All published articles of this journal are available on ScienceDirect.

Investigating Learning Challenges from the Perspective of Nursing Students and Educators at a University in Casablanca, Morocco
Authors Info & Affiliations
Abstract
Background:
Whether in an academic or clinical setting, many students often consider nursing studies to be difficult. Identifying learning challenges could help to improve the quality of the training and students’ skills.
Objective:
This study aimed to identify the main learning challenges of nursing students.
Methods:
The study utilised a two-phase mixed methods design. First, a focus group discussion with nine teachers and tutors was conducted to explore the learning challenges observed by staff. Then, based on the results, a questionnaire was developed for 54 students to explore and estimate the frequency of learning challenges perceived by them.
Results:
The data analysis confirmed 15 major learning challenges, including cognitive challenges, consisting of theoretical gaps, and challenges related to clinical reasoning, and non-cognitive procedural and behavioural challenges. Challenges related to clinical reasoning, such as the difficulty in developing care plans (100%) and choosing care actions (90.2%), remain the most frequent regardless of the level of study.
Conclusion:
Supervisors should consider students’ learning challenges when designing, developing and implementing their educational interventions.
1. INTRODUCTION
Nursing education programs provide theoretical and clinical training to prepare students to practice nursing. The main objective is to develop the competency to offer patients comprehensive and adapted health care. Such competency requires theoretical knowledge, complex technical and attitudinal skills, and a significant capacity to integrate and transfer all of the knowledge to real clinical situations. These requirements pose a significant challenge [1].
The role of training institutions is to facilitate student learning by helping them to develop knowledge, skills and attitudes that are central to the nursing profession. However, as teachers, we have little knowledge about student learning challenges and deficits. The learning deficits are rarely defined in terms of challenges. They are described as ignorance, or lack of aptitude. In some countries, diagnosing learning deficits would rarely be considered. However, many national surveys have been conducted to diagnose learning disabilities such as dyslexia and dyspraxia among nursing students, for example in the United States [2, 3], United Kingdom [4] and Japan [5]. Because the number of students with learning disabilities continues to rise, researchers have studied student experiences and attitudes by examining the perceptions of both students [6, 7] and faculty [8]. More recent studies have focused on screening practices [9] and specific support strategies with a view to examining their implications for clinical settings [10-12]. In Morocco, the term ‘learning deficit’ often refers to a summary description of a difficulty identified individually during a formative or summative evaluation. In this paper, we are not investigating learning difficulties such as dyslexia and dyspraxia, rather the focus of our work is on the issues and barriers associated with our students’ learning.
In Morocco, the present education system is split over three levels: bachelor’s degree, master’s degree, and doctorate. The duration of the training program at the bachelor's degree is 3 years. In recent years, training institutions have adopted a competence-based approach to teaching and learning nursing sciences. Nevertheless, the educational system faces several problems. For example, the overload of the program and the limited time available for the various courses do not favour the use of active teaching methods. Some discrepancies are also observed between theoretical and clinical teaching. In addition, training institutions have little access to new information and communication technologies including clinical simulation [13]. These problems can cause considerable challenges and delays in acquiring knowledge among students. This paper will investigate the learning challenges faced by nursing students from the perspective of students and educators at a university in Casablanca, Morocco.
2. LITERATURE REVIEW
In the literature, the terminology related to ‘learning challenges’ is used to describe problems that hinder learning and leading to learning deficits [14-20]. The focus has been more on barriers and factors that impede learning than on determining the nature of learning deficits and their manifestations. For this paper, the term learning challenges refers exclusively to deficits as a lack of skills.
In pedagogical literature, learning challenges or “low achievement” is used to describe any delay in acquiring school performance [21]. Although it is a common phenomenon found in all areas of education and training, there are few studies on learning challenges in the nursing field from this angle. Researchers have examined specific challenges to learning within a clinical environment and identified some deficits such as poor relationships [20, 22], inadequate knowledge, deficient practical skills and insufficient communication skills [19].
Even with the lack of specific studies related to learning challenges in nursing, researchers have identified and tried to explain some deficits. Brown et al. [23] claimed that many nursing students do not properly understand the basic concepts related to anatomy and semiotics, which calls into question their ability to understand the most advanced approaches and procedures. This difficulty often leads students to memorize knowledge, sometimes even without understanding. According to Charlin et al. [24], health science students often learn taught material by heart. This learning strategy is called ‘on the surface’ because the knowledge learned does not stay in the memory for long and is quickly forgotten after an exam. It becomes difficult for these students to make connections between knowledge and generalizable skills built in the clinical setting.
