All published articles of this journal are available on ScienceDirect.

The Effect of a Discharge Education Program on Mother’s Preparedness for Late-Preterm Infants Discharged from the NICU: A Quasi-Experimental Study Protocol
Abstract
Background
Home care of late preterm infants (LPIs) can be challenging for mothers after hospital discharge because they are more vulnerable than full-term infants and experience higher hospital admission rates.
Purpose
This study aims to determine the effect of a thorough and collaborative discharge education program offered by a nurse to mothers of LPIs. The program focuses on the mother’s preparedness (self-efficacy and readiness) to care for their LPIs at home after discharge from the neonatal intensive care unit.
Methods
A quasi-experimental design will be applied in a large, accredited referral NICU in Jordan. Two groups of mothers will be enrolled using convenience sampling. The experimental group will receive the designed pre-discharge education, and the comparison group will receive routine discharge instructions for LPI care at home. The outcome will measure a mother’s self-efficacy and readiness to care for their LPI at home. Data will be compared within and between the groups before and after the intervention. An independent and paired sample t-test will be used for analysis.
Results/Discussion
This study will be conducted on the notion that educating mothers is a principal role for neonatal nurses and helps improve the quality of healthcare services provided to parents of vulnerable infants.
Implications for Nursing
The study findings will provide insight into national and global neonatal nursing practices through a thorough discharge education program for mothers with LPIs.
Conclusion
Publishing a research protocol encourages research transparency and allows the exchange of methodological insights and feedback between academic and clinical communities.
1. INTRODUCTION
Preterm infants are born before 37 weeks of gestation [1] and late-preterm infants (LPIs) are a unique group of preterm infants born between 34 0/7 and 36 6/7 weeks of gestation [2]. As LPIs are near term, they are close enough to full term and maturity; therefore, their survival rate is much higher than that of other preterm infants born at less than 34 weeks [3]. However, LPIs are still more vulnerable than full-term infants and experience higher hospital admission rates [4]. Owing to their physiological immaturity, LPIs are more likely than term infants to experience morbidities requiring hospital care, such as respiratory distress, hyperbilirubinemia, and hypo- glycemia [5]. Sometimes, LPIs require relatively little medical and nursing support until they are mature enough to be discharged [6]. Specialized hospital care is essential for preterm infants' long-term health and well-being, as they require continuity and consistency of a mother’s care after discharge [7].
A recent systematic review by Govindaswamy et al. (2019) highlighted that mothers of infants with near-term conditions require precise and accurate information as well as good communication from healthcare providers. The primary areas of concern revolve around the provision of sensitive care for LPIs and active engagement of mothers in the decision-making process [8]. The primary source of stress experienced by parents is the change in their responsibilities, which is closely followed by concerns related to the physical appearance of their LPI [8].
In contrast, a scoping review by Maghaireh et al. (2016) showed that parents of infants admitted to the NICU change their parental roles, which negatively affect the family system by affecting the behaviors, duties, thinking, and the overall impact exhibited by the parents towards infants. Specifically, a scoping review of parents who had LPIs also found that they experienced little support at home and feared assuming full responsibility for their LPI, which may cause them to deteriorate and require readmission to the hospital after discharge [9]. Mothers need informative support and an enhanced sense of ability to provide care, such as changing diapers, providing baths, feeding, temperature checks, and skin-to-skin contact [10, 11]. Mothers have the potential to positively perceive the home care process through proactive efforts to adequately equip them to assume responsibility for home care [10].
A systematic review by Smith et al. (2022) showed that post-birth discharge education is widely used in NICUs, however, the evidence is far from forming evidence-based practices, and further research is needed to evaluate discharge preparation and a sense of preparedness for mothers (and parents) of LPIs, as well as the effectiveness of different approaches to pre-discharge education on expected outcomes [12]. Accordingly, the evidence and practices of mothers' preparedness for LPI discharge from the NICU need to be investigated. There is a need for research examining pre-discharge education programs that focus on and involve mothers with LPIs in response to this limitation and the gap in research and practice.
This paper presents a study protocol designed to examine the effect of an evidence-based discharge education intervention on mothers' concerns and the need for adequate and quality care for their LPI at home and to promote the health and well-being of infants after discharge from the NICU.
