breast self-examination as they are in a unique position to raise breast cancer awareness, especially among at-risk groups.
1. INTRODUCTION
Breast cancer is the most common cancer in both developed and developing countries, and it is the world's second leading cause of death. Over one million new instances of breast cancer are diagnosed each year around the world, resulting in more than 600,000 deaths [1]. One in every eight women worldwide is diagnosed with breast cancer, accounting for 12% of new cancer cases and 25% of all cancers in women. Breast cancer affects roughly 1.7 million women worldwide each year. As a result, breast cancer is the leading cause of cancer-related death and morbidity among women [2].
Breast cancer screening is critical for early detection and lowering mortality rates. Mammography, clinical breast examination, and breast self-examination (BSE) are all suggested screening methods for early breast cancer detection. Annual mammography screening is the most efficient way to detect cancers before symptoms occur and receive fast and successful treatment [3]. Regular BSE has been proposed as part of a broader health promotion strategy; nevertheless, BSE is dependent on women's understanding and attitudes toward BSE practice. Its effectiveness is determined by the healthcare providers' abilities and the facilities provided. For younger and high-risk women, it offers a straightforward, non-invasive, affordable, and accessible means of detecting early alterations and abnormalities in their breasts [4].
Women's attitudes toward health promotion actions are heavily influenced by their views about health. One of the most well-studied educational frameworks in health education is the health belief model, and it is commonly utilized in research studies aimed at predicting health behaviours and recognizing preventive actions to diagnose breast cancer early [5]. There are six domains in the health belief model that deal with behaviours. It comprises factors, such as perceived severity, susceptibility, perceived benefits and barriers, cues to action, and self-efficacy [6, 7].
Educational information on BSE is readily available in different forms, such as written, videos, or pamphlets where women can benefit from it at any time. However, one segment of women is completely underserved by these available materials because of their special needs from visual impairment. The prevalence of blindness among adults aged 50 and up in Egypt is estimated to be 7.9 percent. Women are 1.68 times more likely to have impaired vision. The best method for early detection is BSE, where the practice of a breast model and pamphlet using the Braille method are the best instructional methods for BSE, from which visually impaired women could benefit [8].
The core functions and roles of the community health nurse are to promote, maintain, and restore the health of the entire population, so nursing interventions increase their knowledge, early detection of breast cancer, and disease progression prevention, where proper instructions about the correct technique of BSE will increase their awareness and skills to carrying out this particular task and overcome the barriers of practice. When a woman is informed about BSE, she gains more understanding and confidence and is more likely to use it often [9].
1.1. Significance of the Study
Breast cancer is a serious health problem in Egypt, affecting 35.1% of women. However, the prevalence of visual impairment or loss (11.8%) makes it challenging to detect any abnormal changes in their breast. Recent research has indicated that it is critical to raise awareness among women, particularly those who are visually impaired, about the risks of breast cancer and the need for early detection. Inadequate educational programs about breast health awareness may have contributed to this lack of knowledge [10].
Early detection of breast abnormalities helps to reduce the fatal repercussions of this disease, especially among women who are visually impaired. The Health Belief Model is one of the models that can effectively improve women's understanding, change harmful habits, and boost early breast cancer prevention activities [11]. As a result, the researchers decided to perform the study to evaluate the effectiveness of utilizing the health beliefs model in improving knowledge, beliefs, and behaviour of visually impaired women toward breast self-examination practice.
1.2. Theoretical Framework
The Health Belief Model (HBM) served as the theoretical framework for this research. The social psychologists Godfrey Hochbaum and Irwin Rosenstock first established this model in the 1950s. Threats, together with an individual's knowledge and beliefs of susceptibility, severity, and self-efficacy, are essential elements in predicting participation in preventive measures [11, 12] (Figs. 1 and 2).