It is well documented in the literature that nursing students have deficits in some clinical skills. According to Maamri [25], a large proportion of students do not completely manage to realize or master internship objectives. The lack of theoretical knowledge has been stated as the main reason of these deficits. Other studies have revealed that many students find it difficult to generalize their knowledge in different clinical contexts. Therefore, at the end of their training, a significant proportion of students fail to achieve the level of competence required to treat [26, 27]. Other researchers have studied the clinical reasoning process and identified some deficits such as the difficulty in selecting relevant cues [28], linking the information collected [29] and formulating clinical hypotheses or judgments [30].
Indeed, learning challenges are a major source of stress for students because of their feeling of incompetence in dealing with various patients in the clinical setting. They are especially afraid of harming the patient or making a mistake [20, 21]. This situation may impact negatively the quality of care and the safety of the patient. In addition to low self-esteem and professional misconduct, the risk of school failure and abandonment is significant. Despite the low failure rates in our context, this does not mean that students can easily overcome difficulties. These low rates can be due to a significant ability to adapt or, sometimes, the faculty’s inability to fail students; as Duffy [33-35] claims, ‘failing to fail’.
To better understand learning challenges, Duffy and Hardicre’s [34] study tried to identify the behaviours displayed by underperforming students. These behaviours include lack of motivation or interest, incoherent or erratic clinical performance, lack of knowledge, incomplete care, lack of nurse transmissions, avoidance of work and poor interpersonal skills. Based on these behaviours, Duffy and Hardicre [34] proposed an individual approach to diagnose and remediate learning deficits based on support meetings with the concerned student.
This research aims to enhance the overall understanding of students’ common learning challenges in the context of one Moroccan nursing education institution. The study considers the perceptions of teachers and students.
3. METHODOLOGY
3.1. Design
This study aimed to identify the main learning challenges of nursing students. To achieve these objectives, an exploratory and a two-phase mixed methods design was used.
3.2. Context
The research took place at a school of nursing in Casablanca, Morocco, during the 2017/2018 academic year.
3.3. Data Collection
The data collection was spread over two complementary phases.
3.3.1. The First Phase
The first phase aimed to identify the learning challenges observed by teachers and supervisors through group discussion. One focus group discussion was conducted with nine participants: five teachers from the teaching staff of the institution in question and four tutors who work at the student internship sites. The focus group discussion was held in May 2018 and lasted for 98 minutes. The principal researcher led the group following a discussion about a grid previously drafted by the principal researcher (Table 1). In our context, there is a shared understanding of the term “learning challenges” as related to “learning deficits”. The questions were sent to the participants three days before the meeting. The objective and questions were explicitly explained at the beginning of the discussion. During the focus group discussion, it was necessary to analyse the identified challenges by clarifying their manifestations, causes and possible solutions.
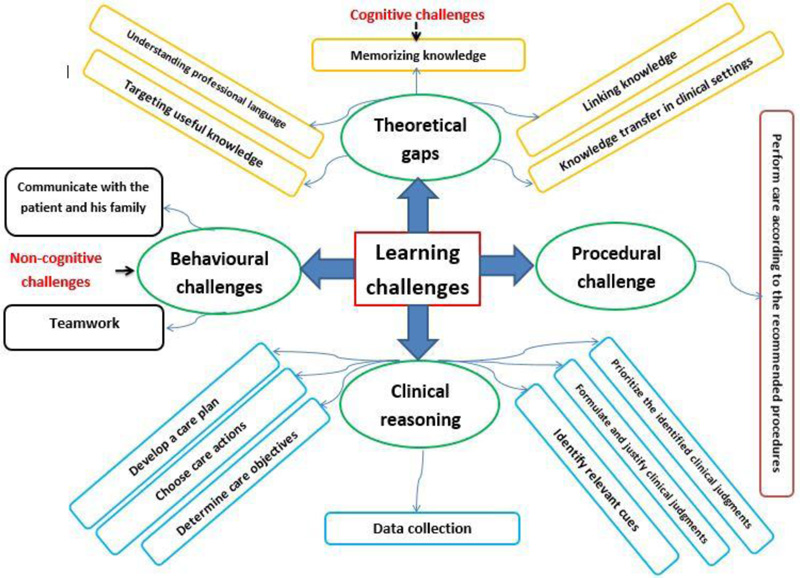
The discussion was audio recorded, and a verbatim record was transcribed for analysis. The results of the discussion were analysed to identify the learning challenges observed among nursing students. The 15 identified challenges (Fig. 1) served as a basis to develop a self-reported questionnaire for students during the second phase of the study.
3.3.2. The Second Phase
The second phase aimed to explore the nature and frequency of learning challenges perceived by students themselves. All nursing students were invited to participate in this survey (N = 54). Table 2 shows the number of students by year of study.
