All published articles of this journal are available on ScienceDirect.

Development of a Positive Psychological Capital Improvement Program for Nurses Working in a Long-Term Care Hospital
Abstract
Introduction
The aim of this study was to develop and evaluate a program to improve positive psychological capital (PsyCap) among nurses working in long-term care hospitals.
Methods
A nonequivalent control group pretest-posttest design was employed. The participants included 27 nurses in the experimental group and 26 in the control group. The program, designed to enhance hope, optimism, self-efficacy, and resilience, was developed based on the positive psychological capital intervention (PCI) model using the ADDIE process (Analysis, Design, Development, Implementation, and Evaluation).
Results
The developed program focused on contemplation, sharing experiences, and identifying strengths. The intervention demonstrated significant positive effects on professional quality of life, specifically increasing compassion satisfaction and reducing burnout, as well as enhancing organizational commitment.
Discussion
This study delineates the development process and the effectiveness of a PsyCap improvement program tailored for long-term care nurses. The program is expected to make a meaningful contribution to improving the professional quality of life and organizational commitment within this nursing demographic.
Conclusion
The findings indicate that the intervention effectively fosters a positive psychological state and improves work quality among nurses. These results encourage further research into its impact on various work environment outcomes.
1. INTRODUCTION
As life expectancy rises and many nations transition toward aging or super-aging societies, the demand for chronic disease management and geriatric rehabilitation has intensified. Consequently, long-term care infrastructures have rapidly expanded over the past decade [1, 2]. In this evolving healthcare landscape, nurses in long-term care hospitals have become essential providers, performing pivotal roles in direct patient care, safety management, and staff supervision [3]. However, these nurses face significant occupational challenges. The complexity of geriatric diseases, coupled with frequent exposure to patient mortality and the demands of end-of-life care, places them at a high risk of job stress, compassion fatigue, and burnout [4-10]. To address these issues, Positive Psychological Capital (PsyCap), a construct encompassing hope, optimism, self-efficacy, and resilience, has emerged as a promising framework for enhancing psychological well-being [5, 6].
While previous research suggests that PsyCap interventions can effectively improve job satisfaction and organizational commitment [7], there is a lack of structured programs specifically tailored to the unique environment of long-term care nursing. Therefore, this study aims to develop a PsyCap improvement program utilizing the ADDIE model and to evaluate its impact on nurses' professional quality of life and organizational commitment. By strengthening psychological competencies, this program is expected to enhance the quality of nursing services and promote workforce stability in geriatric care settings.
2. METHOD
2.1. Design
This study employed a nonequivalent control group pretest-posttest design to develop and evaluate the effects of a PsyCap improvement program for nurses in long-term care hospitals (Fig. 1).
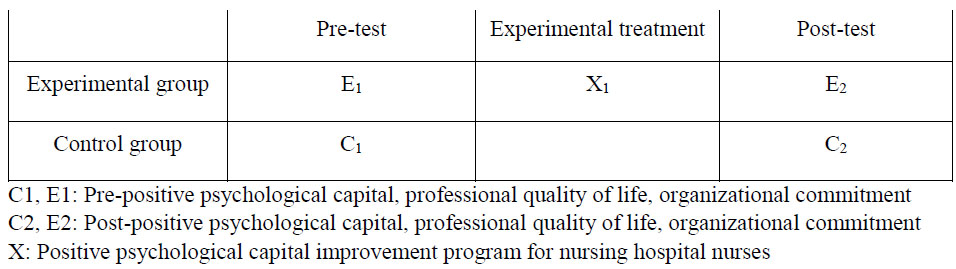
Research design.
2.2. Participants and Sample
Participants were recruited from two long-term care hospitals via official announcements on hospital bulletin boards. Prior to recruitment, formal approval was obtained from hospital directors and nursing administrators after a detailed explanation of the study’s purpose, methodology, and duration.
Inclusion criteria were as follows: (1) registered nurses providing direct patient care in long-term care hospitals; (2) those with at least six months of clinical experience in such facilities; and (3) individuals who voluntarily consented to participate.
The sample size was determined using G*Power 3.1.9.2. Based on a significance level (α) of 0.05, an effect size (d) of 0.80, and a power (1-β) of 0.80, the required size was 26 per group. To account for a potential 20% attrition rate, 60 nurses were initially recruited. Following the loss of seven participants during the study (3 from the experimental group due to resignation/withdrawal; 4 from the control group due to personal reasons), the final analysis included 53 participants: 27 in the experimental group and 26 in the control group.
2.3. Program Development and Intervention
The program was designed to enhance the four core components of PsyCa, hope, optimism, self-efficacy, and resilience, based on the Positive Psychological Capital Intervention (PCI) model [11-13]. The development process followed the ADDIE instructional design model, which systematically progresses through five stages: Analysis, Design, Development, Implementation, and Evaluation (Fig. 2). Program contents and session activities were structured by integrating findings from an extensive literature review and a needs analysis (Table 1).
