All published articles of this journal are available on ScienceDirect.

Evaluating the Cost-Effectiveness of Plastic Surgery Based on the Satisfaction with Quality of Life and Nasolabial Appearance in Thai Preteens with Cleft Lip and Palate
Authors Info & Affiliations
Abstract
Background:
Cleft Lip and Palate (CLP) negatively affect the quality of life (QoL) and nasolabial appearance, especially in preteen patients who start to be interested in their own appearance and society.
Objective:
The objective of this study is to evaluate the cost-effectiveness of plastic surgery for Thai preteen CLP patients through their satisfaction with their QoL and nasolabial appearance.
Methods:
A cross-sectional study covered purposively selected 30 samples aged between 8 and 12 years old.Their satisfaction with their QoL and appearance was reflected through an interview and a questionnaire with the cooperation of their parents as their caregivers including satisfaction with their nasolabial appearance evaluated by five experts. They compared the photos of patients’nasolabial appearance with those of normal faces of children of the same age using 5-rating scales.
Results:
General findings showed 53.3% of samples were male patients with mostly (63.3%) UCLP whose parents were mainly (73.3%) poor, so they relied on government financial supports for the treatment. Only some (15%) earned up to 5,001 to 10,000 baht per month because of their low education with just high school level. Specific findings indicated the overall satisfaction with QoL through five dimensions at average level (3.26±1.39). This was based on the satisfaction with the center services, the overall treatments, the medical additional costs, parental satisfaction with psychosocial effects including concerns about the impacts of CLP on the family ranged from high to low i.e. 4.30±0.98, 3.72±1.15, 3.70±1.14, 3.33±1.08 and 2.81±1.46 respectively. Moreover, five experts trended to be highly satisfied with patients’ nasolabial appearance by rating it from Good (53.3%) to Fair (43.43%) with only Poor (3.3%).
Conclusion:
The good cost-effectiveness of the surgery was represented through the average and high satisfaction of CLP patients with their QoL and their appearance respectively indicating the absence of disability weights for these treated CLP patients.
1. INTRODUCTION
Cleft lip and palate (CLP) is the most common external congenital craniofacial abnormality that occurs in approximately 1 out of 1 000 live births worldwide. In Thailand, the incidence is about 2.14 cases per 1 000 live births. It is more prevalent in the Northeast of Thailand, which is the most deprived area of the country. The causes could stem from taking some unprescribed or local herbal medication without consulting gynecologists during pregnancy and the influence of genes and other environmental factors during pregnancy [1, 2]. As CLP disfigures the face, it creates concern for parents and social isolation from the family and community besides impairing feeding, communication, and speech development. Therefore, the patients are affected both physically and psychologically, leading to a reduced QoL for them and their families. CLP surgery, which is commonly done in children, aims to improve the quality of life for patients and their families. Their quality of life could be enhanced by their improved appearance as appearance is one of the main parts of their body image (BI) which directly and strongly influences their quality of life [3].
Long-term medical treatment and assessment, which are typically carried out by an interdisciplinary team based on a specific age range, is necessary. A critical period for this treatment and assessment is between 8 to 12 years because these preteens naturally become increasingly concerned about their body image and how others perceive them. This concern is heightened for preteens with CLP and their parents, who of course worry about their children’s craniofacial abnormality and how it will impact their relationship with others, their self-image, self-worth, individuality, and psychosocial adjustment within their specific social environments [4].
The ultimate goal of the Tawanchai Center, which is one of the Thai royal projects, is to improve the QoL of CLP patients and their families. Our study aimed to evaluate the cost-effectiveness of CLP plastic surgery done on these patients from the disadvantaged Northeastern part of Thailand based on their satisfaction with the QoL and nasolabial appearance after surgery.
Plastic surgery requires specialized surgical expertise and good postoperative facilities to avoid potentially lethal postsurgical complications. It demands expertise and infrastructure that may not be readily available, particularly in low- and middle-income countries. The WHO Guide to Cost-Effectiveness Analysis discusses ways to minimize the burden of disease and maximize health outcomes in resource-scarce settings. Medical treatments need to have positive health benefits without great and unacceptable sacrifices [5]. Studies on the cost-effectiveness of surgery in children with CL or CP have been carried out in different regions like Eastern and Central Africa [6]. Another research showed the cost-effectiveness of surgical interventions for CLP patients in the developing world and highlighted the crucial role of surgery from a global public health perspective. The life tables of the first Disease Control Priorities Project (DCP1) in Sub-Saharan Africa [7, 8] suggested that the entire burden of disease from CLP is incurred within the first 4 years of life and the disability associated with it goes beyond the first 5 years of life and continued until their adulthood or even their whole life. For 8 Operation Smile missions analyzed, the cost per patient was between $278 and $1827 (average $796). Using the modified life tables created by the authors, the cost per patient was between $7.36 and $96.04 (average $33.94). This indicated that the absence of disability weight for untreated CLP after the fifth year of life did not justify the reality of living with it. They concluded that secondary interventions alleviate disabilities and should enable an individual to approach a zero residual disability weight.