We chose the questionnaire as a data collection tool to cover the maximum of the target population and to collect accurate information anonymously. A 21-item questionnaire was developed for this study using data from the focus group. Students were asked to estimate the frequency of the 15 learning challenges observed by their supervisors. The questions consisted of a closed, Likert scale ranging from 1 (‘frequently’) to 4 (‘never’). This rating scale provides more accurate answers compared with Yes/No questions. An open-ended question was provided so that students could identify other learning challenges, if they existed. Last, a ‘proposals’ section was placed for them to suggest ways to overcome their learning challenges. This questionnaire was an opportunity for students to express their challenges and opinions freely. It was the moment that allowed them to speak not only about their difficulties but also their ideas and criticisms.
| Question 1 | Based on your experience as trainers, what are the learning challenges that you have observed among nursing students in academic and clinical settings? |
| Question 2 | How do these learning challenges manifest themselves? |
| Question 3 | Which causes and factors can explain these learning challenges? |
| Question 4 | In your opinion, what are the strategies to address these challenges? |
| Year of Study | Number of Students |
|---|---|
| First year | 21 |
| Second year | 19 |
| Third year | 14 |
| Total | 54 |
To validate the questionnaire, a pre-test was conducted with seven students from the nursing department of another institution. This pre-test helped to verify the degree of understanding of the questions. Unclear questions were rephrased. A brief description of the term “learning challenge” and the 15 learning challenges was appended to the questionnaire. The internal consistency (Cronbach’s alpha coefficient) of this tool was 0.782 in this study.
3.4. Data Analysis
Focus group data were audio recorded and transcribed verbatim. Then, the transcribed accounts were analysed using inductive thematic analysis [25]. Initially, the whole transcript was read several times and independently by two authors. During this phase, statements connected to ‘learning challenges’ were highlighted and reduced to meaning units. Then, initial codes and categories were individually identified and explored to determine similarities and/or differences. Initial findings were compared and discussed during another in-depth analysis of transcripts. Through researcher consensus, 15 themes, four categories and two major categories were identified (Fig. 1). Interpretations of findings were validated by the participants three weeks after the focus group discussion.
The quantitative data were analysed using SPSS version 20 for Windows. Frequency distribution of the variables was conducted in order to identify the respondents’ perceptions, and compare means and standard deviations for each variable. A one-way ANOVA was used to compare the three levels of study and identify which group was different in their perception of learning challenges. Sex and age were not significant variables in the analysis. The majority of students at all three levels of study were female (93%), so this variable was not included in the analysis. Similarly, the age of the students was identical for the whole group (age range 18-20); this did not influence their answers and was not taken into account.
3.5. Ethical Considerations
The present study obtained ethical approval from the local ethics committee of the Faculty of Health Sciences and Techniques at Mohammed VI University of Health Sciences in Casablanca, Morocco. The study was introduced and explained to all concerned nursing teachers and students, and informed consent was obtained from those who were willing to participate. They were reassured that their answers and identity would remain confidential.
4. RESULTS
Out of the 54 distributed questionnaires, 51 (n = 51) were collected, representing a response rate of 94%.
4.1. Qualitative Findings: Types of Learning Challenges
The solicited teachers report that the results from the verbatim analysis are consistent with their own perceptions based on experience. The thematic analysis revealed two major learning challenges: cognitive challenges and non-cognitive challenges. Cognitive challenges include theoretical gaps and challenges related to clinical reasoning. Non-cognitive challenges are of a procedural and behavioural nature (Fig. 1).
4.1.1. Cognitive Challenges
This main category consisted of two subcategories of challenges (Table 3).
| Cognitive challenges | Related Themes |
|---|---|
| Theoretical gaps | Memorizing Knowledge |
| Understanding professional language | |
| Targeting ‘useful’ knowledge | |
| Linking knowledge | |
| Knowledge transfer in clinical settings | |
| Challenges related to clinical reasoning | Data collection |
| Identify relevant cues | |
| Formulate and justify clinical judgments | |
| Prioritize the identified clinical judgments | |
| Determine care objectives | |
| Choose care actions | |
| Develop a care plan |
All of the participants stated that many students do not have sufficient knowledge to cope with assessments and to provide care to patients in clinical settings. According to many teachers, this challenge constitutes the direct cause of all the other deficits. As many teachers observed:
‘I think some students find it difficult to memorize knowledge. Other students do not find it very difficult to memorize knowledge, but, unfortunately, it is most often a temporary memorization because this knowledge is quickly forgotten following the exams ... This difficulty constitutes in my opinion the starting point of all the other difficulties….’ (P3)
‘An overloaded programme is one of the genuine complaints of the students… it blocks the students' ability to memorize the required knowledge’ (P1)
Understanding Professional Language
According to many participants, students encounter some challenges in understanding professional language, especially at the start of the training. Many teachers stated:
‘First-year students find it very difficult to understand medical language. This may be explained by the fact that they are entering the field of nursing for the first time…. The frequency of this challenge gradually decreases towards the end of the training….’ (P5)