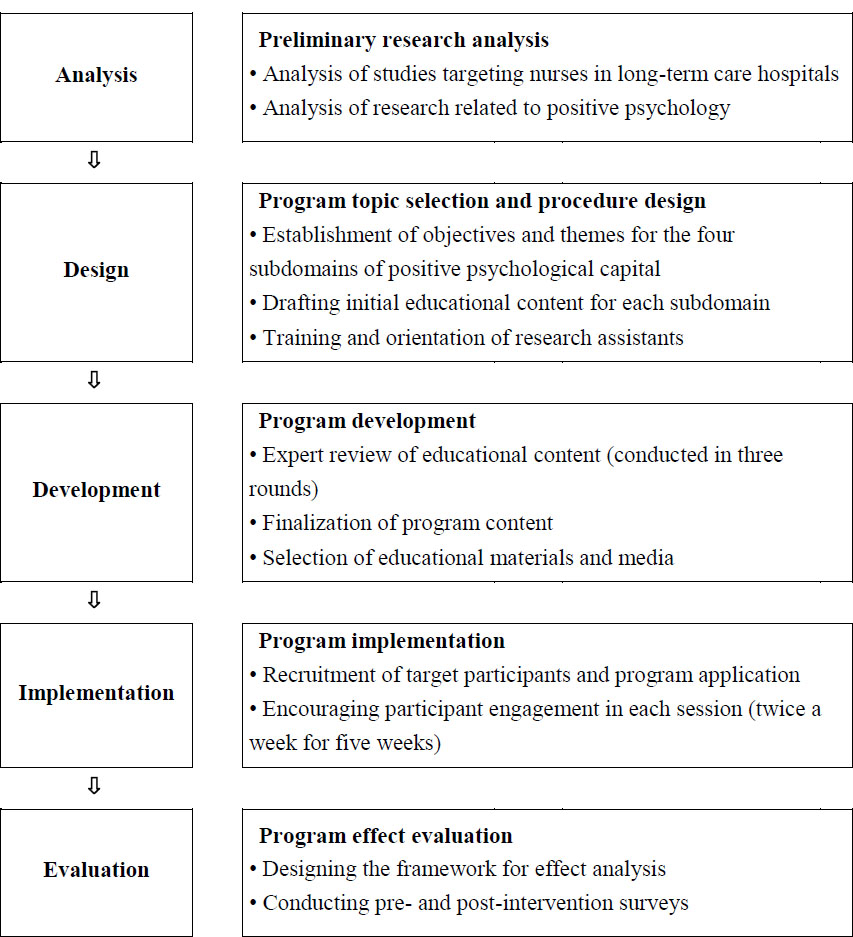
Procedure of the study.
| Session | Topic | Set Goals |
|---|---|---|
| Program introduction |
∙ Understanding programs ∙ Building trust among team members |
∙ Explain the theme and purpose of the program. ∙ Positive psychological capital can be explained in detail. ∙ You can build a sense of trust. |
| Hope | ∙ Understanding hope ∙ Understanding the path setting of hope ∙ Training to eliminate the obstruction of hope |
∙ I can explain hope. ∙ Hopeful emotions can be found through recuperation training. ∙ You can create a compensation system to get hope. |
| Optimism | ∙ Understanding optimism ∙ Learning optimism ∙ Gratitude practice |
∙ I can explain optimism. ∙ We can find optimism through recuperation training ∙ It can be carried out through optimistic learning ∙ I can express my gratitude. |
| Self-efficacy | ∙ Understanding self-efficacy ∙ Achieving positive expectations ∙ Introduction to strengths |
∙Explain self-efficacy. ∙You can discover your self-efficacy through recuperation training. ∙Share the successful experiences of senior nurses. ∙You can know your strengths and take advantage of them. |
| Resilience | ∙ Understanding resilience ∙ Remove one's own stress source ∙ Understanding one's capabilities |
∙ Explain resilience. ∙ You can discover resilience through flashback training. ∙ You can talk about your own abilities. ∙ I can make a list of resources to achieve my goals. |
To ensure the program's quality, a panel of 12 experts with extensive experience in long-term care nursing and positive psychology was consulted. The panel included three specialists in positive psychology programs, one professor of education, two professors of nursing, two physicians (a neurologist and an internist), and four nursing administrators from long-term care hospitals. Following informed consent, an open-ended survey was conducted with the panel to refine the program items. Based on their feedback, a preliminary draft was developed that reflects expert consensus on the importance and clinical relevance of each component.
The content validity of the preliminary program was assessed using the Content Validity Index (CVI). Items with a CVI of 0.80 or higher were retained. Each item was rated on a 4-point Likert scale (1 = not at all valid to 4 = very valid) to evaluate appropriateness, applicability, and effectiveness. Based on the expert review and literature synthesis, optimal instructional methods and media were selected for each session. Instructional approaches included lectures to clarify core concepts and reminiscence training to enhance participant engagement. Various supplemental materials, including specialized workbooks developed by the researcher, strength cards, and professional meditation music, were utilized to align with the program’s specific objectives.
2.4. Research Tools
2.4.1. Positive Psychological Capital
Positive psychological capital (PsyCap) was measured using the Positive Psychological Capital Questionnaire (PCQ) developed by Luthans et al. [14]. The instrument consists of 24 items, categorized into four subscales with six items each: hope, optimism, self-efficacy, and resilience. Each item is rated on a 5-point Likert scale, ranging from 1 (not at all true) to 5 (very true), where higher scores indicate higher levels of PsyCap. Items 13, 20, and 21 are reverse-coded. In the original study by Luthans et al. [14], the Cronbach’s α for the subscales were 0.75 for hope, 0.73 for optimism, 0.84 for self-efficacy, and 0.70 for resilience. In the present study, the Cronbach’s α coefficients were 0.78, 0.76, 0.77, and 0.85 for hope, optimism, self-efficacy, and resilience, respectively.