Also, the nursing care system for patients with CLP and craniofacial deformities had been well developed at Tawanchai Cleft Center. For instance, Pradubwong et al. [9] had showed the importance of the interdisciplinary nursing care team as well as the specialized care center with systematic coordinated care. This nursing care system consisted of relevant medical staff like specialist nurses and medical doctors for providing psychosocial care, breast feeding, counseling and other required assistance to provide holistic, superior quality care for directly serving the needs and effectively solving the problems of the patient/family leading to their better quality of life. Thus, it was clear that the nursing care system at this center whose nurses with specialism for nursing children with CLP have taken a vital role in the disciplinary nursing care team. These nurses at the center started providing effective support, guidance and care for the pregnant mothers both before and after the CLP babies were born. This nursing care was under the interdisciplinary care team continued both before and after their surgical treatment from the center until the age of 19 to 20 years old which is the final stage of the treatment and the follow-up session.
In addition, nurses also played a very important role in assessing the QoL of the patients with CLP and their families in physical, psychological and social health after completing the surgical treatment from the center [10]. Furthermore, the team of nurses at Tawanchai Centre was a main agent in empowering volunteers for patients with Cleft Lip and Palate [11] and developing Cleft lip/Palate Face models for teaching parents of CLP children [12]. All of these clearly indicated the importance of nurses as one of the active team players in multidiscipline team for improving the QoL of patients with CLP in the center before and after the patients were born through their guiding, counselling, caring, managing and coordinating to support the patients [13] until they become adult and complete the treatment when they turn 19-20 years old.
A systematic review and analysis of cost-effectiveness studies [8] assessed surgical interventions in low-and middle-income countries and quantified their potential value. Surgery is often thought to be expensive and complex and this might be a barrier to its widespread acceptance in global health efforts. A systematic review found that only 26 out of 584 surgical interventions met the full inclusion criteria. It indicated that many of these essential surgical interventions in resource-poor countries were cost-effective or very cost-effective. Although the quantification of the economic value of surgery provides a strong argument for the expansion of surgery in the global health movement, it should not be the only argument for resource allocation-other organizational, ethical, and political arguments can also be made.
The findings of Odton et al. [14] showed that the real cost of patient management was on average 12,025.14 baht per patient, and the reimbursement from the National Health Security Office (NHSO) was approximately 10,527.63 baht per patient, which is 87.55% of the total cost. The largest expenses were for anesthesia (36.42%), thus indicating that the total cost of surgery per patient was far lower than costs including medical equipment, the operation room and wardroom.
In cost-effectiveness analysis, costs are compared with other outcomes such as pain or symptom-free days. It is necessary to assess both the costs and other consequences as different health care interventions might not produce the same outcomes as expected [15]. This is in line with the cost-effectiveness analysis (CEA) for health interventions by the WHO [16]. To evaluate specific interventions, CEA is used to quantify gains and setbacks using parameters such as the disability-adjusted life years (DALYs) or cost per life saved.
We used the WHO CEA concept to justify evaluating the cost-effectiveness of plastic surgery for Thai preteen patients with CLP based on the satisfaction with their QoL and nasolabial appearance. This is especially necessary because they were underprivileged patients in the rural areas of the Northeast of Thailand, which is considered the most deprived area of the country with the highest prevalence of CLP [1, 2]. They need long-term support services that will incur high treatment expenses. Two previous investigations at the Tawanchai Center for Cleft Lip, Cleft Palate, and Craniofacial Deformities at Srinagarind Hospital identified three concerns in families taking care of patients with CLP. They are as follows: 1) the lack of knowledge about treatment care by the parents; 2) socio-economic problems; and 3) the QoL of affected patients [17-19].
A relevant study conducted at a mobile speech camp indicated that the caregivers of patients with CLP required support for language and speech development, and general activities such as eating and drinking [17]. Another study showed that young patients with CLP had unhealthy oral cavities and exhibited a lower QoL compared with normal children [18]. Dental care, speech practice, and health care were identified as vital requirements to improve the QoL of these patients [18, 19]. Another study which was carried out through phone interviews with the parents of 2 to 12-year-old patients with CLP revealed that appearance was considered as an essential part of the QoL for the 8 to 12-year-old patients because children at that age started to pay attention to their appearance and that of others. This shifting perception could cause them to develop anxiety about their appearance [4, 19, 20].
Another related study identified the psychosocial effects on the parents of children with CLP, such as worries about their child’s health, problems related to their child’s psychosocial development, and their relationships with others [19, 21]. Similarly, CLP can affect children’s self-esteem due to satisfaction with their appearance and individuality being impacted and this directly affects these children in making social adjustments [22, 23].
The face which is made up of eyes, nose, lips, eyebrows, ears, cheeks, forehead, and chin creates the first impression one makes on others. Abnormalities of the nose, such as twisting on either side or at the base or having an abnormal nasal alar crease, are quickly noticed. A plastic surgeon needs to repair the abnormally-shaped noses of patients with CLP by doing rhinoplasty with a nasal creator device to stabilize the structure of the nose. Additionally, an orthodontist can prepare the alveolar cleft for a maxillofacial surgeon who performs bone grafting to help the patient achieve an appearance close to normal.
Interestingly, one of the studies investigating the evaluation of nasolabial appearance in patients with CLP after surgery found that there were no differences in the ratings between young adults with CLP and surgeons [23]. There was also no difference in evaluation by experts either with or without experience in CLP [24]. A study of the nasolabial appearance of patients with unilateral CLP who had undergone plastic surgery in Vietnam and Estonia revealed that there were no differences in the assessments by experts, although different methods were applied to treat the patients [25].