‘Introducing medical terms in basic education could help nursing students understand them more quickly…’ (P3)
Targeting ‘Useful’ Knowledge
Some participants stated that many students lack the capacity to target the key elements among the knowledge taught. They are often affected by curriculum overload, as some participants noted:
‘ [I]n the face of a busy programme that includes major and other complementary courses, students must develop the ability to identify useful knowledge….’ (P4)
‘Students find it very difficult to identify and focus on the knowledge that forms the basis of the profession….’ (P2)
Linking Knowledge
Knowledge organization is an important step in the learning process. The lack of knowledge organization and the inadequacy of linking knowledge was raised within the group, with some teachers stating:
‘Many students find it difficult to link new information with already acquired knowledge. This is especially evident during exams and assessments… [when] students find it very difficult to answer questions that integrate the knowledge acquired through the different courses….’ (P6)
‘Students must learn how to link the knowledge acquired through the different courses…’ (P2)
Knowledge Transfer in Clinical Settings
The capacity to transfer knowledge acquired in the academic environment to the clinical settings, such as health-care services, is crucial in the context of nursing education. However, many teachers believed that most students lack this ability, as participants noted:
‘I believe that most students are not able to transfer what they learned to their daily practice. Usually time is spent performing usual technical care….’ (P9)
‘[O]ne day, I was with a second-year student preparing a drug for an intramuscular injection. When I asked whether the patient had a contraindication for intramuscular injection, he did not know. However, this knowledge should normally be acquired in the first year of study….’ (P1)
Data Collection
The collection of clinical data is the first step in the clinical reasoning process. The teachers claimed that many students are unable to use suitable methods to identify patient needs. As one teacher observed:
‘Usually, students spend little time in collecting clinical data… information sources are underexploited… they quickly take action and relevant information can be overlooked…. [T]his situation can have a negative impact on the quality and safety of patient care….’ (P8)
Identify Relevant Cues
According to many participants, students encounter some challenges identifying relevant cues among the collected clinical information. Many teachers stated:
‘Some students are unable to identify relevant cues that may lead to the identification of clinical problems…’ (P4)
‘Many students manage to identify lots of information related to patients’ health status... but they find it difficult to identify relevant cues among this information…. [S]ometimes important facts are overlooked….’ (P3)
Formulate and Justify Clinical Judgments
The formulation of clinical judgment is a pivotal part of the nursing profession. It leads to appropriate clinical decision-making and health promotion. However, some students lack the capacity to formulate correct nursing diagnoses. One teacher said
‘[D]espite the existence of a taxonomy of nursing diagnosis statements…. Some students cannot differentiate between medical diagnoses and nurses’ clinical judgments.... [O] thers cannot identify potential risks related to the identified cues and treatment side effects….’ (P1)
The teachers' comments suggest that the students' deficits go beyond simply identifying clinical judgments. Many participants revealed the weak capacity of some students to justify judgments identified by persuasive arguments. One teacher observed:
‘The most challenging question for students, when discussing care plans, is to justify the clinical judgments identified…. [I]t is difficult for many students to explain the clinical arguments that led to these results….’ (P7)
Prioritize the Identified Clinical Judgments
Many of the teachers participating in this study mentioned the difficulty in prioritizing the clinical judgments identified. Many teachers noted:
‘Prioritizing the patient's health problems is a core competency…All students should develop this skill…’ (P3)
‘When reading care projects developed by some students… sometimes we notice that the priority is not given to urgent problems….’ (P5)
Determine Care Objectives
Students are challenged by the inability to formulate realistic care objectives adapted to the patients’ health problems. Many teachers said:
‘Care goals are not always written in the patient's care plan… students may find it difficult to explicitly formulate goals and action plans…’ (P6)
‘[S]ometimes we notice a discrepancy between the clinical judgments identified and the formulated care goals…. [M]any students formulate unachievable goals that do not take into consideration the patient's state of health….’ (P4)
Choose Care Actions
Some students find it difficult to identify care actions adapted to patient needs. Many teachers stated the following.
‘what's often missing is the scientific reason for selecting a specific nursing action…Students often focus on technical care and ignore educational and relational action…’ (P7)
‘The care actions chosen by the students are not always sufficient.... [S]ometimes they are not in perfect harmony with the set objectives and the patients’ needs.... [I]t could be due to the lack of basic theoretical knowledge…’ (P8)
Develop a Care Plan
Students are challenged by their low capacity to write a good care plan. One teacher stated:
‘[W]riting a good care plan is not easy…. [I]t is the end of a long process that begins with the collection of a comprehensive assessment of patients' needs, including the identification of problems, objectives and care actions…. [I]f the student misses one of these steps, then I think it is completely normal that he will find it difficult to develop his care plan….’ (P2)
4.1.2. Non-cognitive Challenges
This category consisted of two subcategories of challenges (Table 4).