2.4.2. Professional Quality of Life
Professional quality of life was assessed using the Professional Quality of Life Scale (ProQOL) Version 5, developed by Stamm [15], and available on the official ProQOL website. The scale consists of 30 items across three subscales: Compassion Satisfaction (10 items), Secondary Traumatic Stress (10 items), and Burnout (10 items). Each item is rated on a 5-point Likert scale from 1 (Never) to 5 (Very often). Negatively worded items were reverse-coded during analysis. Higher scores indicate higher compassion satisfaction and lower levels of secondary traumatic stress and burnout. The original Cronbach’s α values reported by Stamm [15] were: compassion satisfaction = 0.88, secondary traumatic stress = 0.81, and burnout = 0.75. In the present study, the reliability coefficients were: compassion satisfaction = 0.94, secondary traumatic stress = 0.72, and burnout = 0.84.
2.4.3. Organizational Commitment
Organizational commitment was measured using the Organizational Commitment Questionnaire (OCQ), developed by Mowday et al. [16]. This instrument comprises 12 items across three subscales: affective commitment (6 items), continuance commitment (3 items), and normative commitment (3 items). Each item is rated on a 5-point Likert scale ranging from 1 (Strongly disagree) to 5 (Strongly agree), with higher scores indicating greater organizational commitment. In this study, the total score was calculated by summing all subscale scores. Mowday et al. [16] reported a Cronbach’s α of 0.79 for the overall scale. In this study, the Cronbach’s α was 0.85.
2.5. Research Hypotheses
To verify the effectiveness of the PsyCap improvement program for nurses in long-term care hospitals, the following hypotheses were established:
Hypothesis 1. The experimental group participating in the PsyCap improvement program will demonstrate higher levels of PsyCap than the control group.
H1-1. The experimental group will show higher levels of hope than the control group.
H1-2. The experimental group will show higher levels of optimism than the control group.
H1-3. The experimental group will show higher levels of self-efficacy than the control group.
H1-4. The experimental group will show higher levels of resilience than the control group.
Hypothesis 2. The experimental group participating in the program will demonstrate a higher level of professional quality of life than the control group.
H2-1. The experimental group will show higher levels of compassion satisfaction than the control group.
H2-2. The experimental group will show lower levels of secondary traumatic stress than the control group.
H2-3. The experimental group will show lower levels of burnout than the control group.
Hypothesis 3. The experimental group participating in the program will demonstrate higher levels of organizational commitment than the control group.
2.6. Data Analysis
The data collected in this study were analyzed using SPSS/PC WIN 21.0. Participants' general characteristics were analyzed using frequencies, percentages, means, and standard deviations. Homogeneity between the experimental and control groups in terms of general characteristics and pre-test scores was verified using the χ2-test and independent t-test. To test the hypotheses and evaluate the effects of the positive psychological capital program, ANCOVA and independent t-tests were performed.
2.7. Pre-test Procedure
Prior to the intervention, the purpose of the study was explained to the selected participants, and written informed consent was obtained. General characteristics and baseline data were collected using a structured questionnaire. Two trained research assistants provided instructions on completing the survey and collected the forms immediately upon completion. To ensure unbiased group assignment, participants were randomly allocated to either the experimental or control group using sequentially numbered, opaque, sealed envelopes. This concealment of allocation was maintained throughout the data collection process. The control group underwent the same pre-test procedures under identical conditions. To compensate for their time and effort, all participants received a transportation reimbursement for each session.
2.8. Post-test Procedure
Following the completion of the 10-session program over five weeks, the experimental group underwent a post-test using the same structured questionnaire. To ensure consistency in the measurement timeline, the control group completed the post-test at the same time point as the experimental group. Upon completion of the survey, transportation reimbursement was provided to all participants in both groups as a token of appreciation for their participation.
2.9. Ethical Consideration
This study was approved by the Institutional Review Board of Keimyung University (IRB No. 40525-201810-HR-96-03). Before data collection and program implementation, the researcher explained the study's purpose, procedures, and participants' rights to the nursing department heads and nurses at the two long-term care hospitals. Written informed consent was obtained from all participants. They were explicitly informed that their participation was voluntary, that they could withdraw from the study at any time without any penalty, and that their anonymity and confidentiality would be strictly maintained. All collected data were used solely for research purposes and stored securely.
3. RESULTS
3.1. Development of a Positive Psychological Capital Improvement Program
3.1.1. Analysis
3.1.1.1. Previous Studies on Nurses in Long-Term Care Hospitals
Previous studies targeting nurses in long-term care hospitals have predominantly focused on end-of-life care stress, death anxiety, and clinical competencies. However, interventions specifically aimed at personal growth or the enhancement of PsyCap remain significantly limited.
3.1.1.2. Previous Studies on Positive Psychology
Research on PsyCap improvement programs is scarce, with most interventions based on positive psychology theory being implemented through therapy, counseling, or coaching. These interventions have predominantly targeted the elderly, people with disabilities, immigrants, and specific vulnerable groups, rather than the general workforce. PsyCap has been significantly correlated with job satisfaction, reduced depression, hope, optimism, and work engagement.
