All published articles of this journal are available on ScienceDirect.

Issues Related to the use of a Mobile Application of the Protocol for Preventing and Managing Urinary Catheter Blockage Among Long-term Indwelling Urinary Catheter Users for Visiting Nurses: An Interview Study of Visiting Nurses in Japan
Abstract
Background:
We developed a mobile application of the protocol for preventing and managing catheter blockage among long-term indwelling catheter users for visiting nurses. We conducted meetings at four visiting nurse stations in Japan from May to June 2017 to explain the application to visiting nurses.
Objective:
The purpose of the present study was to clarify issues related to the full-scale use of this protocol application, using data from focus group interviews with visiting nurses.
Methods:
We conducted focus group interviews with the meeting participants. The focus group interviews were conducted at four different venues. Three focus groups had eight participants, and the fourth had two participants, for a total of 26 study participants. Specifically, the group interviews covered (1) the application’s structure and content; (2) operability; (3) portability; (4) possibilities for use, effects, and expectations; and (5) concerns about use.
Results:
The results of the group interviews were classified into five categories: possibilities for the use of the mobile application, possibilities for further use of the application by nurses, suggestions for the use of the application by caregivers and nursing care workers, the burden associated with the use of the mobile application, and opinions and desires for improvements in the mobile application.
Conclusion:
The results suggested that visiting nurses would use the mobile application. However, for full-scale use, it would be necessary to add the ability to use accumulated data, increase the number of learning screens, and take safety management measures for the transmission of medical information.
1. INTRODUCTION
The indwelling duration is prolonged in patients with indwelling catheters (hereafter referred to as catheters) living at home, which can result in complications such as urinary tract infection or catheter blockage [1, 2]. In particular, catheter blockage has been reported to require emergency care by visiting nurses, emergency outpatient services, or hospitalization [3, 4]. Medical expenses caused by catheter blockage are reportedly increasing [2]. In fact, approximately half of visiting nursing service users with catheters who live at home have been reported to develop catheter blockages within 6 months, and half of these patients experience repeated catheter blockages [4]. Catheter blockage may disturb the urinary flow and increase the pressure in the bladder, which may cause pyelonephritis and sepsis. Catheter blockage is induced by parenchymal conditions such as formations of biofilm or other deposits accumulating in the catheter or by the torsion and compression of the catheter [5]. The characteristics of patients who are prone to catheter blockage include a large amount of sediment in the urine, leakage of urine around the catheter, and female sex [6].
A checklist for the prevention of catheter blockage has been developed to encourage patients with spinal cord injuries to perform self-management [7]. However, this checklist was not designed to assess the risk or occurrence of catheter blockage. Therefore, considering that visiting nurses are tasked with preventing catheter blockage, assessing the presence or absence of blockages, and coping with blockages during home visits, we developed a protocol for preventing and dealing with catheter blockage among long-term indwelling catheter users for visiting nurses (henceforth referred to as “the protocol”), which consists of three sub-protocols: (1) a protocol for identifying the factors of catheter blockage; (2) a protocol for assessing catheter blockage; and (3) a protocol for dealing with catheter blockage.
We conducted a pilot study of the protocol involving visiting nurses and catheter users. The results revealed that the protocol caused errors in the observation route and order [8]. Thus, we considered it necessary to develop a mobile application of this protocol using information and communication technology, such as personal computers and tablets, to automatically guide the observation route and order. We, therefore, developed a mobile protocol application.
The use of applications has been shown to be effective for managing patients’ symptoms and for other aspects of outpatient management [9, 10]. It has also been reported that the use of learning applications for nursing techniques is effective for improving the knowledge, skills, and self-efficiency of nursing students [11, 12]. Nurses have been found to use applications to build networks with members of other professions (cited), to solve nursing problems [13], and as learning support tools. The number of reports has been increasing each year [14]. Applications for nurses have been developed in many areas and are expected to be increasingly used in nursing care settings in the future. Applications for catheter management have previously been developed for ward nurses, including the Automated Risk Assessment System [15], and for those assisting patients with catheter-associated urinary tract infection [16] to assess the risk of catheter-related urinary tract infection. These applications have started to be used in the same way that other care and health management applications are used.