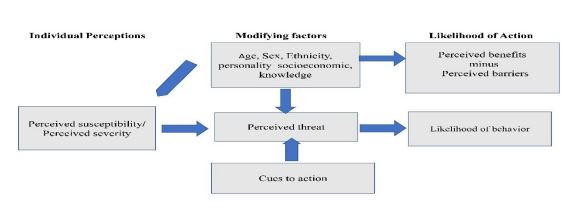
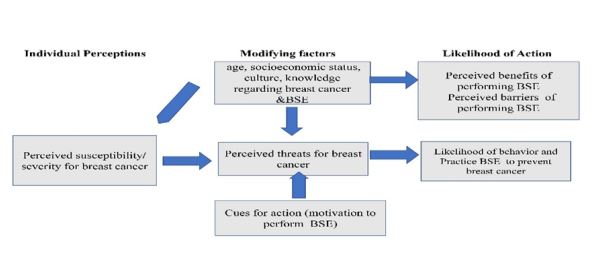
In this study, the Health Belief Model was used to address the issue of reducing the occurrence/early detection of breast cancer for visually impaired women through (a) increasing their awareness of breast self-examination, (b) informing them about the susceptibility to breast cancer, (c) informing them about the severity/seriousness of breast cancer, (d) making them aware of the benefits of breast self-examination, (e) identifying barriers to breast self-examination, and (f) examining cues to breast self-examination.
According to HBM, visually impaired women who believe they are vulnerable to a specific disease (breast cancer) or believe the disease has progressed to a dangerous stage are more likely to engage in breast cancer screening behaviours. The BSE is still regarded as a straightforward, non-invasive, inexpensive, affordable, and accessible tool for women who are younger and at a high risk of breast cancer to detect early changes in their breasts among breast cancer screening tests. The HBM was used as a theoretical foundation in this study to investigate variables that influence BSE behavioursur in visually impaired women.
1.2.1. Perceived Susceptibility
Visually impaired women believe that they are susceptible to breast cancer when they do not practice preventive actions (avoid predisposing factors, not practicing breast self-examination for early detection and management).
1.2.2. Perceived Severity of Breast Cancer
Knowledge and beliefs of the consequences of breast cancer and its threatening consequences on their life (breast cancer requires lifelong management for complications of treatment, increased morbidity and mortality, and the psychosocial burden on women and their families).
1.2.3. Perceived Benefits
Of breast self-examination include early detection of breast cancer, early diagnosis and treatment, decreased complications, and a decreased bio-psychosocial burden on the woman and her family.
1.2.4. Perceived Barriers
To breast self-examination: Identifying the factors that prevent them from practicing the BSE to prevent breast cancer as they are visually impaired; it is embarrassing for women to do monthly BSE; doing BSE increases women’s anxiety and fear, and BSE can be painful and time-consuming.
1.3. Aim of the Study
The aim of this study was to evaluate the effectiveness of utilizing a health belief model in the knowledge, beliefs, and behaviour of visually impaired women toward breast self-examination.
1.4. Research Hypotheses
To achieve the aim of the study, the following research hypotheses were formulated:
1.4.1. H.1
Visually impaired women who will receive the health education program will have higher knowledge scores regarding breast self-examination after implementation of the program.
2. MATERIALS AND METHODS
2.2. Setting
The study was conducted at the Al Nour Wal Amal Association (ANWA) for visually impaired women in Cairo governorate, Egypt. It is a non-profit organization established in 1954 by a group of volunteer women as the first centre in Egypt and the Middle East for the care, education, vocational training, and social integration of blind girls and women into society. Al Nour Wal Amal Association aims to establish the rights of blind girls and women by providing them with education, boarding facilities, literacy programs in Braille, and vocational training in order to develop their potential and special abilities, ensuring their physical and psychological health and allowing them to develop their own identities to become self-dependent, integrated members of society.
2.3. Sample
A purposive sample of 42 visually impaired women was included in this study according to visually impaired women’s following inclusion criteria, involving age from 18 years old and above, married or single females, and willing to participate in the study.
2.4. Tools for Data Collection
The study tools were created by the researchers based on an exhaustive examination of the associated literature to collect data relevant to the current study.
A structured interviewing knowledge questionnaire has two parts:
Part 1: Demographic data. It includes women’s age, marital status, educational level, place of residence, occupation, and family income.
Part 2: Pre/post-knowledge questionnaire to assess women’s knowledge regarding breast cancer and breast self-examination.
Total knowledge scores are classified as follows: a poor level of knowledge is < 60% with a total score of less than 23 points, a fair level of knowledge ranges from 60% to 75% with a total score of 23 to 28 points, and a good level of knowledge is >75% with a total score of more than 28 points.
Breast self-examination checklist: a checklist regarding the steps of BSE performance.
Total practice scores are classified as follows: a poor level of practice is < 60% with a total score of less than 4 points, a fair level of practice ranges from 60% to 75% with a total score of 4 to 5 points, and a good level of practice is > 75% with a total score of more than 5 points.