3.1.2. Program Design
3.1.2.1. Conceptual Framework Design
This study developed a Positive Psychological Capital (PsyCap) improvement Program for nurses in long-term care hospitals and applied program activities aimed at improving PsyCap. The results showed improvements in PsyCap, which ultimately led to improvements in professional quality of life and organizational commitment. The program was developed and evaluated according to the PsyCap intervention model [13]. This model has demonstrated that short-term, workshop-style interventions can effectively enhance the core elements of PsyCap (self-efficacy, hope, optimism, and resilience) and positively impact organizational performance [16, 17].
3.1.2.2. Conceptual Framework Design
The program consisted of 10 sessions, designed based on the researcher’s certified training in positive psychology. Each session included various psychological stimulation activities such as positive feedback, meditation, and sharing of success stories. Pre- and post-program assessments of PsyCap were conducted before the first session and after the final session. The program aimed to help nurses maintain positive emotions even in stressful situations and to improve job satisfaction and organizational commitment. In practice, the program was found to effectively enhance both professional quality of life and organizational commitment among participating nurses (Fig. 3).
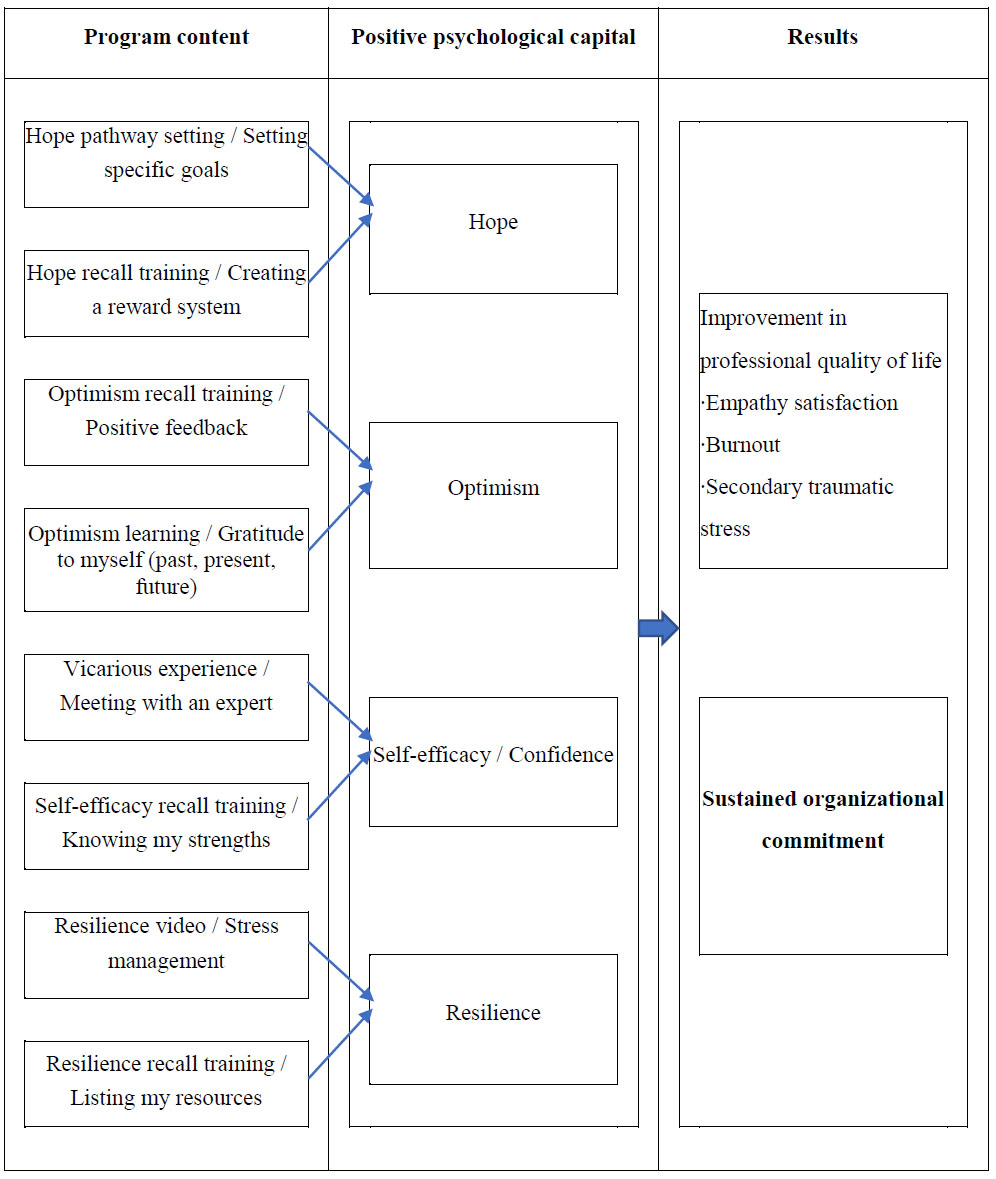
Conceptual framework of the study.