In Japan, many applications for visiting nurses have been developed for the management of visit schedules and for the entry of user information or service plans. Visiting nurses are becoming familiar with these applications. However, few applications have been developed to assist visiting nurses in the process of helping service users.
The protocol application for visiting nurses examined in the present study was designed to assist nurses in preventing, assessing the presence of, and dealing with catheter blockage in visiting nursing settings. The mobile protocol application was designed to prevent errors in the observation route and order by providing automatic guidance. Although this mobile protocol application has not previously been tested in terms of its effects in actual visiting nursing settings, the efficacy of the protocol, when used on paper, has been demonstrated [8]. As the protocol has been found to be effective for preventing catheter blockage, assessing the presence/absence of such a blockage, and dealing with the development of catheter blockage, an application version of the protocol was proposed as a countermeasure against errors in the observation route and order, which were a problem with the paper-based protocol. The purpose of the present study was to clarify issues related to the full-scale use of this protocol application using data from group interviews with visiting nurses.
2. METHODS
We held meetings to explain the prototype mobile application of the protocol (Table 1) for affiliated visiting nurses at four visiting nurse stations, conducted interviews with these nurses to clarify issues related to the use of the application, and analyzed the data from these group interviews.
2.1. Participants and Data Collection Period
We recruited the participants by requesting the cooperation of a representative of the visiting nurse department and of all visiting nurse station managers working for a corporation that supervises multiple visiting nurse stations. We organized a meeting to explain the prototype mobile application of the protocol. We required that visiting nurses participate in the meeting, but we did not consider whether managerial staff were present, working form, or other factors.
We collected data using focus group interviews. The focus group interviews were held at four different venues. Three focus groups had eight participants, and the fourth had two participants, for a total of 26 study participants. The focus group interview is a method used to gather data on participants’ feelings and opinions. Data were collected from May to June 2017.
2.2. Data Collection Method
We held a meeting at each visiting nurse station. After the participants experienced the operation of the mobile protocol application, we conducted group interviews with the nurses at each visiting nurse station. Each focus group interview lasted approximately one hour or until the topic was covered to the satisfaction of the participants and the interviewer. The interviews were audio-recorded and transcribed verbatim. The interviews were conducted by the first and second authors.
2.3. Details of the Focus Group Interviews
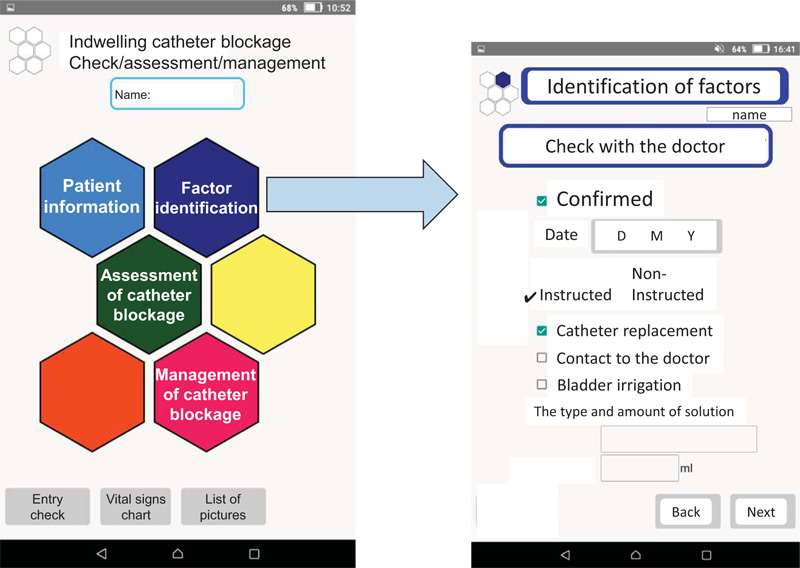
A semi-structured interview guide with open-ended questions was used. The focus group interviews covered the following topics on the mobile protocol application: (1) the application’s structure and content; (2) operability; (3) portability; (4) possibilities for use, effects, and expectations; and (5) concerns about using the application (Table 1). The contents of the focus group interviews were audio-recorded with the consent of the participants. A short questionnaire was administered to the participants at the end of each meeting. This questionnaire was used to collect data on individual attributes (years of experience working as a nurse, years of experience working as visiting nursing, presence or absence of experience with indwelling bladder catheter management, and presence or absence of experience dealing with catheter blockage). The documents explaining the mobile protocol application, which were shown to the participants, are presented in Fig. (1) and Table 2.