Different studies offered a variety of indicators for evaluating the success of plastic surgery, such as the Nasolabial Yardstick [26], the Cleft Aesthetic Rating Scale (CARS) [27], and the Esthetic Index. They all evaluated the nasolabial appearance using 2D pictures of the nose, which showed the front and side views of the nose, in the following four dimensions: nasal form, nasal symmetry, vermillion border of the lips, and nasolabial profile. Five to seven evaluators used five rating scales to find the internal correlation which is determined using the appearance score. Although the patients were satisfied with their nasolabial appearance with overall good treatment in many cases, it was found that the appearance score of nose treatment was lower than that of mouth treatment [28]. In addition, patients with CLP who rated their post-surgery nasolabial appearance as “Fair” or “Good”, still tended to have lower self-esteem because they felt that they were less beautiful [29].
However, CLP surgery, which is commonly done in children, predominantly aims to improve the quality of life for patients and their families. Their quality of life could be developed by their improved appearance as the appearance is one of the main parts of their body image (BI) which directly and strongly influences their quality of life [3]. The study investigated the relationship between the two found that a good body image was a strong predictor of QoL or a predictor enhancing the quality of life in all sub-domains like physical, psychological, social, environmental and culture standardized (CS) environmental domains.
A systematic review of QoL studies [30] found that there were few studies on the image satisfaction of patients, families, and treatment teams. The evaluation of treatment outcomes is essential to the success of the treatment and care of those patients with CLP. This was absolutely justified this current study in assessing QoL which was closely related to patients’ facial appearance as the preteen CLP patients aged between 8 to 12 years old starting to be aware of or worried about their own appearance [4, 29]. Therefore, our study aims to evaluate the cost-effectiveness of plastic surgery based on the satisfaction of patients with their QoL and nasolabial appearance. The findings will help improve the quality of treatment, care, surgery, and recovery of the patients with CLP.
A systematic review of QoL studies [30] found that there were few studies on the image satisfaction of patients, families, and treatment teams. The evaluation of treatment outcomes is essential to the success of the treatment and care of those patients with CLP. This was absolutely justified in this current study in assessing QoL, which was closely related to patients’ facial appearance as the preteen CLP patients aging between 8 to 12 years old started to be aware of or worried about their own appearance [4, 29].
Although the cost of the surgery at this medical center for cleft lip and cleft palate seemed costly, especially for the poor, it was worth doing as one of the best choices among other alternatives. Of course, this medical treatment needed a long term and continuous treatment for at least 15 years requiring specialists and high technology, which greatly affected the social and economic system of the whole nation and it was a great barrier for underprivileged patients. For instance, retrospective studies obtained from secondary data about the cost of plastic surgery for a cleft lip and cleft palate patient with the universal health coverage program (UHCP) of Tawanchai Center, Srinagarind Hospital, Faculty of Medicine, Khon Kaen University, 2008-2013 was 22,739.54 Baht (690 US $) per patient. Similarly [31], the other related study about similar medical treatment with patients aged between 4- 7 years old receiving Cheiloplasty, Palatoplasty, cleft lip and nose correction, and closure fistula had average costs (in 2019), 12,515 baht, 16,229 baht (380 US $), 14,895 baht (492 US $) and 20,315 baht (616US $), respectively.
However, if considering only the cost of surgery, we can see that this cost definitely indicated that the cost-effectiveness of the surgery was unquestionable as it was the best solution for treating the patient by the surgery if compared to other alternatives especially leaving the patients without any treatment till their life if considering in terms of cost-effectiveness for the sake of quality of life for both the patients and their families.
Therefore, our study aims to evaluate the cost-effectiveness of plastic surgery based on the satisfaction of patients with their QoL and nasolabial appearance. The findings will help improve the quality of treatment, care, surgery, and recovery of the patients with CLP.
2. MATERIALS AND METHODS
2.1. Study Design and Sampling
The study design was a cross-sectional study with Thai preteen patients with CLP aged between 8 to 12 years. Based on an initial study before this main study from 2017 to 2019, it was found that there were 613 patients of CLP who underwent primary surgery in this research center of Cleft Lip-Cleft Palate and Craniofacial Deformities since it was founded in 2008.
In focus, the sample size of 30 participants was purposively selected from the whole population within three different groups based on their ages ranging from 4-6, 8-12 to 16-20 years old. The population and the samples of each age range were calculated based on this formula.
The sample size of 30 participants aged between 8 to 12 years old was the target sample of the study based on the total age of all 613 populations. Its population size was 274, with 95% of its confidence interval level with standard deviation (SD = 0.05). The size of its tolerance was acceptable with e = 0.05 or e2 = 0.0025 (appendix).
2.2. Participants
In particular, the target samples were intentionally chosen from its 274 populations within its specific age ranges between 6 to 12 years old. They were selected from the patients who came for an appointment with one or more of the multidisciplinary team, such as a dentist or a surgeon, during the follow-up treatment after their primary surgery.
All of them would first come to the center to get financial support and necessary advice or guidance from the nurses at the center before seeing any specialist. At this particular time, the researchers could screen and purposively select the eligible samples on- site on when they came to the center for their medical appointment.