3.1.2.3. Expert Consultation Results
The initial draft of the program was developed based on a comprehensive literature review, which then underwent a two-stage expert review process for refinement. During the first round, the expert panel evaluated the draft and suggested revisions to enhance the content's relevance to the specific needs of nurses in long-term care hospitals. Following these initial adjustments, the program was further refined in a second round of review to address its practical usefulness and applicability. Key revisions during this stage included the addition of subtitles for each session topic, the creation of nickname badges reflecting specific elements of PsyCap to foster a positive identity during introductions, and the allocation of more time for post-reflection discussions to deepen participant engagement. These expert recommendations were fully incorporated into the final version of the program to ensure its content validity and practical effectiveness.
3.1.3. Program Development
The program’s appropriateness, applicability, and effectiveness were rigorously evaluated by an expert panel using the Content Validity Index (CVI). Only items receiving a score of 3 or 4 on a 4-point scale were considered valid, and a CVI threshold of 0.80 was applied for item retention. Consequently, two components, Bandura’s (2005) self-regulation checklist (CVI=.75) and distress management for patients (CVI = 0.50), were excluded from the final program due to insufficient validity scores.
Following the validity assessment, a pilot study was conducted with two research assistants to identify potential operational issues. Feedback from the trial run highlighted concerns regarding the time required to complete reverse-coded questionnaire items, the necessity for more frequent breaks during the 90-minute sessions, and the complexity of certain new PsyCap concepts. Based on these findings, the session structure was adjusted to include 30-minute segments interspersed with breaks, and the workbook was enhanced with additional explanatory materials to facilitate understanding. The final program composition was achieved by synthesizing the results from the two rounds of expert review, content validity testing, and pilot testing. This comprehensive development process ensured the structural integrity and practical feasibility of the final intervention (Table 2).
| - | Session | Title & Theme | Time (min) |
|---|---|---|---|
| 1 | Program overview (Welcome to a positive world) |
- Explanation of program process and objectives - Introduction of program rules, schedule, and content - Completion of pre-survey and consent form - Introduction to positive psychological capital and ways to enhance it - Watching a video of an athlete - Self-introduction and creating nicknames for positive psychological capital elements - Closing with “awakening positivity” (clapping) and distribution of positive stickers |
90 |
| 2 | Knowing myself (I am truly a good person) |
- Introduction to positive psychology - Introduction of 6 virtues and 24 strengths - Speed game to match 24 strengths - Strengths test to identify personal strengths and focus on key life-related strengths - Closing with “awakening positivity” (clapping), music meditation, and positive sticker distribution |
90 |
| 3 | Enhancing hope I (Hope budding) |
- Definition of hope and methods to enhance hope - Hope recall training using the workbook - Discussion on topics such as relationships with managers and promotion within the organization - Setting pathways to find hope and establishing new goals - Closing with “awakening positivity” (clapping), music meditation, and positive sticker distribution |
90 |
| 4 | Enhancing hope II (Hope blossoming) |
- Watching hope-related videos and sharing feelings - Hope recall training using the workbook - Discussion on personal economic and social issues, and relationships with colleagues - Sharing experiences from hope recall training and creating a reward system - Closing with “awakening positivity” (clapping), music meditation, and positive sticker distribution |
90 |
| 5 | Enhancing optimism I (Finding positivity in my heart) |
- Definition of optimism and ways to enhance it - Optimism recall training using a workbook - Discussion on positive events that happened in the past, present, and may happen in the future - Optimism learning through the ABCDE method - Recording and practicing finding one’s own optimism in various situations - Closing with “awakening positivity” (clapping), music meditation, and positive sticker distribution |
90 |
| 6 | Enhancing optimism II (Savoring positivity in my heart) |
- Watching optimism-related videos - Sharing feelings from the videos - Optimism recall training using a workbook - Discussion on negative events that happened in the past, present, and may happen in the future - Sharing experiences from recall training - Gratitude exercise: writing letters of thanks to past, present, and future selves - Closing with “awakening positivity” (clapping), music meditation, and positive sticker distribution |
90 |
| 7 | Enhancing Self-Efficacy I (Powerup level I) |
-Definition of self-efficacy and methods to enhance it special lecture on end-of-life care and pain management — sharing success stories and Q&A -Completing a coloring book project, using stickers and coloring to achieve goals (creating a personal masterpiece) -Closing with “awakening Positivity” (clapping), music meditation, and distribution of positive stickers |
90 |
| 8 | Enhancing self-efficacy II (Powerup level II) |
-Self-efficacy recall training (using workbook) -Reading questions about challenges overcome and problem-solving abilities, followed by group discussion -Discovering strengths using strength cards (introduced in session 2) -Sharing success stories based on discovered strengths -Closing with “awakening positivity” (clapping), music meditation, and positive sticker distribution |
90 |
| 9 | Enhancing resilience I (I can do it) |
-Definition of resilience and methods to enhance it -Resilience recall training (using workbook) -Reading questions about recent adversities, conflicts, failures, and positive experiences, followed by group discussion -Stress management -Sharing personal experiences of stress and coping strategies -Closing with “awakening positivity” (clapping), music meditation, and positive sticker distribution |
90 |
| 10 | Enhancing resilience II (I did it) |
-Orchestration session by a music instructor — about human existence and life -Resilience recall training (using workbook) -Reading questions about recent new or difficult experiences, followed by group discussion -Sharing reflections from the recall training -Creating a list of resources that helped in achieving goals -Closing with “awakening positivity” (clapping), music meditation, and positive sticker distribution |
90 |
3.1.4. Program Implementation
The PsyCap improvement program was implemented over five weeks, consisting of 10 sessions, with each session lasting 90 minutes. In the first session, participants were introduced to the program’s objectives and structure to foster a foundational understanding of the PsyCap concept. To establish a positive group identity, participants created name tags featuring positive nicknames for self-introductions. Each session concluded with a music meditation and the distribution of “positivity stickers” as a reinforcement tool. The program's content was grounded in the PsyCap framework proposed by Luthans et al. [6] and incorporated validated scales for hope [18], optimism [19], self-efficacy [20], and resilience [21]. The intervention design integrated evidence-based strategies, including reflective training, participatory activities, and a systematic reward system [13, 19-22]. To maximize participant engagement, positivity stickers were awarded for constructive contributions and active participation. In the final session, the participant with the highest number of stickers was recognized with a small prize to reinforce the positive behaviors learned throughout the program.