2.4. Data Analysis Method
We collectively analyzed the data on the 26 participants at the four visiting nurse stations instead of conducting a separate analysis for each meeting. Content analysis was used to analyze the transcript data. Content analysis was chosen because it offered a flexible method for developing and extending knowledge on the participants’ visiting nursing experiences. The second author was the primary coder of the study data. She discussed the codes with the first author throughout the coding process. If disagreement occurred, these authors referred to the original transcripts for clarification. Credibility was achieved by adopting maximum variation in the selection of participants and through prolonged engagement with the data.
(1) The attributes of the participants were tabulated.
(2) Regarding the results of the group interviews, statements were extracted from verbatim transcriptions prepared based on the recording of each group interview (Group Interviews 1 to 5). A minimum number of words were established for this extraction to ensure that the meaning of the extracted statements could be clearly understood. The content of these statements was then classified, with sentences (including a subject and a predicate) taken as the classification unit. Phrases and sentences that were not directly related to the protocol were deleted. Finally, each sentence was coded and classified into categories and subcategories containing other sentences expressing similar content.
2.5. Ethical Considerations
We obtained the approval of the institutional review board of Kanazawa Medical University for the implementation of the meetings and the data collection (I 147). This study was conducted in accordance with the Helsinki Declaration. We provided verbal and written explanations to the managers of the visiting nurse stations and to the visiting nurses regarding participation in the meeting, research participation, and the publication of the data, and we obtained written consent from all participants. The study data were not stored as identifiable information, so individuals and affiliations could not be identified. Other data were stored in a secure environment.
| Topic | Content |
|---|---|
| 1. Explanation of the protocol by the researchers | The intention, aims, and structure of the protocol and the functions and use of the mobile application were explained. |
| Operation of the mobile protocol application by the participants | When the participants operated the device, they imagined fictitious visit scenes and entered the necessary items using fictitious names for nurses and service users. |
| 3. Group interview | (1) Structure and content of the mobile protocol application |
| - | (2) Operability (ease of viewing, operating, and using the application) |
| - | (3) Portability (ease of carrying the digital tablet device) |
| - | (4) Possibilities for use, effects, and expectations |
| - | (5) Concerns about the use of the application |
| - | (6) Other topics |
| Types of Screen | Number of Screens |
|---|---|
| Startup | 1 |
| Login | 2 |
| Menu | 4 |
| User search/new creation/correction/deletion | 5 |
| Input confirmation | 1 |
| Graph of vital sign measurements | 1 |
| List of imaging results | 1 |
| Identification of factors of catheter blockage | 9 |
| Assessment of catheter blockage | 21 |
| Management of catheter blockage | 10 |
3. RESULTS
3.1. Attributes of Participants
We held meetings involving 26 visiting nurses at four visiting nurse stations. Eight nurses participated at each of three visiting nurse stations, and two nurses participated at one visiting nurse station. The mean period of experience working as a nurse was 16.4 years (range: 1–35 years), the mean period of experience working as a visiting nurse was 7.2 years (range: 1–23 years), and 25 participants had experience with managing indwelling catheters and dealing with catheter blockage (one participant had no such experience).
3.2. Group Interview Results
After the participants experienced the operation of the mobile protocol application, we conducted group interviews. The group interviews lasted 20 minutes, 21 minutes, 13 minutes, and 15 minutes at the four visiting nurse stations. A total of 61 statements were extracted from the group interviews, which we divided into 69 phrases. After deleting 22 phrases that were not directly related to the purposes of this study, the remaining 47 phrases were classified into categories and subcategories according to the similarity of the content of the phrases. The phrases were classified into five categories: possibilities for the use of the mobile application, possibilities for further use of the application by nurses, suggestions for the use of the application by caregivers and nursing care workers, the burden associated with the use of the mobile application, and opinions and desires for improvements in the mobile application (Table 3). One subcategory was defined for the category of possibilities for the use of the application, and two subcategories were defined for the other four categories.