Five main eligibility criteria for choosing 30 participants were: 1) He or she was a patient with either unilateral or bilateral CLP; 2) He or she underwent a primary surgery being an on-going follow-up treatment at the Tawanchai Center and resided in the Northeast area to easily get access to the facilities at the center as needed; 3) He or she was in the age range between 8 to 12 years old during the data collection in 2020; 4) He or she had only a nonsyndromic CLP, and 5). Both patients and their parents were willing to participate in the project with consent.
A purposive sampling method was applied to reduce bias due to the patients’ homogeneous nature, so any eligible patients coming for health services at the center could take part in the study as being anonymous if they willingly consented. They were interviewed and asked to fill in questionnaire with clear explanations. They also had their front and side view photographed. The whole process took about 15 to 30 minutes. The data collection lasted about 10 months from March to December of 2020 at the Tawanchai Center.
2.3. Research Tools
The first research tool, namely, THAICLEFT QoL was adapted from the WHO QoL questionnaire. It was specifically designed to traditionally and culturally suit the Thai context by the teams of child psychiatrists and specialist nurses for assessing the QoL of Thai CLP children [32]. It includes an interview and a 41-item questionnaire with five rating scales from 1 to 5 in five main aspects related to the QoL of patients. This questionnaire has a reliability of 0.94.
The questions in the questionnaire and the interview focused on life satisfaction, which is closely related to self-esteem, self-image, and social roles. QoL also depends on their health or the outcome of treatment within Thai Buddhist tradition and culture. It was the researchers’ intention to identify the quality of medical services offered at the center in order to develop the medical treatments and additional services provided to the patients which directly lead to the patients’ QoL. In other words, the quality of medical treatments and the services provided at the center which the patients can get access to are one of the major indicators of their QoL. Hence, the questionnaire did not only focus an individual person but also covers all aspects relating to or affecting on the patients’ QoL.
The method of measurement of the QoL was based on five rating scales ranging from the least satisfied to the most satisfied. The quantitative variables in the questionnaire cover five dimensions with the following items: 1) 8 items about overall treatment; 2) three items about services at the center; 3) four items about medical and additional costs; 4) six items about parental satisfaction with psychosocial effects, and 5) twenty items about the effects of CLP on the family. The CLP patients were assisted by their parents in completing the questionnaire and when being interviewed. The whole process was undertaken at the Tawanchai center, a prestigious CLP regional center located in Srinagarind University Hospital inside Khon Kaen University under the cooperation of the Faculties of Medicine and Dentistry.
The second research tool was the front and side view photographs of each patient’s face that were used to evaluate the nasolabial appearance focusing on the nasal alar parts and lips, especially the nasal form, nasal symmetry, vermillion border, and nasolabial profile. Each of these four aspects was assessed by five interdisciplinary assessors with 5 rating scales resulting in 20 (4 X 5) scores in total. They assessed each participant’s appearance by comparing their photo with that of a child of the same age without CLP. The criteria for assessment ranged from 1= very good to 5 = very bad. The photo of one patient sample after the surgery is shown in Fig. (1).
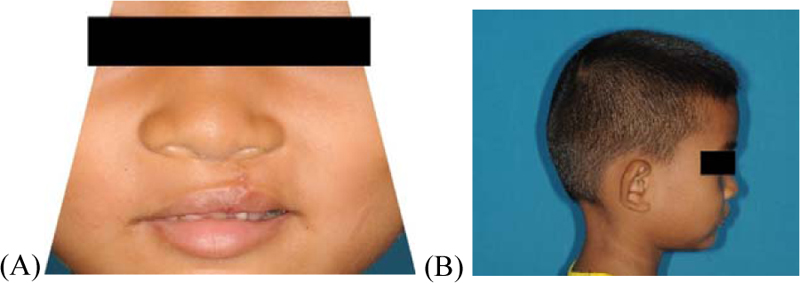
(A) Nasal form and symmetry and vermillion border.
(B) Nasolabial profile.
Retrieved from Tawanchai Center Database, with permission of Tawanchai Center
2.4. Statistical Analyses
The statistical method for the quantitative data gained from the interview and the questionnaire representing cost-effectiveness based on satisfaction with their QoL and nasolabial appearance were analyzed and presented in the forms of percentages, average values, and standard deviations. The data from the assessment of nasolabial appearance by experts were analyzed and presented in the form of rating scales with specific scores out of 20 within four aspects. Then, the scores were summarized and interpreted into three categories i.e. Good, Fair and Bad.
For sensitivity analysis, the satisfaction with the patients’appearance was not derived only from the consensus of patients and their parents expressed through some questions in the questionnaire and interview but also from the results of the assessment of five interdisciplinary assessors. Four of them were medical staff from the CLP care team at the Tawanchai Center who were experts in the medical field while one assessor was a lay person outside the medical field. All of these assessors were well informed of the method and the criteria before assessing the patients’ appearance.
2.5. Ethical Considerations
None of the variables or data used in this study allowed an individual to be identified. Confidentiality in this study was considered where relevant. The obligation to protect and promote the nondisclosure of information imparted in a relationship of trust lies at the core of the concept of confidentiality. This study was certified by Khon Kaen University Ethics Committee on Research (referred to with the number 631531). In spite of this policy based on the ethical concern, one of the samples with his parents was asked for permission to show some parts of his photos with his eyes covered for publication with anonymity. Thus, the photos were the result of their consensus and ethical consent which is internationally acceptable in a medical field.