2. METHODOLOGY
2.1. Design
A quasi-experimental design will be used to assess the effectiveness of a discharge education program in improving self-efficacy and preparedness among mothers of LPIs. This design will involve non-equivalent experimental and comparison groups, no randomization, and pre-post-intervention observations. The intervention group will receive a face-to-face pre-discharge education session with an expert neonatal nurse and the researcher. The nurse (Advanced nurse specialist) will demonstrate a hands-on interactive training intervention and the education will be facilitated by a structured, colorful booklet containing essential information about home-based LPI care. The comparison group will receive usual care, including routine education training in the postpartum care unit by the assigned staff nurse working in this ward.
2.2. Setting
The preterm dyad participants were selected from an accredited NICU and postpartum unit by the Health Care Accreditation Council (HCAC) as a Baby-Friendly hospital in 2022. The Baby-Friendly Hospital Initiative is a recognized program endorsed by the United Nations Children's Fund and World Health Organization [13]. Therefore, by selecting mothers from a Baby-Friendly hospital, the study ensures that mothers with LPIs have been exposed to an environment that prioritizes and encourages breastfeeding, which may have a positive impact on their breastfeeding self-efficacy and preparedness after discharge.
The selected NICU is located in one of the largest medical centers in Jordan. Medical centers are government-operated referral centers that serve a wide range of rural and urban areas in Jordan. The postnatal ward of this institution is a specialized maternal and neonatal ward with 64 beds. The occupancy rate in the ward is approximately 30-40 cases each day, with approximately 15 mothers giving birth each day.
Recently, postnatal units have established private comfortable rooms specially equipped to support maternal breastfeeding. The researcher selected a breastfeeding room to conduct the LPI-mother discharge education program because of its privacy, comfortable furniture, and availability. These features make the room more controlled and conducive to learning at the bedside of LPIs.
2.3. Population, Sample, and Sampling
The target population of this study is all mothers of LPIs who are discharged from the NICU the study setting and who meet the eligibility criteria. Mothers need to comprehend Arabic and have their infants at 340/7 -366/7 weeks of gestation. However, mothers of high-risk infants (e.g., severe growth retardation at birth, congenital anomalies, or need for respiratory support at home) will not be eligible to participate as this may affect the study variables and the mother's transition [14]. The literature also suggests that the mother’s condition may affect their self-efficacy and preparedness to care for their LPIs [15, 16]. Consequently, mothers who require further observation of their physical or psychological condition, according to mother of LPIs medical diagnosis, will not be eligible to participate.
2.4. Sample Size
This study's fully powered sample size was estimated using G Power (Version 3.1.9.4). The calculation will use an independent sample t-test (two groups, one-tailed) while considering the following parameters: 0.80 (1-β) power level, 0.05 significance level, and a medium effect size (0.5) will be selected for convenience. Accordingly, the sample size will be 120 participants, increasing to 144 participants, with 72 in each group to account for possible attrition of 20% of the total sample size, as well as a low response rate and missing data.
2.5. Sampling Procedure
A non-probability convenience sampling will be used to non-randomly select participants for each group. The comparison group will be recruited first for data collection and then the intervention group will be approached, preventing intervention contamination between the two groups since this study will be conducted in one setting.
Before inviting the mothers to participate, the researcher will verify, from the hospital records and hospital staff, that they meet the eligibility criteria. Initially, the researcher will first ask for a list of eligible preterm infants admitted to the NICU. The researcher will then communicate with mothers who meet the eligibility criteria, addressing environmental and personal/ behavioral barriers using active listening, empathy, respect, feedback, and verbal and nonverbal cues [17].
The researcher will invite and enroll the participants by meeting them face-to-face. The researcher will start by introducing herself and explaining the investigation to the mother as per the ethical guidelines. Mothers who agree to participate and sign the consent forms will be enrolled in the study, and the study groups will be formed accordingly.