The Health Beliefs Assessment Scale:
After analyzing the literature, the researchers created a health beliefs assessment tool to measure visually impaired women's health beliefs about breast self-examination. It is based on the Champion's Health Belief Model (CHBM), which consists of five basic constructs with 28 items. The tool is classified into five parts according to the five constructs of CHBM.
Part 1: Five questions related to perceived susceptibility to breast cancer.
Part 2: Six questions related to the perceived severity/seriousness of breast cancer.
Part 3: Five questions related to perceived benefits of breast self-examination.
Part 4: Six questions related to perceived barriers to breast self-examination.
Part 5: Six questions related to cues for breast cancer prevention.
The five categories were assessed on a 5-point Likert scale ranging from 1 strongly disagree, disagree, neutral, agree to 5 strongly agree, with the exception of the barriers scale, which was scored as 5 strongly disagree, 4 disagree, 3 neutral, 2 agree to 1 strongly agree.
Total belief scores are classified as follows: negative belief is <60% with a total score of less than 84 points, and positive belief is ≥ 60% with a total score of more than or equal to 84 points.
2.5. Tool Validity
A team of five expert professors in the field of community health nursing reviewed the study tools. Each of the experts on the panel was asked to examine the tools for clarity, wording, and format, as well as the general look. According to the comments and recommendations of experts, certain items have been added, modified, and/ or omitted.
2.6. Ethical Considerations
- The Research Ethics Committee of Cairo University, the Faculty of Nursing, and the director of the Al Nour Wal Amal Association for visually impaired women in Cairo governorate gave their first approval.
- The researchers emphasized that participation in the study was entirely voluntary and that each individual had the right to withdraw at any time. The institution director, as the responsible person for visually impaired women, gave written informed consent, and visually impaired women who agreed to participate in the study provided oral agreement, as their vision problems prohibited them from signing the consent. In addition, as they are considered amongst the disabled population, written informed consent was taken by a caregiver or a responsible person in the association.
- Data coding was used to ensure anonymity and confidentiality. Subjects were promised that their data would not be utilized in another study without their approval and that the information gathered would be used only for the study.
2.7. Procedure
- Upon receiving formal approval from the Faculty of Nursing, Cairo University, to conduct the study, official permission was obtained from the director of Al Nour Wal Amal Association for visually impaired women in the Cairo Governorate to approve the fieldwork and collect data.
- Before the beginning of the study, the researchers explained the purpose and steps of the study to the participants. Written informed consent was obtained from the association director as the responsible person for women, and oral consent was obtained from visually impaired women who accepted to participate in the study.
The study included the following phases:
2.7.1. Assessment Phase
This includes the assessment of knowledge, beliefs, and behaviour of visually impaired women toward breast self-examination using the study tools. The researchers introduced themselves to each woman and provided a verbal explanation of the study in simple terms. Then, the researchers explained the instrument content and filled in the tools of each woman by themselves, as the women are visually impaired. The questionnaires were filled in the presence of a responsible person in the association. The time spent filling out the questionnaires ranged between 20-30 minutes for each participant. The researchers collected the data twice a week from 9 a.m. to 1 p.m.
• Implementation of the program: based on the pre-assessment data and related literature review, the researchers designed the educational program about breast self-examination practice to improve women’s knowledge, health beliefs, and behaviour. The educational program was delivered according to the level of understanding of visually impaired women.
• The program included knowledge regarding breast cancer and BSE, the time of performing BSE, how to perform BSE, and the normal and abnormal characteristics of the breast using simulators (breast models) of the normal and abnormal breast, allowing women to palpate them to be able to compare between the normal and abnormal breast, and applying re-demonstration to ensure that they are able to differentiate between the normal and abnormal breast to ensure that they perform BSE correctly. The researchers gave the women audiotape recordings and a booklet in Braille to use as a reminder of the program's content.
The booklet and the program’s contents were designed by the researchers. El-Nour and El-Amal Association revised and translated the Arabic language/program handout into the braille method. The contents of the program were recorded orally on CD by the researchers and were distributed to visually impaired women to hear all the program content comfortably. The designed program was conducted in four teaching sessions in the form of a teaching class through pre-designed teaching materials. The duration of sessions was from 20 to 30 minutes.
2.7.2. Evaluation Phase
The effectiveness of utilizing the health belief model in improving the knowledge, beliefs, and behaviour of visually impaired women toward breast self-examination was evaluated in this phase. The same tools used for the pre-test were applied during the immediate post-program period to the same women.