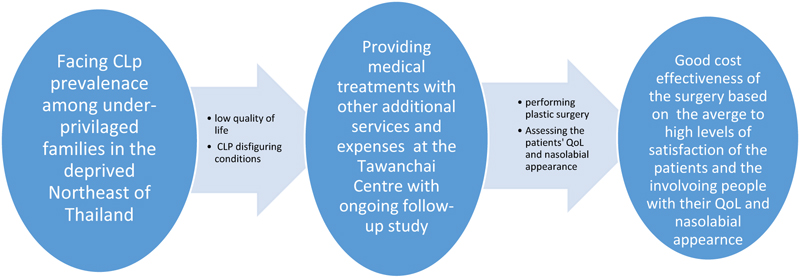
2.6. Conceptual Framework
CLP among live births is more prevalent in the deprived Northeast of Thailand. It is a disfiguring condition that causes great concerns in underprivileged preteen patients who worry about their appearance and how they are perceived by others. Parents of these patients also worry overwhelmingly about their children’s congenital craniofacial abnormality as well as the high cost of plastic surgery and other expenses. Hence, there is a need to assess the cost-effectiveness of surgery based on the patients’ satisfaction with their QoL and nasolabial appearance. The evaluation yields the desired outcome on the cost-effectiveness of plastic surgery for Thai preteen CLP patients shown through the “Average” to “High” satisfaction with their QoL and nasolabial appearance shown in Fig. (2).
3. RESULTS
The findings showed that a little more than half of the patients were boys (16 out of 30; 53.3%). More than half of patients had complete unilateral CLP (19 out of 30, 63.3%). Most of the patients (22 out of 30, 73.3%) were cared for by their parents. All the medical costs of the patients (100%) were financially supported by the government because most of them were poor and only about a quarter of their parents (9 out of 30, 30%) could earn 5, 001 to 10, 000 baht per month as shown in Table 1.
Retrieved from Tawanchai Center Database, with permission of Tawanchai Center
Retrieved from Tawanchai Center Database, with permission of Tawanchai Center
| Data | Percentage/ Mean |
|---|---|
| Genders | |
| Male | 16 (53.3) |
| Female | 14 (46.7) |
| Age 8-12 years old | Average 9 years old |
| Types of Cleft lip-cleft palate | |
| Unilateral cleft lip-cleft palate | 19 (63.3) |
| Bilateral cleft lip-cleft palate | 11 (36.7) |
| Care givers | |
| Parents | 22 (73.3) |
| Grandfather/ Grandmother/ Uncle/ Aunt | 8 (26.7) |
| Health benefit schemes | |
| Universal Coverage/ Beautiful Smile, Beautiful Voice Project | 27 (90.0) |
| Civil Servant Medical Benefit Scheme | 3 (10.0) |
| Education of parents | |
| Primary school | 22 (73.3) |
| Higher primary school | 8 (26.7) |
| Family income per month (Thai baht: THB) | |
| ≤ 5,000 | 6 (20) |
| 5,001-10,000 | 9 (30) |
| 10,001-15,000 | 3 (10) |
| 15,001-20,000 | 6 (20) |
| ≥ 25,000 (3) and N/A (3) | 6 (20) |
The overall findings showed that the average patient satisfaction with their QoL based on the five dimensions rating was 3.26 ± 1.39 (Table 2). The satisfaction with services at the center, overall treatments costs, and additional costs were “High” at 4.30 ± 0.98, 3.72 ± 1.15, and 3.70 ± 1.14, respectively, whereas the parental satisfaction with psychosocial effects, including concerns about CLP effects on the family were “Average” at 3.33 ± 1.08 and 2.81 ± 1.46, respectively (Table 2).
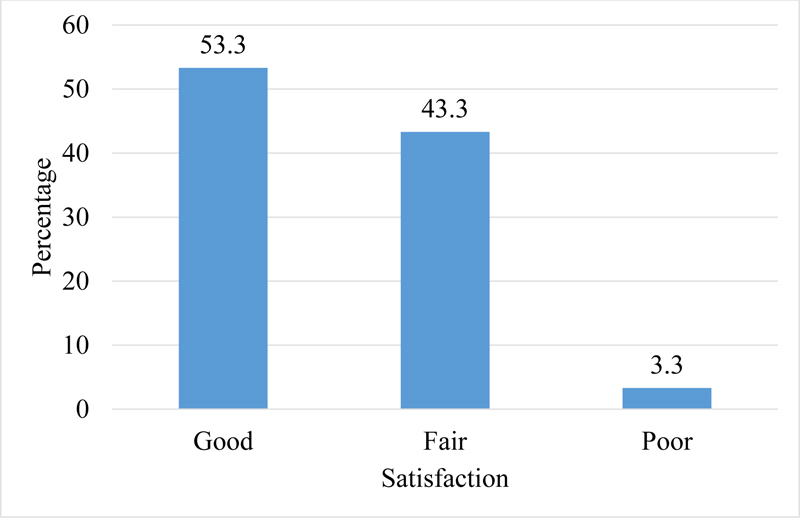
In addition, satisfaction with the patients’ nasolabial appearance was rated by five interdisciplinary assessors for four aspects i.e. nasal form, nasal symmetry, vermillion border, and nasolabial profile. Five rating scales were employed ranging from 1= very good to 5 = very poor resulting in 20 (4 X 5) scores in total for each assessor to be given. Therefore, the scores from each assessor from 4 to 20 would be summarized, then interpreted and presented within three ranges i.e. Good = 4 to 7, Fair = 8 to 13 and Poor = 14-20. These rating scales were adopted from those of Phatchrida [33]. The results of the satisfaction with the patients’ nasolabial appearance rated by five interdisciplinary assessors within three categories were presented in a bar graph as in Fig. (3).