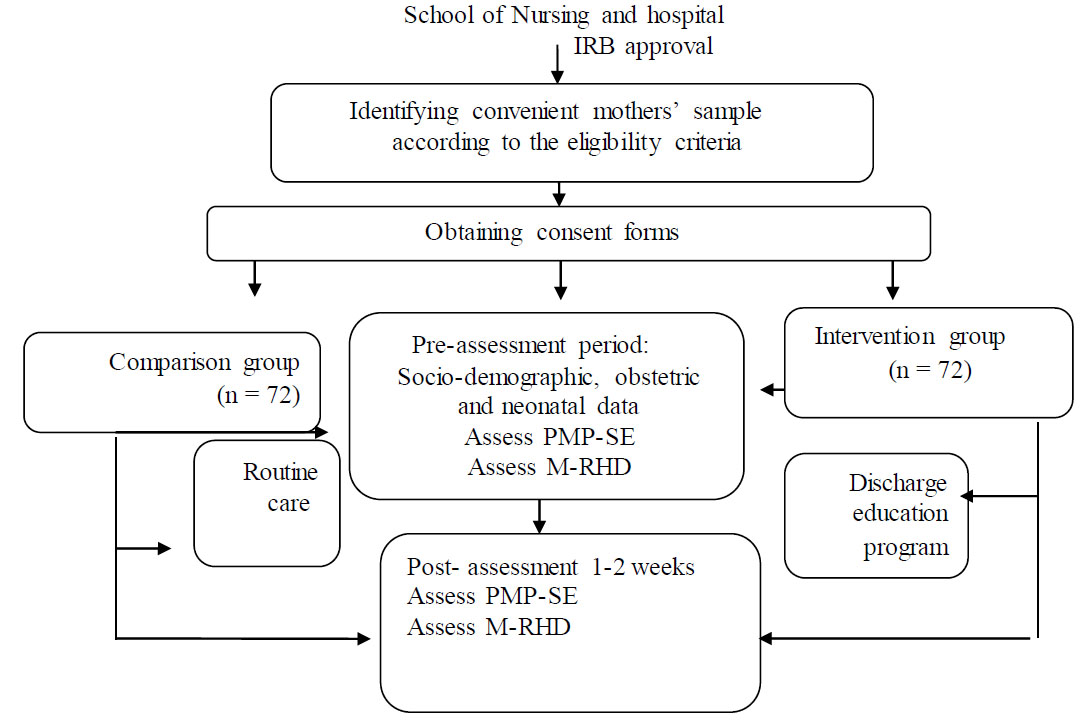
Data collection procedure of the study.
2.6. Data Collection
The comparison group will be approached first where routine care (starting breastfeeding, bowel discharge, delayed bathing, and follow-up screening tests of infants) will be provided according to hospital standards with a group of 72 mothers.
The baseline data will be collected from both groups: socio-demographic, obstetric, and neonatal data; and the Mother’s Parenting Self-Efficacy (PMP-SE) and Maternal Readiness to Hospital Discharge (M-RHD) scales. The two groups will be separated to prevent the transfer of information provided in the education sessions to the comparison group. The mothers in the comparison group will only receive traditional predischarge care before data are collected, while the intervention group will receive a discharge education program. The posttest assessment will include administering the PMP-SE and M-RHD scales 1-2 weeks after providing education for the intervention group and routine care for the comparison group. Therefore, the researcher can evaluate the mother’s preparedness after the discharge education program (Fig. 1).
2.7. Study Intervention
2.7.1. Program Development
The program was developed based on comprehensive global guidelines and evidence-based protocols for addressing the specific needs and challenges faced by LPIs. In addition, the researcher goes with a previous literature study on LPIs to offer valuable insights and findings that can inform the development of the program, ensuring its effectiveness and relevance in improving outcomes for these vulnerable groups.
The program will comprise sections on LPIs in a booklet and is an intervention used to educate mothers. Based on the updated literature, this booklet will be guided by the National Institution of Neonatal Nurses to concentrate on the following areas: breastfeeding, thermoregulation, Kangaroo mother care, and care after discharge (e.g., bathing, eye care, umbilical care, diaper care, common issues such as jaundice or hypoglycemia, handling, positioning, and car seat care) [18]. Additionally, a behavioral sense program that supports development based on gestational age will be added. Vaccination, the typical issues mothers might face, the duration of infants’ follow-up, and other important factors will be included [18].