3.1.5. Program Evaluation
The effectiveness of the program was evaluated through a pre- and post-test design conducted over the five-week intervention period. The primary outcome measures included positive psychological capital, professional quality of life, and organizational commitment. The participants were predominantly in their 40s, with clinical experience spanning from less than 10 years to over 20 years. To ensure the internal validity of the study, the homogeneity of baseline variables between the experimental and control groups was first verified using independent t-tests and chi-square tests. Subsequently, the study hypotheses were tested by comparing the mean differences in pre- and post-test scores between the two groups. Statistical analyses were performed to determine whether the PsyCap improvement program led to significant positive changes in the target variables compared to the control group.
4. EFFECTS OF THE POSITIVE PSYCHOLOGICAL CAPITAL IMPROVEMENT PROGRAM
4.1. Homogeneity Test
4.1.1. Homogeneity of General Characteristics
An examination of the general characteristics of the participants (nurses at long-term care hospitals) revealed the following: The mean age was 46.93±10.08 for the experimental group and 46.81±10.59 for the control group. In terms of marital status, most participants were married, with 22 (81.5%) in the experimental group and 20 (76.9%) in the control group. Regarding gender, the majority were female: 26 (96.3%) in the experimental group and 24 (92.3%) in the control group. The mean clinical experience was 14.30±8.48 years for the experimental group and 12.69±7.77 years for the control group. The largest proportion of participants in both groups had 10 to less than 20 years of experience:12 (50%) in the experimental group and 8 (36.4%) in the control group. In terms of job position, most participants were staff nurses: 24 (88.9%) in the experimental group and 23 (88.5%) in the control group. Regarding shift type, rotating shifts were reported by 13 (48.1%) in the experimental group and 13 (50%) in the control group. Statistical analysis confirmed no significant differences between the two groups in any of these characteristics, thereby ensuring group homogeneity (Table 3).
| Characteristic | Sortation | Experimental Group (n=27) | Control Group (n=26) | χ2 / t | p |
|---|---|---|---|---|---|
| n(%) or Mean±SD | |||||
| Age (age) | ≥30 | 8(29.6) | 7(26.9) | 0.48 | 0.976 |
| 40 | 9(33.3) | 9(34.6) | - | - | |
| 50≤ | 10(37.0) | 10(38.5) | - | - | |
| 46.93±10.08 | 46.81±10.59 | 0.42 | 0.967 | ||
| Marriage | Single | 5(18.5) | 6(23.1) | 0.16 | 0.682 |
| Married | 22(81.5) | 20(76.9) | - | - | |
| Gender | Women | 26(96.3) | 24(92.3) | 0.39 | 0.530 |
| Men | 1(3.7) | 2(7.7) | - | - | |
| Clinical experience (years) | ≥10 | 6(25.0) | 10(45.5) | 2.11 | 0.347 |
| 10-20 | 12(50.0) | 8(36.4) | - | - | |
| 20≤ | 6(25.0) | 4(18.2) | - | - | |
| 14.30±8.48 | 12.69±7.77 | 0.71 | 0.476 | ||
| Position | Nurse | 24(88.9) | 23(88.5) | 0.01 | 0.961 |
| Chief nurse | 3(11.1) | 3(11.5) | - | - | |
| Type of work | Alternation | 13(48.1) | 13(50.0) | 0.01 | 0.893 |
| Comparative stand | 14(51.9) | 13(50.0) | - | - | |
4.1.2. Homogeneity of Dependent Variables
Homogeneity of baseline dependent variables between the experimental and control groups was tested. No significant differences were found, indicating equivalence across most variables. However, the “hope” subscale of positive psychological capital showed a statistically significant difference between groups (Table 4).