Retrieved from Tawanchai Center Database, with permission of Tawanchai Center.
| S.No | Dimensions | Mean (x̄) | Standard Deviation (S.D.) | Coding |
|---|---|---|---|---|
| 1 | Overall Treatment: Getting access to meals, verbal practice, and development, respiratory infection, otitis media, hearing system care; Being well-informed on approaches for effective communication when bullied. | 3.72 | 1.15 | High |
| 2 | Services at the Center: Getting access to effective coordination and consultation when encountering problems; Being empowered for active participation in treatment; Being well-informed of the treatment. | 4.30 | 0.98 | High |
| 3 | Medical and Additional Costs: Access to medical privileges; Understanding where to get help; Getting access to financial support from the center such as traveling costs due to the economic condition of the family. | 3.70 | 1.14 | High |
| 4 | Parental Satisfaction: Realizing child’s satisfaction; Being satisfied not only with child’s appearance but also voice and hearing; Being free from worries about the child’s illness and troublesome behavior. | 3.33 | 1.08 | Average |
| 5 | The Effects of CLP on the Family: Negative effects: decreased income due to work leave and loss of income, accrual of additional debt; not being able to relax due to traveling or increased stress; decreased level of family happiness; having less time to take care of the other children, being exhausted due to lack of inspiration, understanding, and help from close relatives; worrying about the illness occurring in a future child; worrying about the child’s future; being concerned about the child being pitied; increased demand of attention from the ill child; child’s illness badly affecting parents’ health due to inadequate time to take care of themselves, less time to take a rest resulting in reduced sexual pleasure Positive effects: Strengthening of the family bond due to increased cooperation to solve problems; Getting more attention and support from siblings or relatives who are in good health. |
2.81 | 1.46 | Average |
| 6 | All Dimensions Combined | 3.26 | 1.39 | Average |
Retrieved from Tawanchai Center Database, with permission of Tawanchai Center
The bar graph showed that the nasolabial appearance of more than half of the patients (16 out of 30; 53.3%) was rated as “Good” with scores between 4 and 7; whereas less than half of them (13 out of 30; 43.4%) were assessed as “Fair” with scores between 8 and 13. Only one of them (1 out of 30; 3.3%) was evaluated as “Poor” with scores between 14 and 20.
In sum, it could infer from the results that all five interdisciplinary assessors were very satisfied with the appearance of the patients after the surgery based on the results of their rating were mainly “Good” and “Fair” for almost all the patients (29 out of 30; 96.66%) with just 1 (3.3%) for “Poor”.
However, while the overall results of the five raters shown above indicated a relatively high level of satisfaction in patients’ appearance as an outcome of the surgery, these results signified some relatively low correlation to some extent as shown in Table 3 below.
Retrieved from Tawanchai Center Database, with permission of Tawanchai Center
| 4-Dimensional Evaluation (4-20 Points) | Kappa Agreement Signified | p-values |
|---|---|---|
| 4 | 0.18 | 0.001* |
| 5 | -0.10 | 0.952 |
| 6 | 0.03 | 0.295 |
| 7 | -0.04 | 0.804 |
| 8 | 0.02 | 0.361 |
| 9 | -0.08 | 0.934 |
| 10 | -0.04 | 0.801 |
| 11 | -0.03 | 0.724 |
| 12 | 0.03 | 0.000* |
Although the table seems to indicate a relatively low correlation (in column 2 through the Kappa Agreement) among five raters, the raters’ agreement about satisfaction with Good appearance (4 scores in column1on the first line) was statistically significant at P = .001 (in column 3). This was strongly confirmed by their agreement about satisfaction with Poor appearance (just12 scores: no one rated more than 12 to 20 in column 1 on the last line) was statistically significant at P = .001 based on the same criteria mentioned above. This could be inferred that the five inter-examiners were highly satisfied with the patients’ appearance as the good outcome of the surgery. The assumption why their correlation of their results was relatively low would be presented in the following section i.e. Discussion below.
4. DISCUSSION
The research findings from the demographic data of 30 preteen patients aged between 8 and 12 years old were in line with earlier studies that showed that more boys than girls were diagnosed with CLP and it occurred more on the left rather than the right side of the lip.
Among the five dimensions of QoL, satisfaction with treatment, including information about dental care, was scored as “High”. The 8- to 12-years age range is the crucial time when the patients need to be prepared to have bone grafting for permanent canine teeth and orthodontic treatments. Patients need to start taking good care of their teeth during this phase [18, 28]. Actually, these patients had undergonesurgery since they were born, and they have been followed right after the surgery until they turn 20 years old. Although this study has investigated all the patients within three age ranges i.e. 4 to 6, 8-12 and 16 to 20 years old, this present study focused on the target group of patients aged between 8 to 12 years old as it is the crucial time for them with two main reasons. The first reason it is the time they become preteenagers who begin to concern about their own appearance which affected their self-esteem and the second one is it is the right time to prepare their oral cavity for alveolar bone grafting and orthodontic treatment. Thus, the other age ranges i.e. 4 to 6 and 16 to 20 are on the process of studying which will be presented later. This target group of participants would turn 8 to 12 in 2020 while collecting the data based on the results of the initial study in 2017 to 2019 after their primary surgery since the center was found in 2008.