The primary responsibility for developing the instructional material will be take out with the researcher responsibility with expertise in pediatric nursing, making her well-suited to take on the role of developing instructional materials. The researcher’s (Advance nurse specialist with 10 years of experience in infant care) deep understanding of the subject matter and practical knowledge will ensure that the material is comprehensive, accurate, and effective in educating mothers of LPIs. The program components will be further refined through collaboration with two pediatric nursing specialists who have a minimum of 10 years’ of experience. Furthermore, the educational material will undergo consultation by a Professor specializing in neonatal care who will provide an additional review. Before conducting the main study, an Arabic translation of program content that will included in this study will be applied, along with a pilot study involving five mothers of LPIs. The purpose of this pilot study is to evaluate the program content in terms of simplicity and acceptance, as perceived by mothers' comprehension level. Thus, the feasibility of research tools, recruitment process, and the method of data collection was workable and acceptable for mothers and their late preterm infants.
2.7.2. Intervention Phases
The intervention will be conducted in two phases. In Phase 1, mothers will attend face-to-face training sessions (30-35 minutes) in a private room located in the postnatal unit. In Phase 2 (30-45 minutes), the mothers will demonstrate the learned knowledge of their LPI in a private room under the observation and verbal feedback of the researcher.
Prior to discharge, booklets will be provided to the mothers via their cell phones. This approach ensures that mothers have access to a wealth of knowledge and can dig into specific areas of interest or concern related to the topic discussed in the education session, allowing easy accessibility to the information.
The strategies for teaching mothers are based on Bandura's theory of self-efficacy, concepts of performance modeling, and verbal and emotional claims of mothers’ self-efficacy [19]. Consequently, 1) the completion of training in two phases will allow researchers to understand their performance requirements, demonstration, involvement, and evaluation; 2) training occurs by individualized instruction by modeling and allows observation of the educator; 3) the educator will provide verbal support, feedback, and assurance to help mothers develop a sense of self-efficacy; 4) beliefs that mothers have in their capacity to exert control over the things that happen in their lives and at work might stimulate them to care for their LPIs.
2.8. Research Instruments
Participants received a copy of the data collection tool, including two main parts: 1) a demographic datasheet and 2) three instruments to measure the study variables. Approval to use the instruments was obtained from authors of the various instruments and was then translated into Arabic according to WHO guidelines. The World Health Organization (WHO) Process of Translation and Adaptation of Instruments were used to translate the instruments that are not available in Arabic [20]. Two bilingual experts—a Jordanian English teacher with a Master's degree and a US-based Ph.D. nurse—translated the scales. Changes were made after this suggestion. After being translated by a bilingual US professor, the scales were checked by the expert nurse. The translation was accepted in its final form.
2.8.1. Demographic and Background Data Sheets
First, a demographic and background data sheet was prepared by the researchers, which included: 1) Mothers’ sociodemographic data, including age, marital status, education level, employment, family income, current house living, the current area of residence, and nationality; 2) Mother’s obstetric data, including gravidity and parity, history of complicated pregnancy, mode of delivery, number of antenatal visits, type of antenatal visit, date of mother's admission and discharge; and 3) Infants’ demographic and clinical data, including gestational age at admission and discharge, birth weight at admission and discharge, sex, APGAR score (at one and five minutes after birth), and reason for neonatal admission.
2.8.2. The Perceived Maternal Parenting Self-efficacy (PMP S-E)
The PMP-SE tool (Barnes & Adamson-Macedo, 2004) will be used to measure mothers’ self-efficacy. This tool measures a mother's belief in her ability to provide adequate care for her infant during transition in four areas: 1) caretaking procedures, 2) evoking behavior, 3) reading behavior, and 4) situational beliefs with a total of 20 items [21]. Responses to each item comprise a four-point Likert scale ranging from 1 = disagree to 4 = strongly agree. A higher score indicates a higher level of maternal self-efficacy. Cronbach’s alpha internal consistency coefficient of the whole scale is 0.91; the internal consistency coefficients for subscales are 0.74, 0.89, and 0.72, respectively [22]. In a study conducted with a sample of mothers in Jordan, the Arabic version of the tool showed a Cronbach's alpha of 0.78 [23].
2.8.3. The Maternal Readiness to Hospital Discharge (M-RHD)
The M-RHDS comprises 11 items (short version); the revised RHDS contains five factors consistent with the original scale, which assesses the family's competency during the transition to home, with a score range from 0 = none to 10 = totally, extremely (Higher scores indicate greater readiness for hospital discharge) [24]. The reliability of the RHDS was 0.85 [24]. The Arabic version of the RHDS scale was reliable among postpartum: 22 items in four subscales: 1) personal status, 2) knowledge, 3) coping skills, 4) expected support. Cronbach’s alpha internal consistency coefficient of the whole scale is 0.75 [25].