| Characteristic | Experimental Group (n=27) | Control Group (n=26) | t | p |
|---|---|---|---|---|
| n(%) or Mean±SD | ||||
| Positive psychological capital | 3.16±0.56 | 3.46±0.58 | -1.92 | 0.060 |
| Hope | 3.22±0.61 | 3.60±0.61 | -2.30 | 0.025 |
| Optimism | 3.10±0.58 | 3.43±0.63 | -2.01 | 0.051 |
| Self-efficacy | 3.18±0.60 | 3.31±0.60 | -0.81 | 0.417 |
| Resilience | 3.15±0.63 | 3.50±0.65 | -2.01 | 0.050 |
| Professional quality of life | 2.81±0.20 | 2.84±0.28 | -0.44 | 0.661 |
| Satisfied with empathy | 3.31±0.57 | 3.58±0.80 | -1.41 | 0.162 |
| Secondary traumatic stress | 2.57±0.43 | 2.57±0.45 | 0.04 | 0.967 |
| Exhaustion | 2.54±0.50 | 2.37±0.52 | 1.25 | 0.216 |
| Organizational commitment | 2.68±0.54 | 2.92±0.64 | -1.49 | 0.142 |
4.2. Hypothesis Test
Prior to hypothesis testing, normality and baseline homogeneity were assessed for all general characteristics and dependent variables. No significant differences were found in the baseline scores for optimism, self-efficacy, resilience, compassion satisfaction, secondary traumatic stress, and burnout. However, as homogeneity was not met for hope, an ANCOVA was performed using the pre-test scores as a covariate. All other hypotheses were tested using independent t-tests.
4.2.1. Hypothesis 1: PsyCap Improvement
H1-1 (Hope): After program participation, the hope score was significantly higher in the experimental group (M=3.93, SD=0.49) than in the control group (M=3.52, SD=0.61; F=41.56, p<0.001).
H1-2 (Optimism): Post-intervention, optimism was significantly higher in the experimental group (M=3.78, SD=0.56) compared to the control group (M=3.43, SD=0.60; t=21.67, p<0.001).
H1-3 (Self-efficacy): Post-intervention, self-efficacy was significantly higher in the experimental group (M=3.80, SD=0.54) than in the control group (M=3.39, SD=0.63; t=26.27, p<0.001).
H1-4 (Resilience): After the program, resilience scores were significantly higher in the experimental group (M=3.86, SD=0.62) compared to the control group (M=3.46, SD=0.71; t=34.35, p<0.001). (Table 5).
| Characteristic | Experimental Group (n=27) | Control Group (n=26) | t/ F | p |
|---|---|---|---|---|
| n(%) or Mean±SD | ||||
| Hope* | 3.93±0.49 | 3.52±0.61 | 41.56 | <0.001 |
| Optimism | 3.78±0.56 | 3.43±0.60 | 21.67 | <0.001 |
| Self-efficacy | 3.80±0.54 | 3.39±0.63 | 26.27 | <0.001 |
| Resilience | 3.86±0.62 | 3.46±0.71 | 34.34 | <0.001 |
| Satisfied with empathy | 3.84±0.59 | 3.46±0.84 | -4.99 | <0.001 |
| Secondary traumatic stress | 2.32±0.54 | 2.52±0.54 | 0.47 | 0.637 |
| Exhaustion | 2.14±0.56 | 2.39±0.56 | 4.17 | <0.001 |
| Organizational commitment | 3.00±0.51 | 2.67±0.53 | -2.98 | 0.006 |
Note: *ANCOVA conducted with the covariate of pretest score.
4.2.2. Hypothesis 2: Professional Quality of Life
H2-1 (Compassion satisfaction): The compassion satisfaction score was significantly higher in the experimental group (M=3.84, SD=0.59) than in the control group (M=3.46, SD=0.84) (t=-4.99, p<0.001).
H2-2 (Secondary traumatic stress): Post-test results showed that the experimental group had slightly higher levels of secondary traumatic stress than the control group, but this difference was not statistically significant.
H2-3 (Burnout): Burnout levels were significantly lower in the experimental group (M=2.14, SD=0.56) than in the control group (M=2.39, SD=0.56; t=4.17, p<0.001).
5. DISCUSSION
The purpose of this study was to develop and evaluate a PsyCap improvement program for nurses in long-term care hospitals. The findings indicated significant improvements in PsyCap, compassion satisfaction, burnout, and organizational commitment in the experimental group compared to the control group.
5.1. Development of the Positive Psychological Capital Improvement Program
This study was conducted to develop a Positive Psychological Capital (PsyCap) improvement program tailored for nurses in long-term care hospitals and to verify its effectiveness. The program was systematically developed using the ADDIE model (Analysis, Design, Development, Implementation, and Evaluation) to ensure a robust and evidence-based intervention. In the analysis phase, a comprehensive review of the work environment of long-term care nurses [7, 8, 20] confirmed a critical need for psychological support, particularly as these nurses face high levels of end-of-life care stress and burnout. While previous PsyCap interventions have primarily focused on student populations [11, 23], this study distinguishes itself by targeting professional nurses in high-stress clinical settings, addressing a significant gap in existing literature. While considering the design and development phases, the program’s content was established through a multidisciplinary Delphi method, ensuring high content validity (CVI ≥ 0.80). Unlike conventional short-term workshops, this program was structured into 10 sessions over five weeks. This longitudinal approach aligns with meta-analytical recommendations [22-24] suggesting that sustained interventions are more effective for behavioral and psychological change.
A unique feature of this program is the integration of reminiscence training, art therapy, and music meditation. Strength cards [25] and gratitude practices [26] were designed to help participants internalize positive emotions, which is crucial for maintaining resilience in challenging geriatric care environments. Furthermore, by offering flexible participation options to accommodate shift workers, the program demonstrated high practical feasibility. These systematic development processes and tailored intervention strategies are considered key factors in enhancing compassion satisfaction and reducing burnout among the participants.