| Cognitive Challenges | Related Themes |
|---|---|
| Behavioural challenges | Communicate with the patient and his family |
| Teamwork | |
| Procedural challenge | Perform care according to the recommended procedures |
Students encounter some challenges in interacting with patients and their families in the clinical setting. Many teachers believed that poor communication skills were the reason for this deficit. Some teachers said:
‘There is a lack of communication between nursing students and the patients... This is due to a problem of integration within the medical teams…’ (P6)
‘Care projects developed by many students show the weaknesses of the relevant clinical cues identified with the patients and their families…. The patient interview as a way of obtaining comprehensive information is often overlooked…. This is certainly due to the lack of communication skills…’ (P7)
Teamwork
Teamwork is a necessary skill in nursing education. However, communication with members of the health-care team can be challenging for many students. As one teacher noted:
‘The majority of students fail to integrate into the health-care team…. [T]his situation constitutes a real obstacle to learning…. The relationship with the members of the team is most often limited to the execution of orders….’ (P5)
There may be several reasons for insufficient communication skills. In this regard, one of the instructors noted:
‘[I]t could be due to students’ personal characters; low self- confidence… [A]lso… the short duration of the internship periods does not help students to establish good relationships…. [T]he discrimination [too]…. Many students complain about some discriminatory behaviours in the clinical setting….’ (P9)
Perform Care According to the Recommended Procedures
In some situations, many students find it difficult to perform procedures due to the lack of necessary skills. One participant noted:
‘[M]y personal experience as a clinical supervisor shows that many students lack the necessary practical skills, especially concerning invasive procedures…. They must always be accompanied by nurses, even towards the end of the third year.... It could be due to the difficult nature of these procedures…. [I]t appears that the clinical simulation sessions are not sufficient….’ (P2)
4.2. Frequency of Learning Challenges
According to students’ perceptions, the challenges related to clinical reasoning remain the most frequent (86.5%), followed by challenges of learning declarative knowledge (74.12%) and then behavioural (69.6%) and procedural challenges (68.7%). The most frequent clinical reasoning challenges included difficulty in developing a nursing intervention plan (100%), difficulty in choosing care actions (90.2%) and difficulty in defining care objectives (90.2%) (Table 5).
4.3. Differences in Students’ Perceptions by Level
The ANOVA test revealed that there were significant differences among student groups in 3 out of 15 measuring items (Table 6). There were statistically significant differences between groups perceptions in memorising knowledge (F = 3.459, p = 0.040), linking knowledge (F = 4.873, p = 0.012) and targeting useful knowledge (F = 3.839, p = 0.028). Nevertheless, there were no statistically significant differences between groups regarding the frequency of the other challenges.
Post hoc comparisons using the Scheffe test indicated that the difficulty to memorise knowledge was significantly frequent (p=0.046) among first year students (1.75±0.90) than third year students (2.67±1.155). The frequency of linking knowledge difficulty was significantly (p=0.013) higher among first year students (1.35±0.745) than third year students (2.42±1.165). Regarding the difficulty to target useful knowledge, results showed that students’ perception of the frequency was significantly (p=0.029) higher among first year students (1.25±0.55) compared to second year students (2.00±1.15) (Table 7).
| Learning Challenges | Frequently | Occasionally | Rarely | Never (%) | Mean | Std. Deviation |
|---|---|---|---|---|---|---|
| Theoretical Gaps | ||||||
| Memorizing knowledge | 31.4 | 35.3 | 19.6 | 13.7 | 2.16 | 1.027 |
| Understanding professional language | 31.4 | 31.4 | 21.6 | 15.7 | 2.22 | 1.064 |
| Targeting useful knowledge | 58.8 | 25.5 | 9.8 | 5.9 | 1.63 | 0.894 |
| Linking knowledge | 52.9 | 23.5 | 13.7 | 9.8 | 1.8 | 1.02 |
| Knowledge transfer in clinical settings | 58.8 | 21.6 | 9.8 | 9.8 | 1.71 | 1.006 |
| Challenges related to clinical reasoning | ||||||
| Data collection | 60.8 | 17.6 | 11.8 | 9.8 | 1.71 | 1.026 |