2.9. The Data Collection Procedure
Data collection will be divided into two phases for each group (intervention and comparison group): mothers of LPIs before their infants’ discharge (pre-intervention period or pre-routine discharge care) and mothers of LPIs discharged home (post-intervention period or post-routine care 1-2 weeks after discharge.
2.9.1. The Comparison Group
First, the researcher will start with the comparison group to prevent the transfer of information between the groups. The steps will be as follows:
1. A contact and rapport relationship will be established with the mothers of LPIs who will be selected according to the study protocol (identifying LPIs from the NICU and then obtaining the name mothers from the postpartum lists). An assistant from the nursing staff will explain the history of the mothers before meeting them face-to-face.
2. A written consent form for each study participant will be signed, with a full explanation of the study's aim, full protection of their confidentiality, and their ability to drop out at any time.
3. Neonatal demographic data will first be collected from the logbook in the NICU, and after the mother's agreement to participate, the socio-demographic and obstetric data will be obtained.
4. The researcher will obtain the preassessment (PMP S-E, and M-RHD) questionnaires from the mothers of LPIs at two different time points. Initial data will be collected through face-to-face interviews in September 2023 in the postnatal units. The researcher will also contact the mothers via telephone after discharge to verify that they have adhered to the prescribed regular care. The second post-assessment questionnaire (PMP S-E and M-RHD) will be obtained 1-2 weeks after discharge via telephone.
5. Routine care primarily focuses on the assessment of maternal and neonatal physiological stability before discharge. Firstly, the mother is discharged if she has an uncomplicated birth that lasts no longer than 24 hours, she enforces exclusive breastfeeding, and mothers and family recognize danger signs for the mother and infant and know when to seek help. The mother is also educated about counseling on postpartum family planning and is offered a contraceptive method of choice.
6. Considering that the hospital adopted the Baby-Friendly hospital initiative in 2022, specialized nurses discuss breastfeeding with mothers, help them start breastfeeding immediately after birth, and provide immediate 15-minute skin-to-skin contact. Moreover, nurses help mothers overcome the challenges of breastfeeding by allowing mothers and infants to stay in the room together 24 hours a day and educate mothers on feeding cues, proper sucking techniques, efficient breastfeeding time, and duration.
7. The infant’s physical exam, breastfeeding, weight status, Vitamin K level, delayed bathing, and meconium passage are part of the routine care before discharge. Neonatal testing (thyroid functioning, metabolic screening, hearing screening, and APGAR test) is applied before discharge. Positive serologic tests for hepatitis are treated as protocol. If the infant has signs of congenital anomalies, the family will be refered to specialty care.
2.9.2. The Intervention Group
Secondly, the researcher starts with the intervention group with the following steps:
1. A contact and rapport relationship will be established with the mothers of LPIs who were selected according to the study protocol (identifying the LPIs from the NICU, and then obtaining the name of mothers from the postpartum list). An assistant from the nursing staff will be obtained with explanation of the history of the mothers before meeting them face-to-face.
2. Mothers who accompanied their LPIs in the postpartum unit will be invited to a specialized room in the postpartum ward, which was established as part of the Baby-Friendly initiative. This gives caregivers the opportunity to enhance the modeling, verbalization, and emotional support of mothers while teaching the discharge education program. The room contains two beds, a smart TV, and a refrigerator and is equipped with standard precautions.
3. A booklet will be used to guide researchers. The intervention of the study is described in detail in the Intervention section. However, the researcher will obtain the preassessment (PMP S-E, and M-RHD) questionnaires from the mothers at two different time points. Initial data will be collected through face-to-face interviews at the beginning of August 2023 in the postnatal units. The researcher will also contact the mothers via telephone after discharge to verify that they have adhered to the prescribed regular care. The second post-assessment questionnaire (PMP S-E, and M-RHD) will be obtained 1-2 weeks after discharge via telephone.
2.10. Pilot Study
The researchers analyzed the study to examine the feasibility of the recruitment process and ensure that the data collection method was workable and acceptable to the mothers. This pilot study was conducted with 10 mothers (five mothers in each group) and the recruiting method was the same as the primary study protocol.