5.2. Effects of the Positive Psychological Capital Improvement Program
Following the five-week PsyCap improvement program, the experimental group demonstrated significantly higher levels of hope, optimism, self-efficacy, and resilience compared to the control group. Furthermore, significant improvements were observed in compassion satisfaction and organizational commitment, accompanied by a significant reduction in burnout.
The observed reduction in burnout and the concurrent increase in compassion satisfaction align with previous intervention studies targeting healthcare professionals [27, 28]. This effectiveness may be attributed to the cognitive-behavioral components integrated into the program. For instance, the 'Enhancing Optimism' module (Session 5), which utilized the ABCDE method to reframe negative perceptions, likely equipped nurses with the psychological tools necessary to manage the intense emotional labor inherent in geriatric care. While long-term care nurses are frequently exposed to 'compassion fatigue' due to the chronic nature of patients' illnesses and cognitive decline, enhancing resilience and self-efficacy serves as a vital psychological buffer [5]. Unlike acute care settings, where stressors are often episodic, the repetitive and prolonged stress in long-term care necessitates the sustained hope and resilience fostered by this five-week intervention to prevent emotional exhaustion from escalating into chronic burnout.
The significant improvement in organizational commitment underscores PsyCap as a critical antecedent to organizational performance. This finding supports the theoretical framework of Luthans et al. [5, 13], who posited that hopeful and self-efficacious employees demonstrate greater commitment to organizational goals. In the context of long-term care hospitals, which often face high turnover rates, the 'Hope Blossoming' session (Session 4) enabled nurses to re-examine their professional pathways and find intrinsic meaning in their roles. By aligning personal professional growth with institutional objectives, the program successfully translated individual psychological development into organizational loyalty. This suggests that PsyCap interventions are not merely well-being initiatives but strategic human resource management tools for enhancing nurse retention in aging societies [29].
Conversely, no statistically significant difference was found in secondary traumatic stress (STS) between the two groups, contradicting results from emergency room or intensive care unit settings [27, 30]. This discrepancy may be explained by the unique clinical environment of long-term care hospitals. Nurses in these settings are more frequently exposed to 'indirect grief' from the gradual deterioration of long-term residents, rather than the acute, sudden traumatic deaths prevalent in emergency departments. Consequently, baseline STS levels may not have been sufficiently high to exhibit dramatic changes within a five-week period. Furthermore, as STS is deeply influenced by organizational culture and peer support [28], individual-centered PsyCap programs may have inherent limitations in mitigating systemic trauma without concurrent organizational changes.
6. SIGNIFICANCE AND LIMITATIONS
The significance of this study lies in the development of a practical PsyCap intervention based on Luthans et al. [6], specifically for long-term care nurses. This program can be integrated into new nurse orientations and continuing education to foster positive self-perception and communication skills [23, 29-31]. However, a limitation of this study is the lack of long-term follow-up to evaluate the sustainability of the effects. Additionally, the study did not incorporate qualitative data to capture the depth of participants' lived experiences. Future research should employ mixed-methodology approaches and longitudinal designs to further validate these findings.
CONCLUSION
This study aimed to develop and evaluate the efficacy of a Positive Psychological Capital (PsyCap) improvement program tailored for nurses in long-term care hospitals, integrating reminiscence training, vicarious experiences, and diverse interactive activities. The findings demonstrated significant improvements in the core subcomponents of PsyCap: hope, optimism, self-efficacy, and resilience. Additionally, compassion satisfaction, a key dimension of professional quality of life, increased, while burnout significantly decreased. A notable enhancement in organizational commitment was also observed. These results suggest that the program serves as an effective intervention for fostering positive emotions and strengthening the psychological resources of long-term care nurses. Furthermore, the program exhibits potential for broader application across various clinical settings, including geriatric nursing.
Based on these findings, the following recommendations are proposed:
- A standardized PsyCap improvement program for long-term care nurses should be established based on the results of this study and systematically integrated into clinical training curricula.
- Further research is necessary to analyze the specific needs of long-term care nurses and to explore diverse intervention tools and methodologies aimed at enhancing PsyCap, professional quality of life, and organizational commitment.
- Replication studies should be conducted to verify whether the effectiveness of this program can be sustained across various clinical environments beyond the context of long-term care hospitals.
AUTHORS’ CONTRIBUTIONS
The authors confirm contribution to the paper as follows: M.L.: Contributed to conceptualization, methodology, and writing the draft; H.K.: Supervised the project and performed review and editing.
LIST OF ABBREVIATIONS
| PCI | = Psychological Capital Intervention |
| CVI | = Content Validity Index |
| OCQ | = Organizational Commitment Questionnaire |
| ADDIE process | = Analysis, Design, Development, Implementation, and Evaluation |
| STS | = Secondary Traumatic Stress |
| PsyCap | = Positive Psychological Capital |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was reviewed and approved by the Institutional Review Board (IRB) at Keimyung University, Republic of Korea with the approval number IRB No. 40525-201810-HR-96-03.
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
All participants provided informed consent to participate in the study and to the publication of their anonymized case details.
ACKNOWLEDGEMENTS
Declared none.