| Identify relevant cues | 54.9 | 23.5 | 13.7 | 7.8 | 1.75 | 0.977 |
| Formulate and justify clinical judgments | 68.6 | 11.8 | 13.7 | 5.9 | 1.57 | 0.944 |
| Prioritize the identified clinical judgments | 60.8 | 27.5 | 5.9 | 5.9 | 1.57 | 0.855 |
| Determine care objectives | 54.9 | 35.3 | 3.9 | 5.9 | 1.61 | 0.827 |
| Choose care actions | 74.5 | 15.7 | 3.9 | 5.9 | 1.41 | 0.829 |
| Develop a care plan | 82.4 | 17.6 | 0 | 0 | 1.18 | 0.385 |
| Behavioural challenges | ||||||
| Communicate with the patient and his family | 39.2 | 33.3 | 17.6 | 9.8 | 1.98 | 0.99 |
| Teamwork | 19.6 | 47.1 | 19.6 | 13.7 | 2.27 | 0.94 |
| Procedural Challenge | ||||||
| Perform care according to the recommended procedures | 41.2 | 27.5 | 21.6 | 9.8 | 2 | 1.02 |
| Learning challenges | - | N | Mean | Std. Deviation | Std. Error | F | Sig. |
|---|---|---|---|---|---|---|---|
| Memorizing knowledge | First year | 21 | 1.75 | 0.91 | 0.204 | 3.459 | 0.04 |
| Second year | 19 | 2.26 | 0.933 | 0.214 | - | - | |
| Third year | 14 | 2.67 | 1.155 | 0.333 | - | - | |
| Linking knowledge | First year | 21 | 1.35 | 0.745 | 0.167 | 4.873 | 0.012 |
| Second year | 19 | 1.89 | 0.994 | 0.228 | - | - | |
| Third year | 14 | 2.42 | 1.165 | 0.336 | - | - | |
| Knowledge transfer in clinical settings | First year | 21 | 1.45 | 0.945 | 0.211 | 1.089 | 0.345 |
| Second year | 19 | 1.84 | 1.119 | 0.257 | - | - | |
| Third year | 14 | 1.92 | 0.9 | 0.26 | - | - | |
| Understanding professional language | First year | 21 | 1.8 | 0.951 | 0.213 | 2.681 | 0.079 |
| Second year | 19 | 2.47 | 1.172 | 0.269 | - | - | |
| Third year | 14 | 2.5 | 0.905 | 0.261 | - | - | |
| Targeting useful knowledge | First year | 21 | 1.25 | 0.55 | 0.123 | 3.839 | 0.028 |
| Second year | 19 | 2 | 1.155 | 0.265 | - | - | |
| Third year | 14 | 1.67 | 0.651 | 0.188 | - | - | |
| Perform care according to the recommended procedures | First year | 21 | 1.6 | 0.754 | 0.169 | 2.704 | 0.077 |
| Second year | 19 | 2.26 | 1.147 | 0.263 | - | - | |
| Third year | 14 | 2.25 | 1.055 | 0.305 | - | - | |
| Communicate with the patient and his family | First year | 21 | 1.75 | 0.91 | 0.204 | 1.771 | 0.181 |
| Second year | 19 | 1.95 | 0.911 | 0.209 | - | - | |
| Third year | 14 | 2.42 | 1.165 | 0.336 | - | - | |
| Teamwork | First year | 21 | 2.2 | 1.056 | 0.236 | 0.195 | 0.823 |
| Second year | 19 | 2.26 | 0.872 | 0.2 | - | - | |
| Third year | 14 | 2.42 | 0.9 | 0.26 | - | - | |
| Data collection | First year | 21 | 1.5 | 0.946 | 0.212 | 0.711 | 0.496 |
| Second year | 19 | 1.79 | 1.032 | 0.237 | - | - | |
| Third year | 14 | 1.92 | 1.165 | 0.336 | - | - | |
| Identify relevant cues | First year | 21 | 1.6 | 0.94 | 0.21 | 0.416 | 0.662 |
| Second year | 19 | 1.79 | 0.976 | 0.224 | - | - | |
| Third year | 14 | 1.92 | 1.084 | 0.313 | - | - | |
| Formulate and justify clinical judgments | First year | 21 | 1.45 | 0.826 | 0.185 | 0.257 | 0.774 |
| Second year | 19 | 1.63 | 1.065 | 0.244 | - | - | |
| Third year | 14 | 1.67 | 0.985 | 0.284 | - | - | |
| Prioritize the identified clinical judgments | First year | 21 | 1.5 | 0.946 | 0.212 | 0.114 | 0.893 |
| Second year | 19 | 1.63 | 0.831 | 0.191 | - | - | |
| Third year | 14 | 1.58 | 0.793 | 0.229 | - | - | |
| Determine care objectives | First year | 21 | 1.5 | 0.827 | 0.185 | 1.105 | 0.34 |
| Second year | 19 | 1.53 | 0.612 | 0.14 | - | - | |
| Third year | 14 | 1.92 | 1.084 | 0.313 | - | - | |
| Choose care actions | First year | 21 | 1.3 | 0.733 | 0.164 | 2.131 | 0.13 |
| Second year | 19 | 1.26 | 0.452 | 0.104 | - | - | |
| Third year | 14 | 1.83 | 1.267 | 0.366 | - | - | |
| Develop a care plan | First year | 21 | 1.1 | 0.308 | 0.069 | 0.679 | 0.512 |
| Second year | 19 | 1.21 | 0.419 | 0.096 | - | - | |
| Third year | 14 | 1.25 | 0.452 | 0.131 | - | - |
| Dependent variables | (I) Level | (J) Level | Mean Difference (I-J) | Std. Error | Sig. | 95% Confidence Interval | |
|---|---|---|---|---|---|---|---|
| - | - | - | - | - | - | Lower Bound | Upper Bound |
| Memorizing knowledge | First year | Second year | -0.513 | 0.314 | 0.273 | -1.31 | 0.28 |
| - | Third year | -0.917* | 0.358 | 0.046 | -1.82 | -0.01 | |
| Second year | First year | 0.513 | 0.314 | 0.273 | -0.28 | 1.31 | |
| - | Third year | -0.404 | 0.361 | 0.54 | -1.32 | 0.51 | |
| Third year | First year | 0.917* | 0.358 | 0.046 | 0.01 | 1.82 | |
| - | Second year | 0.404 | 0.361 | 0.54 | -0.51 | 1.32 | |
| Linking knowledge | First year | Second year | -0.545 | 0.304 | 0.212 | -1.31 | 0.22 |