2.8. Statistical Analysis
The replies were translated into SPSS Statistics version 22 for additional statistical analysis after the data-gathering stage was completed. Furthermore, the mean and standard deviation were used to describe quantitative quantities. Percentages were used to describe qualitative factors. The Pearson correlation test was used to evaluate the data. A value of 0.05 was used as the significant level.
3. RESULTS
Table 1 shows that 42.9% of women aged between 25 and >35 years, 38.1% aged >25, and 19% of them aged between 35 > and 45 years old, and were all single. Regarding their educational level, 42.9% of women were unable to read and write or had primary education, while 14.2% of them had secondary education. In relation to family income, 57.1% of women had income that met routine expenses and emergencies, while 4.8% of them were able to save money. Moreover, the table indicates that all women were doing manual work; 61.9% of them were from rural areas and did not have health insurance.
Table 2 reveals that 19% of women had a family history of breast cancer, and 23.8% of them had a previous breast problem. Furthermore, the table clarifies that all women did not take contraceptive hormones and did not breastfeed.
Table 1.
| Variables | Frequency | % |
|---|---|---|
| Age/Year | ||
| >25 | 16 | 38.1 |
| 25 >35 | 18 | 42.9 |
| 35 >45 | 8 | 19.0 |
| Mean ± SD | 28.1±7.32 | |
| Marital Status | ||
| Single | 42 | 100.0 |
| Educational Level | ||
| Unable to read and write | 18 | 42.9 |
| Primary | 18 | 42.9 |
| Secondary | 6 | 14.2 |
| Family Income | ||
| Do not meet routine expenses | 4 | 9.5 |
| Just meet routine expenses | 12 | 28.6 |
| Meet routine expenses and emergencies | 24 | 57.1 |
| Able to save/invest money | 2 | 4.8 |
| Type of Work | ||
| Manual work | 42 | 100.0 |
| Place of Residence | ||
| Rural | 26 | 61.9 |
| Urban | 16 | 38.1 |
| Health Insurance | ||
| Yes | 16 | 38.1 |
| No | 26 | 61.9 |
| Risk Factors | Frequency | % | Frequency | % |
|---|---|---|---|---|
| Yes | No | |||
| Family history of breast cancer | 8 | 19.0 | 34 | 81.0 |
| Breast problems, such as mass, abscess, and others | 10 | 23.8 | 32 | 76.2 |
| Taking contraceptive hormones | 0 | 0 | 42 | 100.0 |
| Breastfeeding | 0 | 0 | 42 | 100.0 |
| Obesity | 0 | 0 | 42 | 100.0 |
| Practicing exercises | 12 | 28.6 | 30 | 71.4 |
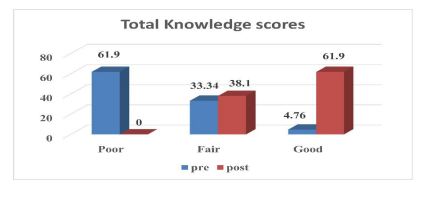
Fig. (3) indicates that only 4.76% of women had a good level of knowledge before the program, which increased to 61.9% after the program. This figure supported the first research hypothesis. Total knowledge scores are classified as follows: a poor level is < 60% of the total score, a fair level ranges from 60% to 75% of the total score, and good knowledge is >75% of the total score.
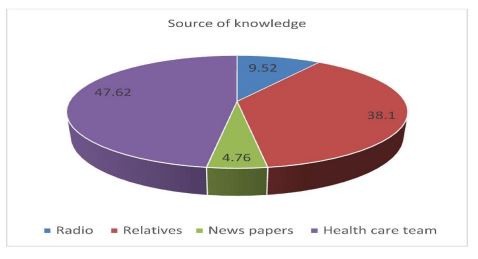
Fig. (4) shows that 47.62% of women gained their knowledge from the health care team, 38.10% from relatives, and only 4.76% from newspapers.
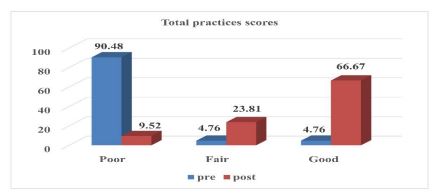
Fig. (5) indicates that only 4.76% of women had a good level of practice before the program, which increased to 66.67% after the program. This figure supported the second research hypothesis. Total practice scores are classified as follows: a poor level is < 60% of the total score, a fair level ranges from 60% to 75% of the total score, and good practice is > 75% of the total score.