The researcher established a feasible time and place to conduct the study intervention. Feedback from the mothers was positive regarding the intervention content and improvement in their sense of preparation for discharge.
2.11. Ethical Considerations
Ethical considerations will align with the Declaration of Helsinki. Written informed consent will be obtained from the participating mothers, assuring them that no personal information will be disclosed at any time during the study. The participants will be enrolled in the study on a voluntary basis and they will be informed that they can withdraw from the study at any time after signing consent. This study has been approved by the institutional review board (IRB) of the mentioned hospital. Moreover, ethical approval from the University of Jordan/ School of Nursing was obtained.
2.12. Data Analysis
The Statistical Package for Social Science (Version 23) will be used for data analysis, including frequency distribution and percentages, to analyze nominal data such as mothers’ sociodemographic and obstetric data, and infants' information. For continuous variables, such as self-efficacy and mother preparedness scores, the total mean will be calculated - mean, median and standard deviation. To test the study hypotheses, data will be analyzed using inferential statistical methods, including the following:
a). An independent t-test (one-tailed) will be used to compare maternal parenting self-efficacy levels among mothers of LPIs who received and did not receive the neonatal care training intervention before discharge. A paired sample t-test will be used to compare the mean self-efficacy between the pre-test and post-test scores within the experimental and comparison groups.
b). An independent t-test (one-tailed) will be used to compare maternal readiness for hospital discharge among mothers of LPIs who received and did not receive the neonatal care training intervention before discharge. While a paired sample t-test will be used to compare the mean maternal readiness for hospital discharge between the pre-test and post-test scores within the experimental and comparison groups.
c). Multiple linear regression will be used to determine which sociodemographic and obstetric factors explain the variability in parenting self-efficacy levels among mothers of LPIs who receive infant care training intervention before discharge. (The sample size was determined using G Power (Version 3.1.9.4). The calculation will utilize a one-tailed t-test with a fixed model, considering the specified parameters. A power level of 0.80 (1-β), a significance level of 0.05, and a medium effect size of 0.5 will be chosen for convenience, with a total of 12 predictors).
2.13. Verifying and Cleaning Data
Due to the high risk of data entry errors, double-checking and correcting data will be assumed by two researchers. The researcher will enter all data into SPSS version 23 in this study. However, outliers will be valued significantly higher or lower than the average [26]. To identify data outliers, the frequency distribution will be analyzed, with particular attention to the minimum and maximum values [27]. Researchers will frequently encounter missing values in their data sets in SPSS [27]. The researchers will also screen the data in this study to identify and address any missing data to be considered before analysis [27].
3. RESULT AND DISCUSSION
This paper shares an original study protocol to examine the effect of a NICU nurse providing discharge educational programs on the essential home care of LPIs on mothers’ sense of preparedness, represented by their sense of self-efficacy and predischarge readiness to care for their LPIs at home.
The study protocol is a comprehensive scientific document that provides a detailed description of the planned design for future studies [28]. It encompasses the study’s underlying rationale, aims, research questions, and measurement strategies [29]. Publishing in-progress research study protocols is on the rise; there is an increased scholarly awareness of the importance of disseminating methodological insights among academic scientists prior to conducting the study [29-33].
Some researchers find it beneficial to publish a study protocol separately from the full report of the study findings; i.e., the protocol allows for a full description of the technique, which may reduce the need for elaborate explanations in the subsequent study reports publication [31]. Publishing a research protocol encourages research transparency and allows for the exchange of methodological merits among researchers. Editors can ask writers to provide clarity for ambiguous, contradictory explanations and rationales for the research methodology [33]. Sharing study protocols improves the researcher's adherence to study plan implementation while avoiding the duplication of similar protocols [29, 33]. Most importantly, sharing a study protocol facilitates peer-to-peer revision of a study plan before its implementation; therefore, highlighting and refining the quality of research studies early lowers bias or inconvenient findings [33-35].
The evidence and practice addressing mothers who transition from the NICU to home with their LPI needs to be revised based on extensive literature [12, 36-39] showing that NICU discharge readiness and strategies for discharge preparation are important worldwide. Recently, the current teaching program dealing with discharge planning among mothers with LPIs has been deemed inefficient owing to its variability and unintended exclusion [38]. The discharge education program mandates the creation of an educational program of study encompassing vital topics for mothers of LPIs to acquire proficiency before leaving the hospital [38]. In addition, the teaching curriculum is accompanied by the utilization of supplementary resources, diverse instructional methods, rooming in with mothers, and the provision of group-based learning opportunity strategies [38].