| Category | Subcategory | Segment |
|---|---|---|
| Possibility of the use of the mobile application | 'Possibility of the use of the mobile application' | *The photo function is useful because floating and colors can be observed. |
| - | - | *(Photo function) It is good in terms of immediate data checking. |
| - | - | *It is a good tool for identifying causes of repeated blockage. |
| - | - | *Data accumulation is useful for review. |
| - | - | *No problems arise because the tablet is used at the station. |
| Burden associated with the use of the | 'Burden associated with operation' | *It takes time to enter patient information |
| mobile application | - | *Many items need to be entered. |
| - | - | *We need to enter the data twice. |
| - | - | *Difficult to operate |
| - | - | *(In the case of blockage) It is quicker to call a doctor. |
| - | - | *No time to enter the data into the tablet |
| - | - | *Not familiar with the current size (of the tablet) |
| - | - | *Hard to use when taking photos |
| - | 'Burden associated with carrying for the visit' | *It is not practical to remove the catheter while operating the tablet. |
| - | - | *It is difficult to enter the data (in the actual setting) while taking care of a patient. |
| - | - | *If I use the tablet in front of the patient, the patient may have a sense of distrust. |
| - | - | *The ordinary smartphone is easier to hold. |
| Opinions and wishes for improvements in the | 'Opinions and wishes for improvements in the contents' | *It would be better if numerical values, rather than ambiguous description, can be entered. |
| mobile application | - | *It would be better if there is a function that allows urine volume and property to be entered in a simple manner. |
| - | - | *It is unclear when the urine volume was checked. |
| - | - | *It is unclear when urine is discarded. (difficult to decide the volume) |
| - | - | *It would be better to include the technique and procedure for management of catheter blockage (Reference page). |
| - | - | *Is a reference page necessary? |
| - | - | *There are errors of Chinese characters (sand like) or spelling |
| - | 'Wishes for improvements in functions' | *It would be useful if it links to medical records. |
| - | - | *It would be useful if input data in the tablet can be used for records. |
| - | - | *It would be good if we can learn from the accumulated data. |
| - | - | *It would be useful if analysis is possible based on the differences in the amount of water and food intake. |
| - | - | *We do not need to have one tablet only for the protocol of management of catheter blockage. |
| Possibility of further use for nurses | 'Use in the nursing education' | *It may be good to use it in university classes. |
| - | - | *Effective for less experienced nurses |
| - | - | *It was useful as an educational tool for new nurses. |
| - | - | *If the necessity of care is indicated depending on the cause (of blockage), it can be used as guidance. |
| - | 'Use in cooperation tools with other professions' | *Able to report values to doctors |
| - | - | *As the recognition of hematuria may differ between a home caregiver and a nurse, a photo function would be useful. |
| - | - | *It would be good if it is used in a group home, etc. and their data can be transferred. |
| Suggestions for the use by caregivers and nursing care professions | 'Possibility of the use by caregivers and nursing care professions' | *It is easy to check if there is a function (for family members) to enter urine volume every day. |
| - | - | *It may be useful if family members use it. |
| - | - | *It may be good for unqualified persons to use it. |
| - | - | *It is good for a person who is not a family member or healthcare professional to use it. |
| - | - | *From a long-term perspective, it should be used by people in multiple job categories such as a home caregiver and therapist. |
| - | 'Possibility of having difficulty in use by caregivers and nursing care professions' | *Aged family members cannot use it. |
| - | - | *If it cannot be used by the elderly living alone, I think the use ends at that point. |
| - | - | *If it is used by a family member or home caregiver, paper media may be better because it can be corrected immediately. |
| - | - | *Terms are difficult for family members. |
| - | - | *The voice guide should be available (for family members). |
4. DISCUSSION
4.1. Points Requiring Improvement
4.1.1. Burden Associated with the use of the Mobile Application
Some participants commented about a burden associated with operating the application and carrying of the device during a home visit. Visiting nurses would be required to enter or write the regular records of their nursing visits in addition to entering information into the mobile protocol application, which would be extra work for them. Overall, 23.0% of visiting nursing records were found to be electronic in a 2015 survey [17], and this increased to 58.8% in a 2017 survey [18]. This indicates that the electronic conversion of visiting nursing records is likely to continue to grow in the future. If the mobile protocol application is incorporated into recording software, the extra work created by the application would be avoided. The burden associated with carrying the device at the time of the home visit was mainly about operating the device while also taking care of patients and about a sense of distrust toward the operation of the device. As Dorte et al. reported that users of visiting nursing have a positive impression about the use of tablet devices by nurses [19], this practice does not appear to lead to a sense of distrust among patients. Future research should investigate patient awareness and attitudes regarding visiting nurses bringing the mobile application version of the protocol with them and entering records during home visits. This protocol itself is not necessary if the prevention of catheter blockage can be performed and assistance at the time of blockage can be provided independently on the basis of information on long-term indwelling catheter users. However, the application still has the advantage of accumulating information on catheter blockages and displaying patient history in list form. Users of this