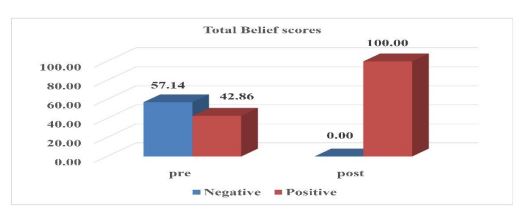
Fig. (6) indicates that 100% of women had positive beliefs after the program, while 57.14% of them had negative beliefs before the program. This figure supported the third research hypothesis. Total belief scores are classified as follows: negative belief is <60% of the total score, and positive belief is ≥ 60% of the total knowledge.
4. DISCUSSION
Breast cancer is a major health concern among Egyptian women. On the other hand, vision impairment creates more difficulties in detecting any abnormal changes in the breasts of visually impaired women. Therefore, early detection of breast abnormalities helps to decrease the devastating consequences of this problem, particularly among visually impaired women. The Health Belief Model is one of the most influential models for predicting cancer-preventive behaviours [1]. The current study aimed to evaluate the effect of utilizing the health beliefs model on the knowledge, beliefs, and behavior of visually impaired women toward breast self-examination.
Regarding demographic characteristics of visually impaired women, results of the current study indicated that more than two-fifths of women aged between 25 to >35 years while less than one-fifth of them aged between 35 to >45 years with a mean age of 28.1±7.32 years old (Table 1). A previous study conducted on younger women [14] in Malaysia revealed that more than two-thirds of women aged between 18 to 20 years. The difference between the two studies could be related to the fact that women stay and work at the El-Nour and El-Amal association because the association provides education, vocational training, and social integration of blind girls and women into society.
According to the findings of the current study, more than two-fifths of women could not read or write and had only primary education, while less than one-fifth had secondary education (Table 1). According to a previous study [15], due to social and geographical conditions, the majority of Egyptian women are illiterate or have only attained primary school, and most females in Egypt are less educated, particularly in rural areas. Access to elementary school is still hampered by gender inequities, and many have visual impairments that make learning difficult.
On the contrary, this result contradicted the findings of a study [5] conducted on 225 Iranian women at a private center in Tehran and reported that the majority of the women were high school graduates. The social and cultural disparities between the two countries could explain the disparity between the two studies.
In relation to family income, more than half of women had income that met routine expenses and emergencies, while the minority of them were able to save money (Table 1). This result was supported by a study [16] conducted on the effects of health belief model-based education on health beliefs and breast self-examination in Turkey and found that 70% of the study sample had an income equal to the expenditures.
The study reflected that the majority of the women did not have a history of breast cancer in their families. This result was in agreement with another study [17, 18] conducted on women at the Health Centers of Tabriz, Iran, which reported that 91.5% of the study sample did not mention breast cancer in their family history, which was consistent with the findings of a previous study [14].
The study results showed that less than half of visually impaired women gained their knowledge from healthcare professionals and more than one-third from their relatives (Fig. 4). This result was supported by a study [19, 20] conducted in Sari, Iran, and reported that two-fifths of the study sample reported doctors as the main source of knowledge. This could be related to the frequent visits from the Baheya Foundation team to El-Nour and El-Amal Association, as mentioned by the participant.
Regarding total knowledge and practice scores of visually impaired women, results of the current study revealed that only 4.7 percent of women had a good level of knowledge and practice in the pretest, which increased to nearly two-thirds and more than two-thirds in the posttest, respectively. Moreover, a highly statistically significant difference was found between women’s total knowledge and practice scores regarding breast self-examination in pre- and post-test (Figs. 3, 5 and Appendix A and B). These results supported the current study hypothesis, i.e., visually impaired women who will receive health education programs will have higher knowledge scores regarding breast self-examination after implementation of the program, and visually impaired women who will receive health education programs will also have higher practice scores regarding breast self-examination after the implementation of the program.
The study findings are consistent with previous research studies [10] conducted on 14 adolescent girls at Al Noor Institute for Visually Impaired Students in Shebein El Kom City, Menoufia Governorate, Egypt, and discovered that there was an increase in total knowledge and practice scores in the pre- and post-test, as well as a highly statistically significant difference in knowledge and practice about breast cancer and breast self-examination. Moreover, a study [21] was conducted on 37 blind girls at the Al Noor institute for blind girls in Qena governorate, Egypt, and found a statistically significant improvement in the total knowledge and practice scores of blind girls in post-test compared to pre-test scores.