| - | Third year | -1.067* | 0.347 | 0.013 | -1.94 | -0.19 | |
| Second year | First year | 0.545 | 0.304 | 0.212 | -0.22 | 1.31 | |
| - | Third year | -0.522 | 0.35 | 0.337 | -1.41 | 0.36 | |
| Third year | First year | 1.067* | 0.347 | 0.013 | 0.19 | 1.94 | |
| - | Second year | 0.522 | 0.35 | 0.337 | -0.36 | 1.41 | |
| Targeting useful knowledge | First year | Second year | -0.750* | 0.271 | 0.029 | -1.44 | -0.06 |
| - | Third year | -0.417 | 0.309 | 0.41 | -1.2 | 0.36 | |
| Second year | First year | 0.750* | 0.271 | 0.029 | 0.06 | 1.44 | |
| - | Third year | 0.333 | 0.312 | 0.569 | -0.46 | 1.12 | |
| Third year | First year | 0.417 | 0.309 | 0.41 | -0.36 | 1.2 | |
| - | Second year | -0.333 | 0.312 | 0.569 | -1.12 | 0.46 | |
5. DISCUSSION
The study revealed that students were challenged by a variety of deficits, and that their educators were able to identify many of these too (Fig. 1). The collected data confirms that nursing students experience challenges related to the three types of knowledge: declarative knowledge, procedural knowledge and conditional knowledge [36]. These challenges can be found in any learning environment (classrooms, internship setting) as they can be particularly evident in specific situations (e.g. apply a method of care, formulate a clinical judgment). In general, the identified challenges include a weak knowledge base, difficulty in organizing information, underdeveloped clinical skills and poor ability to solve clinical problems. This finding is similar to the study conducted by Guerrasio et al. [37], which explored medical students' perceptions of learning challenges at the University of Colorado's Faculty of Medicine.
The results also showed that teachers and students partially agreed on the frequency of the identified challenges. Indeed, the number of learning challenges identified by teachers in the four categories and their degree of frequency estimated by students suggest that the challenges related to clinical reasoning remain the most frequent, followed by challenges related to learning declarative knowledge, and then behavioural and procedural challenges. The level of study influences students’ perceptions of the frequency of three identified theoretical deficits (memorizing knowledge, linking knowledge and targeting useful knowledge). It seems that the frequency of these challenges gradually decreases towards the end of the training curriculum. However, the frequency of the other challenges remains constant even towards the third year of study. These last deficits should be considered a priority.
5.1. The challenges Related to Clinical Reasoning
Clinical reasoning is an important skill in nursing practice. There is a general consensus that it is a complex cognitive process by which students collect cues, process information, make clinical judgments by selecting from alternatives, establish goals, plan and implement interventions, and evaluate outcomes [38]. Studies show that a significant proportion of students and novice nurses [28-30, 39, 40] may lack the clinical reasoning skills to deliver safe patient care.
In this study, the frequency of clinical reasoning challenges, according to the perception of teachers and nursing students, remains very high, even towards the end of the training curriculum. These challenges involved all steps of the clinical reasoning cycle identified by Levett-Jones et al. [38]. They are observable in the middle of the internship, notably through the exploitation of individual care projects developed by students. This type of challenge often manifests itself in limited data collection, early concentration on a single clinical judgment, low ability to identify potential clinical judgements and the development of simple care plans not adapted to the real needs of patients. These results confirm the deficits identified by Demeester et al. [29], Hoffman et al. [28] and Perrier et al. [30].
To better understand the identified challenges, it seems appropriate to ask: What are the most challenging thinking strategies for students during their clinical reasoning? Based on the thinking strategies developed by Fonteyn [41], it can be deduced that students in this study find it more difficult to use the following strategies: (1) propose a statement based on a rule; (2) make a choice and provide explanations; (3) generate hypotheses; (4) order concepts by priority; (5) search for missing information; (6) conclude; and (7) recognize a pattern. Any future teaching approach must focus more on the development of these strategies.