The conceptualization of the successful transition of mothers to LPIs will be added to this shared protocol by incorporating specific criteria of the two important components mentioned by Smith et al. (2021): Education-based curriculum and teaching strategies. The education discharge program for the mother of LPIs, according to the literature, needs to fill some specific gaps of health-related challenges among this specific preterm infant age group [38, 40]. There is also a gap between the global perspective and the standard mean of mothers’ smooth transition from their LPI to home [12, 38, 40, 41].
Carvalho et al. (2021) showed that a mother’s paradoxical emotions, home care concerns, and social networks after discharge are critical for the successful transition after discharge. Although Carvalho et al. (2021) acknowledged the importance of specific factors contributing to successful care transition, the most important was the continuity of care after hospital discharge [42]. Comparing that to this study protocol, the protocol is not focused on the continuity of care after hospital discharge and further research is needed to investigate the impact of continuity of care on the overall well-being and outcomes of both mothers and LPIs after discharge.
This study outlines the methodology of a non-randomized experiment aimed at assessing the impact of an intervention on mothers of LPIs, as well as examining the intervention process. Quasi-experiments provide valuable insight into real-world settings and can help establish causal relationships between variables in situations where true experiments are not applicable [43]. Quasi-experiments are considered a subset of experiments that aim to enhance the rigor of true experiments without random assignment [44].
Thus, researchers utilize nonequivalent comparison groups to reduce non-randomization effects [45, 46]. Specifically, the researchers in this study will focus on experimental manipulation (education program) differences in terms of minimizing the potential confounding variables and increasing the validity of the findings [46]. Therefore, to accomplish the results of the educational program merely among the outcome variables, the researchers created well-defined eligibility specifications for both groups (comparison and experimental) [46, 47]. Additionally, the researcher will employ a statistical approach to further enhance the comparability between the two groups using a regression analysis statistical test [12, 38].
However, researchers should consider several factors when choosing an experimental design to optimize the internal and external validity. The researchers chose a pre-post design for the two groups. The primary objective of the pretest was to establish the comparability of the two groups before the implementation of the treatment [43].
Conversely, the post-test enables researchers to assess the immediate impact of the intervention on the outcome variables [43]. The inclusion of many pre- and post-test designs plays a crucial role in enhancing the internal validity of research outcomes [43, 48].
Additionally, the study protocol discusses the design, measurement, and statistical difficulties of quasi-experiments, focusing on internal validity issues, inclusion/exclusion criteria, and treatment [46]. Thus, researchers can ensure a comprehensive analysis of outcomes and provide valuable insights into the implementation of educational programs.
CONCLUSION
Implementing a comprehensive and holistic educational program is a novel strategy characterized by its diverse nature and scientific underpinnings. These integrated programs have the potential to serve as models for nationwide evidence-based initiatives in the field of infant care. The potential impact of this methodology may have broader implications beyond the well-being results for both mothers and LPIs as perceived by researchers.
The study findings will provide insight into national nursing practices through a thorough discharge education program for mothers of LPIs. The educational program presented in this study will enhance healthcare professionals’ efforts by providing standardized, evidence-based educational resources for mothers to manage LPI home care. Moreover, the information and training that are presented in this program, if well supplied by nurses to mothers, will contribute to the overall improvement of LPI healthcare outcomes and reduce the risk of complications after discharge. Ultimately, this study contributes to the advancement of LPI healthcare globally by disseminating effective and research-examined care considerations for transitioning LPIs to home.
Additionally, a comprehensive educational program may serve to empower mothers and enhance their ability to create a nurturing environment for their LPI in the long run after discharge. Thus, this protocol may inspire standard educational programs and strategies to provide care for mothers and LPIs in healthcare settings.
LIST OF ABBREVIATIONS
| HCAC | = Health Care Accreditation Council |
| PMP S-E | = Perceived Maternal Parenting Self-efficacy |
| LPIs | = Late Preterm Infants |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study setting was provided by AL Hussein Medical Center at RMS -Amman, and the University of Jordan and School of Nursing provided the ethical approval.