On the same line [22], a study conducted on 40 visually challenged girls to assess the effectiveness of audio drama and touch and feel techniques on breast self-examination in knowledge and practice among visually challenged girls revealed that post-test knowledge and practice scores were higher than the pre-test. Moreover, there was an improvement in knowledge and practice on breast self-examination among visually challenged girls. Also, the current findings agreed with the findings of a study [23] conducted at Al-Alzhar University's Health Technical Institute for Female Students in Nasser City, Cairo, Egypt. There was a lack of knowledge and poor practice regarding breast self-examination before educational training, which was improved after training and was consistent with the findings of a previous study [24].
Concerning the health beliefs of visually impaired women regarding breast self-examination, the study results revealed a highly statistically significant difference between total health belief subscales in pre- and post-tests. Also, there was a highly statistically significant difference between total health belief scores among women in pre- and post-tests, and there was an improvement in health belief model subscales and total health belief scores after program implementation. Furthermore, all of the women had positive beliefs after the program implementation, thus validating hypothesis number three (Appendix A and Fig. 4).
These findings are in agreement with several studies [25] examining the effect of health belief model-based educational intervention about breast cancer on knowledge, health beliefs, and breast self-examination practice in Benha City, Egypt, and found that the study group had considerably higher mean scores on perceived susceptibility, severity, benefits, cues for action, self-efficacy, and the total health belief model than the control group. On the same line, this result is congruent with a study [26] conducted to assess the effect of health-belief-model-based training on the performance of 144 women in breast self-examination attending healthcare centers in the city of Abadeh in Fars Province, Iran and found that the average score of health belief increased significantly (p<0.001) after the intervention.
Furthermore, a study [27] was conducted on 244 women at a community education center located in Sivas, a city in Turkey, to assess the effects of training on knowledge and attitudes about breast cancer and early detection methods and discovered a statistically significant improvement in CHBMS subscales scores (susceptibility, seriousness, benefits, barrier, and self-efficacy perception) compared to pre-test, which [28] also supported the current findings.
Moreover, a study [29] was conducted on 226 women at Dezful Health Centers, Iran, to assess the effect of health belief model education on breast cancer screening behaviour, and it was revealed that the difference between total health belief scores and health belief model subscales before and after the program was highly statistically significant. A study [1] reported that, after implementing the health belief model-based education in Egypt, researchers discovered that total health belief scores improved and positive effects of the health belief model-based education were observed on women's knowledge and breast cancer prevention behaviours regarding breast self-examination.
Results of the current study reflected a highly statistically significant difference between women’s total knowledge scores, total health belief scores, and total practice scores regarding breast self-examination before and after the program implementation. This finding was in agreement with many studies [4, 10, 16, 30, 31], which showed that educational programs have a significant positive effect on the knowledge, beliefs, and behavior of visually impaired women toward breast self-examination.
As a high-risk group, visually impaired women are subject to poor health and face many difficulties in their lives, especially when they try to maintain independence, get medical care, or get screening tests. As reported previously [32], vision impairment has a significant impact on the lives of those who experience it as well as on their families, their friends, and society. They can be terrifying and overwhelming, making those around them skeptical of their ability to maintain their independence, pay for necessary medical care, keep their jobs, and provide care for themselves and their family. Vision loss has been linked to falls, injuries, and deteriorated status in a variety of aspects, including mental health, cognition, social function, employment, educational attainment, and a greater need for community services as well. It can also have an impact on one's quality of life, independence, and mobility.
Visually impaired women are less likely to undergo screening procedures and are, therefore, more vulnerable to getting the disease. Consequently, they mostly lack access to sufficient treatments, which can delay their cure and increase their risk. The development and dissemination of accessible health education materials is one way for people with disabilities to improve their knowledge as part of comprehensive health care. Health practitioners must be knowledgeable about disabilities, the laws that protect them, and the measures taken to ensure their accessibility. Various strategies are used to educate blind women about breast cancer and early detection as part of the nurse's role in supporting their health. There is not sufficient research done on the issue addressing the promotion of visual health in individuals [33].
Visually impaired women are thought to have some trouble examining their bodies to find an indication for a specific disease like breast cancer compared to others who are not visually impaired. The health education program will aim to replace the general understanding of breast cancer with academic knowledge regarding the early detection techniques of this neoplasm. It will be advantageous to the demographic group involved, as it can help in enhancing information. It can also be attributed to its potential to improve information and communication systems for the health education of people with disabilities. Additionally, it is anticipated that it will give health managers the information they can use to plan and carry out health education strategies aimed at the early detection, assessment, treatment, and rehabilitation of blind people who are vulnerable or affected by this disease [34].