The average to high level of satisfaction with both QoL and appearance of the patients signified the good caring of patients by their family members like parents and relatives had contributed to the “High” level of satisfaction with treatment and services. This was strongly reinforced by other related aspects of treatment like speech and language therapy and ear check-up. Also, it was strengthened by the interdisciplinary team with the good coordination of the nurses and staff members at the Tawanchai Center, which is a center of excellence in caring for patients with CLP. The center was certified by the Healthcare Accreditation Institute in 2018 and was awarded State Service in 2019 for developing good services. Thus, parents were guaranteed that patients in this center would be well-taken care of them [28]. The treatment and services were rated high by the families who were being asked these questions at the same center where they had received the treatment. The researchers were well aware of this issue that it might have caused some bias. Thus, the families and patients were reassured that their answers would not alter treatment as they all would be made anonymous based on the officially approved ethical consent from the university in order to prevent and avoid the bias of being hesitant to report anything other in fear of it affecting their child's treatment before they were asked to provide the data for the study.
In fact, the center was certified by the Healthcare Accreditation Institute in 2018 and was awarded State Service in 2019 for developing good services. Thus, parents were guaranteed that patients in this center would be well-taken care of them [28] equally. When the families were being asked these questions at the same center where they were receiving treatment, the families and patients were reassured that their answers would not alter treatment as they all would be made anonymous based on the officially approved ethical consent from the university in order to prevent and avoid the bias of being hesitant to report anything other in fear of it affecting their child's treatment before they were asked to provide the data for the study. The researchers were well aware of this issue before starting the interview.
However, as the treatment was free for all patients with financial support from the government through the Tawanchai Foundation. This included other necessary supports for additional costs such as travel, necessary medical equipment, and other related costs from the center as the foundation for these underprivileged patients and families with financial problems due to their low incomes with debt [20]. All this free help without any conditions might have caused the grateful thanks of all the patients and families for all the staff due to the influence of Buddhist belief. This grateful feeling for the kindness from others is common in Thai tradition and culture. This might inevitably have some influence on their rating to some extent.
Likewise, the satisfaction with the medical expenses was also scored as “High”. This might have been from the treatment that was offered free of charge for all patients with the financial support from the government through the Tawanchai Foundation, which also provides additional support which was not covered by the government. The psychosocial aspect and its effect on family, satisfaction levels were found to be “Average” and were predominantly due to financial problems. Most of the families had low incomes and struggled to earn extra money to pay for additional costs such as travel, necessary medical equipment, and other related costs.
Moreover, some parents had to take leave from work resulting in the loss of income and, unfortunately, more debt [20]. Others were worried about their children’s future and were afraid to give birth to more children with similar defects. These factors affected the QoL of the patients and their families. However, the Tawanchai Center has sought ways to help with travel, medical equipment, and other related costs not included in the government’s financial support. The overall expenses, including medical costs, were still lower than that provided by the government. This made it necessary for the Tawanchai Center to find other sources of financial support to effectively manage and maintain the excellent services [31] organization’s high standards.
Although many of the QoL questions seemed to concern the impact on the parents while the appearance scores were mainly based on external raters and the outcome measures were those of patient satisfaction, indeed, how the patient felt about their appearance were reflected through their parents or guardians out of their consensus. This was because both parents and their young children, especially the young ones not older than 12 were strongly influenced by local Thai culture in traditionally bringing up children in a modest and conservative manner not to express their feelings or opinions publicly, especially about their satisfaction with own appearance or others’. This particularly happened in underprivileged families like most of the patients whose parents were poor and undereducated, causing their children to hardly get access to a high standard of education and medical treatments. As a result, these children with craniofacial abnormality were reluctant or even shy to openly express their opinions, especially about their satisfaction with their own appearance. Therefore, these children with limited self-confidence predominantly relied on their parents or guardians to express all inner feelings or opinions for them in public. However, the researchers initially guided the parents to encourage their children to express their opinions as much as they could and willing to do so. Thus, it could infer that the results of the patients’ satisfaction with their appearance were from the consensus of both the parents and the patients themselves, but they were expressed by their parents. This could be assumed to be their own opinions about their own look or appearance.
The high level of satisfaction with the patients’ appearance from both the accessors and the patients themselves as well as their parents, indicated their better quality of life as their appearance which is one of the main parts of their body image (BI) strongly influences their quality of life. This was well in line with the findings of Nayir et al. [3] who strongly confirmed that body image (BI) was found as a strong predictor of QoL.
As the five experts could rate the appearance of each patient’s face as poor, fair, or good by comparing it with the face of a child without CLP, the potential confounders might have occurred from their different perspectives of beauty and their expectations out of the surgery. This included their different experiences and expertise as they are from different disciplines such as a plastic surgeon, an orthodontist, a speech pathologist, a nurse and a lay person who is outside a medical field. More importantly, as they are all human beings, it is impossible to completely control their feelings, especially when each of them had to evaluate a nasolabial appearance for four different aspects like the nasal form and symmetry and vermillion border as well as a nasolabial profile. This was assumed to inevitably influence their judgements in rating each patient’s appearance to some degree which directly resulted in the relatively low correlation among five interdisciplinary assessors.