protocol should be limited to visiting nurses with little experience caring for indwelling catheter users for whom the cause of catheter blockage is unknown and observations of symptoms need to be accumulated. In a set of guidelines for the development of electronic material for use in nursing practice, Chee et al. argued that “researchers should define the meanings and effects of digitalization for research projects and populations [20].” Statements made by participants in the present study regarding the burden associated with the use of the application suggested that visiting nurses did not know what the effects of the mobile application would be. It is necessary to clearly show and notify stakeholders of the effects when the system begins to be used on a large scale. Previously, several articles have reported the development of applications for use by patients [10, 21-23], but the number of studies of this type has been limited. As there is no fixed method for application development, previous work has variously reported application content/processes centering on theory [9, 10] and development driven by expert discussion and consensus [17]. Under these circumstances, it is valuable that this research clarified the viewpoint of the burden associated with the use of the mobile application.
4.1.2. Opinions and Desires for Improvements in the Mobile Application
Some participants made statements about the content of the mobile application and potential improvements in its functions. Comments regarding the application’s content were mainly related to the entry of urine volume. As the timing of urination was unknown, some participants requested ambiguity in the entry of this information, and other participants requested the ability to enter numerical values. The urine volume item needs to be examined to allow visiting nurses to enter the data in accordance with real-world conditions such as whether they are performing a direct visual check or basing their entry on reports from family members.
Other participants expressed opinions such as “Are reference pages necessary?” and “This protocol should include techniques and procedures for the management of catheter blockage.” Reference pages may be unnecessary for experienced nurses; however, these pages should not be deleted because multiple statements suggested that this protocol could be used for basic nursing education, and it is possible for the reference pages to be viewed only by those who want to see them. Bladder irrigation and catheter replacement were mentioned as aspects of dealing with catheter blockage that should be included. However, these procedures involve risks such as urethral injury caused by forced insertion, depending on the physical condition of the patient. If individual circumstances are not clear, the patient’s care should not be guided by the mobile application. Thus, we think that it would be dangerous to add detailed information on these techniques and procedures.
4.2. Suggestions for Use
4.2.1. Possibilities for the use of the Mobile Application and Possibilities for Further use of the Application by Nurses
In terms of possibilities for the use of the mobile application, participants commented that the photo function and the past data viewing function of the application could be used in visiting nursing. Participants’ comments regarding possibilities for further use of the application by nurses included ideas about using the application in nursing education, including both basic nursing education and continuing nursing education, and about using the application as an inter-professional collaboration tool. With increasing population aging and the ongoing promotion of home medical care, the number of users of visiting nursing is rapidly increasing in Japan [24]. The mobile protocol application examined in the present study provides care instructions and incorporates learning functions. Applications have begun to be used in basic nursing education and in continuing nursing education [11, 12]. A previous study found that a smartphone application providing nursing scenarios for patients with chronic diseases may play an important role in the acquisition of knowledge and the development of self-efficacy in basic nursing education [25]. However, because the protocol examined in the present study was not prepared for education, the learning screens would need to be enhanced for use in basic nursing education. Catheter blockages are strongly associated with urinary tract infections, and the application can also be used in continuing nursing education by incorporating the guidelines for the prevention of urinary tract infection into the learning screens. The application could also be used as an inter-professional collaboration tool through the sharing of accumulated patient data. However, in the transmission of medical information, the application would need to comply with the government’s Guidelines for Safety Management of Medical Information Systems, Version 5 [26]. Although security protection measures are expensive, previous work has shown that visiting nurses use private smartphones and tablets for their work at visiting nurse stations [19] and that nurses working at medical institutions in the Philippines use personal smartphones for business conversations and professional text message transmission [27], indicating the need for security measures regarding both information protection and information and communication technology device provision. Security measures related to information protection and information and communication technology devices require nurses to be knowledgeable about information and communications technology. This raises the question of how much computer literacy nurses are required to have. It has been reported that most nurses have moderate anxiety about the use of computers [28], and nurses’ computer skills are associated with their attitudes toward the introduction of information technology in nursing care [29]. In this study, we found that nurses expected various functions for application development. However, to develop these functions, it is necessary to have an educational system that improves nurses’ information and communications technology skills.