Several studies [35, 36] reported that women with vision impairment claim to face physical and communication difficulties, poor health care conditions, and excessive family protection. In spite of having laws that mandate that people who are blind or visually impaired have the right to receive information on reproductive health, there are still gaps in the way these rights are being implemented in terms of services and preventative initiatives.
The literature identifies a number of barriers and facilitators associated with health information delivery to visually impaired people. These operate at three levels: the individual, the community, and society. Barriers at the individual level include a lack of knowledge on specific health topics, limited knowledge of Braille, as well as language and cultural barriers associated with cultures. Community-level barriers include social taboos and insufficient time for visually impaired people to process the information. Additional barriers to effective information provision are imposed by society itself. For example, service providers are often unaware of how many of their clients have a visual impairment. There are often long delays associated with formal registration as blind or partially blind, leading to further delays in individuals’ receipt of the health information they require. It is important to make the needed information available in a wide variety of formats suitable for people with different degrees of visual impairments [37].
Recent studies have shown that it is essential to increase awareness of women, especially the visually impaired, about the risks of breast cancer and its early detection. The lack of knowledge about this might have been due to insufficient educational programs about breast health awareness. Women who will be exposed to direct education on breast cancer and breast self-examination have the ability to teach it to others in ways that are suitable for them. The nurse might be the best source of health information for those women. This chain reaction is promising when there is a group of women who are aware of the procedure of early detection of breast cancer and are capable of influencing and training other women about self-examination. This type of education through the nurse can spread health information more quickly in the community [38].
In this sense, community health nurses and other health professionals need to increase their understanding of the challenges faced by women with visual impairment. They also need to be prepared to interact with people who are visually impaired. Healthcare settings need to be equipped to meet their needs and provide care accordingly. Community health nurses can be an advocate for women who are blind or visually impaired by identifying their needs and creating health education programs to guard them against dangers. Improving one's way of life and disseminating knowledge in educational programs promoting a balanced diet, regular exercise, stress management, reproductive health, and injury prevention are of utmost importance [39]. They might assist women who are visually impaired in living and working in the community. Additionally, they work along with their instructor and family to prevent social, physical, and psychological issues for those women as early as possible [40, 41].
Community health nurses play an exceptional role in alerting the community to the early detection of breast cancer, especially for groups at risk, as they usually have the closest contact with female patients. Nurses can use their knowledge of health services to educate women about breast cancer risk factors and the available breast cancer screening services and practices. Through their knowledge of the healthcare system, nurses play an important role in educating visually impaired women about the importance of breast self-examination and understanding the risk factors of breast cancer and accessible breast cancer screening programs and procedures. Educating women about the value of breast self-examination and the risk factors for breast cancer is a critical role that nurses can perform very well [42].
5. IMPLICATIONS OF THE STUDY
The findings of this study have implications that can guide policymakers and healthcare teams at the governmental level to identify health issues related to women's health and well-being, especially visually impaired women, as a vulnerable group. Also, it can help in planning for future interventions to increase awareness of breast self-examination as a preventive behavior, which will consequently help in lowering the incidence of breast cancer through early detection, treatment, and improvements in outcome and prognosis. In addition, it also reduces the psychological, social, and economic impact as well as medical complications in women, their families, the healthcare system, and the community.
Future research must identify the health information needs regarding breast cancer and breast self-examination for women with different degrees of visual impairment, considering all aspects of information, such as content and format. This might be achieved by greater involvement of the healthcare team in the design and formatting of the content of information and in more complicated matters, such as timing and means of message delivery, any additional support, as well as ensuring accessibility. Future studies should consider the factors affecting the prevalence of breast cancer among visually impaired women. Visually impaired women have a special set of health and social care information needs that are worthy of exploration; they need to be more actively involved in planning and conducting research studies. Finally, the recommendations of this study will be further discussed in nursing education and nursing research.
CONCLUSION
The current study found that after program implementation, there was a significant improvement in knowledge, practice, and health beliefs about breast self-examination among visually impaired women, emphasizing that educational programs based on health belief models have a positive effect in improving women's knowledge, practice, and health beliefs about breast self-examination.
RECOMMENDATIONS
The following recommendations are made in light of the study's findings:
1. Raising visually impaired women’s awareness about breast cancer and breast self-examination through educational programs in different vision impairment schools and associations to improve their knowledge and behaviours with regard to breast cancer prevention.