However, the precaution for controlling potential confounders was considered to prevent and avoid or reduce this bias as much as possible. It was done through setting the criteria clearly for sample selection, giving good training on the criteria assessment for each assessor, and thorough discussions for reaching a consensus after completing the assessment.
As a result of the effective cooperation of the interdisciplinary team, especially the plastic surgeons with their completed cheiloplasty, they all rated the patients’nasolabial appearance in the same trend mainly from “Fair” to “Good” for almost all of the patients with just one patient whose appearance was rated as Poor. The results of assessing four dimensions of nasolabial appearance indicated a high level of consensus among five assessors due to the simple and understandable rating scales with the good training for all raters before the assessing process started.
This study originally evaluated the cost-effectiveness of plastic surgery for Thai preteen patients with CLP based on their satisfaction with their QoL and nasolabial appearance. Its success was expected to be a guideline for caring for other patients with similar conditions together with their families and others involved in their lives in Thailand and beyond.
We inferred that this study had obtained good cost-effectiveness represented through average to high satisfaction with QoL and nasolabial appearance accordingly for both the patients and their families. This endeavor was made possible by the high-standard interdisciplinary team that efficiently cooperated in taking good care of the patients. The study recommends longer follow-up session and systematic evaluation of the patients within each specific age range, sufficient financial support from the government and various non-profit organizations, and good management and communication among the team, patients, and their families.
CONCLUSION
The positive results in terms of “Average”to “Good” level of satisfaction with QoL and the appearance of the patients reflected by the patients, their parents and multidiscipline assessors indicated the good cost-effectiveness of the surgery reflecting the high quality of care, cooperation among the team members of the interdisciplinary staff, and efficient management of financial support for additional costs like commuting between hometowns and the center, medicines, and other necessary medical supply. All these factors contributed to the success of the study.
LIST OF ABBREVIATIONS
| CLP | = Cleft Lip and Palate |
| DCP1 | = Disease Control Priorities Project |
| CS | = Culture Standardized |
RESEARCH LIMITATIONS
According to Thai tradition and culture, children aged between 8 and 12 are still under parental supervision. Our findings might have been affected by parents’ beliefs, perspectives, attitudes, and needs. Some patients did not directly answer the questions of the interview or fill out the questionnaire by themselves, but the responses were collected through the help or with cooperation of their parents. Moreover, the tool for assessing the quality of life was developed to fit the Thai context. Thus, it is recommended to adjust the tool before using it with patients in other countries with different traditions, cultures, socio-economic status, education, etc.
AUTHORS' CONTRIBUTIONS
Palakorn Surakulprapa, Suteera Pradubwong, Kamonwan, Jenwitheesuk, Poonsak Pisek, and Bowornsilp Chowchuen as the authors of this paper designed and conducted the study, including analyzing and interpreting the data with the responsibility for its accuracy. The manuscript was edited and approved by all authors and language experts before submission.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by Khon Kaen University Ethics Committee on Research at the Center for Ethics in Human Research, Khon Kaen University, Khon Kaen, Thailand with approval number: HE 631531.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975 revised in 2013.
CONSENT FOR PUBLICATION
All study participants gave informed consent to participate in the research, which included the agreement that the results would be published.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available in zenodo.org at https://zenodo.org/record/7064134#.YxsKInZByUk, DOI Number: 10.5281/zenodo.7064134”.
STANDARDS OF REPORTING
STROBE guidelines were followed.
FUNDING
Research Center of Cleft Lip-Cleft Palate and Craniofacial Deformities, Khon Kaen University in association with “Tawanchai Project” Faculties of Medicine and Dentistry, Khon Kaen University. It is one of the widely- recognized public research universities in Asia. This research did not receive any specific grants from other funding agencies in public, commercial, or non-profit sectors.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors would like to express thanks to TopEdit (www.topeditsci.com) for its linguistic assistance for the final stage of the manuscript and to the patients and their families, the support staff at the Tawanchai Center for Cleft Lip, Cleft Palate and Craniofacial Deformities, and Khon Kaen University for financial support. We would like to acknowledge Dr. Glenn Borlace and Professor Assistant Dr. Bussabamintra Chalauisaeng for English editing via the Publication Clinic KKU, Thailand.
APPENDIX
Formula:
 with these following symbols with the outcome:
with these following symbols with the outcome:
N = total population = 613
Z = 1.96
Z2 = 3.8416
Variance: σ2 = 0.05
resulting in n =68.2746 or 68.
The whole population and the samples out of the formula calculation was shown in the following table.
The outcome of the whole population and the samples within three ranges of age were calculated through the formula presented in this table.
| Age Rage (Years Old) |
N (Population within Each Range) |
n (Average Sample) |
n (Selected Sample) |
|---|---|---|---|
| 4-6 | 108 | 11.98 | 12 |
| 8-12 | 274 | 30.39 | 30 |
| 16-20 | 231 | 25.62 | 26 |
| Total population | 613 | 68 | 68 |