5.2. The Challenge of Learning Declarative Knowledge
This type of challenge concerns the difficulty of linking knowledge, the difficulty of targeting knowledge useful for the exercise of the profession and the difficulty of understanding professional language, especially in the first year of study. First-year students face the highest challenge at this cognitive level compared with second- and third-year students. Many students stated that they need to work hard to understand the concepts taught in the classroom. The transition from a totally Arabized educational system to a new teaching language has been presented as the main cause by many instructors.
Thus, as soon as students are faced with an unknown concept, their course comprehension is blocked. In addition, it is evident that memorizing knowledge is not a big problem for the majority of students. Nevertheless, the knowledge is quickly forgotten after an exam. This observation is particularly noticed during continuous assessments of theoretical knowledge. The results are mostly satisfactory for questions of pure memorization, whereas they range from average to bad for questions of analysis and synthesis. Some of these results confirm the findings of Charlin et al. [24] and Brown et al. [23] concerning the difficulty in transferring and utilising knowledge in a clinical setting.
5.3. Procedural and Behavioural Challenges
The frequency of non-cognitive challenges remains low compared with the cognitive challenges mentioned above. This frequency decreases considerably towards the end of the final year of study. Thus, it appears that nursing students, at the beginning of their training, undergo a transitional stage of low self-confidence [42] that results in procedural (equipment preparation, performing invasive care following the recommended procedures) and behavioural (teamwork, interaction with the patient and his family) difficulties.
Several authors mentioned the deficiency in practical skills and the lack of communication skills as the most frequent challenges for nursing students in the clinical learning environment [18-20]. These types of difficulties mainly manifest through situations of avoidance of work, isolation and, rarely, conflict situations. The intensity of these manifestations differs among students according to their ability to overcome the shock of the first contact with the clinical environment.
Students’ lack of practical and communication skills disturbs their learning processes and makes them anxious. Several studies have found that stress and anxiety are part of the students’ experience in the clinical environment [42, 43]. These psychological problems might lead to health consequences and encourage students to leave the training.
Supervisors in this study indicated many causes that may explain the emergence of these challenges. Among these causes: inconsistency between the theoretical and practical training, students’ inadequate preparation for entering the clinical environment and inadequate support for students in the clinical environment. These causes were also advanced by Jamshidi [18] and Jamshidi et al. [19]. Moreover, it is commonly admitted, in our context, that learning opportunities are not always sufficient, and nursing students do not have enough time to practice and repeat all care procedures.
The learning challenges identified are of different natures and are interrelated. In the absence of a remediation strategy, the existence of a difficulty could lead to the appearance of several other deficits and delay the acquisition of the targeted competencies. The task of adapting courses to reflect individual needs and deficits is a prime responsibility of the teacher. Teachers can encourage deeper learning through opportunities for reflection with their students, using strategies such as blended learning and clinical simulation. It seems also relevant to use evaluation strategies that lead to production rather than memorization. The remediation of clinical deficits requires faculty to observe situations of the interaction of learners with real patients. Based on the identified deficits, supervisors may provide feedback and determine whether the learner incorporates that feedback in subsequent meetings [19].
In short, the present study contributes to a comprehensive understanding of learning challenges and their frequency in nursing education. Findings confirm some known learning deficits and categorize others, particularly those related to clinical reasoning. These results could help to adopt the most effective teaching strategies.
CONCLUSION
Starting a training program like nursing studies requires an important adaptation effort from each student. Helping to identify and solve learning challenges before problems become established and cause damage is an important responsibility of the training institutions. The teacher's role should not be limited to simple identification of these challenges. The teacher must consider them in the conception, development and implementation of various educational interventions. The different phases of teaching can be structured by taking into account these challenges. The results of this study open up several lines of research, including our project to introduce online multiple-choice questions based on clinical cases to enhance the development of clinical reasoning skills.
LIMITATION
This study provides a clear idea of learning challenges in one Moroccan institute of nursing education. However, because this was a single-site study, we cannot claim the generalizability of the findings. It is to the reader to decide the applicability of the findings to his/her own context. One further limitation is that we did not assess or address issues of learning difficulty in our students, including dyslexia and dyspraxia; these were outside the remit of the study. We acknowledge that it is possible that our students have undiagnosed issues in these areas and therefore also have unmet needs which may have had an impact on this study’s results.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the local ethics committee of the Faculty of Health Sciences and Techniques at Mohammed VI University of Health Sciences in Casablanca, Morocco.
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for studies that are the basis of this research.
CONSENT FOR PUBLICATION
Informed consent was obtained from all participants.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available from the corresponding author upon request [R.G].
FUNDING
None.
CONFLICT OF INTEREST
The author declares no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