2. Distribute copies of an educational braille booklet and a recorded CD about breast cancer and breast self-examination based on the Health Belief Model for visually impaired women in associations to improve women’s knowledge, practice, and health belief.
3. For results to be generalized, this study needs to be replicated on a wide scale and in varied settings.
LIST OF ABBREVIATIONS
| BSE | = Breast self-examination |
| HBM | = Health Belief Model |
| ANWA | = Al Nour Wal Amal Association |
| CHBM | = Champion's Health Belief Model |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This research was approved by the Human Research Ethics Committee-Faculty of Nursing-Cairo University.
• Study number (2020-57).
• IORG (0006883).
• RHDIRB (2019041701).
• FWA (00026458).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013 (http://ethics.iit.edu/ecodes/node/3931).
CONSENT FOR PUBLICATION
Informed consent was obtained from the participants involved in this study after explaining the purpose of the study and assurance from the subject about the privacy and confidentiality of the obtained data. A summary of the interventions was explained to all participants who voluntarily agreed to participate in the study.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available upon request from correspoding author [M.M.A].
FUNDING
None.
CONFLICT OF INTEREST
The authors confirm that this article’s content has no conflicts of interest.
ACKNOWLEDGEMENTS
The authors would like to acknowledge El-Nour and El-Amal Association and all visually impaired women in the Cairo governorate who volunteered to participate in the study.
| Variables | Positive | Negative | Mean ± SD | F | P | |||
|---|---|---|---|---|---|---|---|---|
| N | % | N | % | |||||
| Perceived susceptibility | Pre | 16 | 38.1 | 26 | 61.9 | 13.0476± 3.89466 | 49.546 | .000* |
| Post | 38 | 90.48 | 4 | 9.52 | 20.5238± 3.74321 | |||
| Perceived seriousness | Pre | 30 | 71.43 | 12 | 28.57 | 20.5238± 3.74321 | 39.135 | .000* |
| Post | 40 | 95.24 | 2 | 4.76 | 25.6667± 3.79130 | |||
| Perceived benefits | Pre | 38 | 90.48 | 4 | 9.52 | 16.0952± 4.07137 | 38.928 | .000* |
| Post | 40 | 95.24 | 2 | 4.76 | 20.9048± 2.89499 | |||
| Perceived barriers | Pre | 30 | 71.43 | 12 | 28.57 | 16.6190± 3.51271 | 31.022 | .000* |
| Post | 10 | 23.81 | 32 | 76.19 | 21.8571±4.98080 | |||
| Cues for actions | Pre | 6 | 14.29 | 36 | 85.71 | 15.2381±4.04734 | 121.158 | .000* |
| Post | 40 | 95.24 | 2 | 4.76 | 24.2381±3.42024 | |||
| Total health belief scores | Pre | 81.5238 ± 11.81821 | 146.766 | .000* | ||||
| Post | 110.7619 ± 10.24531 | |||||||
| Total knowledge scores | Pre | 12.5238 ± 8.07658 | 112.818 | .000* | ||||
| Post | 29.9524 ± 6.91747 | |||||||
| Total practice scores | Pre | 0.5714 ± 1.38181 | 179.433 | .000* | ||||
| Post | 4.9524 ± 1.60718 | |||||||
| Variables | Total knowledge | Total practices | Total beliefs | |||
|---|---|---|---|---|---|---|
| r | P | r | p | r | p | |
| Age | 0.191 | 0.225 | -0.06 | 0.707 | -0.169 | 0.284 |
| Educational level | 0.05 | 0.753 | 0.313 | .044* | 0.334 | .031* |
| Family income | 0.096 | 0.545 | 0.18 | 0.254 | 0.113 | 0.475 |
| Place of residence | 0.096 | 0.545 | 0.18 | 0.254 | 0.51 | .001** |
| Health insurance | -0.096 | 0.545 | 0.03 | 0.85 | -0.113 | 0.475 |
| Perceived susceptibility | 0.573 | .000** | 0.612 | .000** | ||
| Perceived seriousness | 0.529 | .000** | 0.623 | .000** | ||
| Perceived benefits | 0.558 | .000** | 0.582 | .000** | ||
| Perceived barriers | -0.456 | .000** | -0.575 | .000** | ||
| Cues for actions | 0.726 | .000** | 0.835 | .000** | ||
* Correlation is significant at the level of.05