4.2.2. Suggestions for the use of the Application by Caregivers and Nursing Care Workers
The participants’ suggestions for the use of the application by caregivers and nursing care workers concerned two points: possibilities for the use of the application by caregivers and nursing care workers and the potential for difficulty in the use of the application by caregivers and nursing care workers. The latter group of comments were related to the perceived inability of older adults to operate devices such as digital tablets. Home nursing care involves not only nurses but also physiotherapists, occupational therapists, and home helpers. In home care in Japan, family members provide nursing care in addition to public services, and the timeframe over which they provide this care tends to be long and to include catheter management. It has also been reported that the observation of conditions such as urine volume and the presence or absence of fever by family members is associated with the frequency of catheter blockage [3]. Regarding the operation of the application, some study participants raised the concern that caregivers in Japan tend to be older adults, who may not be able to use the application [30]. However, because of the rapid diffusion of smartphones (from 9.7% of the population in 2010 to 75.1% in 2017) [31], we believe that caregivers, regardless of their age, will be able to use the application if its operation is simple. In a 2019 survey conducted by Hyojin et al., more than 60% of respondents in their 70s, on average, made positive comments regarding the use of a portal site [32]. Furthermore, it has been reported that older adults can adapt to using applications. In Japan, the roles of patients, family caregivers, and care workers are expanding [33]. Although the application examined in the present study cannot currently be used by caregivers and nursing care workers, it is necessary to clarify the roles of these individuals in preventing and responding to catheter blockage and to consider the possibility of developing a tool to raise awareness regarding daily observation and nursing care. Our application may contribute to the expansion of self-care, and we hope to find a way to ensure this contribution.
4.3. Limitations of the Study
A limitation of this study was that the participants were limited to four visiting nurse stations. The results may differ depending on the attributes of the visiting nurses, affiliated medical institutions, and indwelling catheter users. Furthermore, the suggestions made regarding the use of the mobile application by caregivers and nursing care workers are only speculation. In the future, we should investigate the possibilities for the use of the application by caregivers.
CONCLUSION
The group interview results revealed several issues for the use of the mobile protocol application:
1. The addition of functions of photos and data accumulation may expand the use of the application in visiting nursing care. However, accumulated data are presently only available for viewing, which is a limitation of the application.
2. It is expected that the application will be used for basic nursing education, continuing nursing education, and as a tool for cooperation with members of other professions. However, because the application was not specifically developed for education, learning screens should be added for use in nursing education. It will also be necessary to take safety management measures for the transmission of medical information if the application is to be used as a tool for cooperation with other professionals.
3. As application users are expected to increase in the future, this mobile protocol application is expected also to be used by caregivers and nursing care workers. We need to clarify the roles of these individuals in preventing and managing catheter blockage and examine the content of the application accordingly.
4. At present, visiting nurses need extra time and effort to enter information into the mobile protocol application in addition to completing the regular visiting nursing records. We need to find ways to avoid this extra work in the future, such as by incorporating the mobile protocol application into recording software.
5. The use of the mobile protocol application will be a burden for visiting nurses with sufficient knowledge and experience in the assessment and management of catheter blockage. We need to clarify the users of this protocol and the effects and aims of the mobile application.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
We obtained the approval of the Institutional Review Board of Kanazawa Medical University, Japan, for the implementation of the meetings and the data collection (I 147).
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Written informed consent was obtained from all the participants.
AVAILABILITY OF DATA AND MATERIALS
The study data were not stored as identifiable information, so individuals and affiliations could not be identified. Other data were stored in a secure environment.
FUNDING
This study was supported by a Grant-in-Aid for Scientific Research (B: No. 16H05601) for 2016–19.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
We thank Jennifer Barrett, Ph.D., from Edanz Group (www.edanzediting.com/ac) for editing a draft of this manuscript.

