All published articles of this journal are available on ScienceDirect.

Internal Structure of the Brazilian Online Version of the Childbirth Fear Prior to Pregnancy Scale
Authors Info & Affiliations
Abstract
Background
Approximately 80% of pregnant women have some degree of childbirth fear, which can have short- and long-term negative effects when not correctly identified and managed. Therefore, it is essential to assess childbirth fear to measure and identify factors related to this fear. Furthermore, it is crucial to develop appropriate and early interventions to improve the childbirth experience for women and their families, including the obstetric care provided.
Objective
This study aimed to assess the validity of the internal structure of the Brazilian online version of the Childbirth Fear Prior to Pregnancy (CFPP) scale.
Methods
This methodological study was conducted to assess the validity of the internal structure of the Brazilian online version of the CFPP scale. A total of 553 men and women aged 18 or older participated in the study. The participants were not pregnant at the time of data collection but intended to have children in the future. A combination of Exploratory and Confirmatory Factor Analyses were used for statistical analysis. Reliability was assessed using Cronbach’s Alpha and McDonald’s Omega indicators. The Research Ethics Committee approved the study (protocol no: 4.961.821.)
Results
The psychometric parameters indicated a unidimensional model with adequate factor loadings (0.47–0.73) and reliability (0.86). Goodness of fit was achieved (χ2/df = 1.5, NNFI = 0.97, CFI = 0.98, GFI = 0.98, and SRMR = 0.06).
Conclusion
The Brazilian online version of the CFPP scale showed evidence of internal structural validity and reliability for measuring the construct in the population of this country.
1. INTRODUCTION
Childbirth is a physiological and dynamic process permeated with several sensations and feelings experienced individually by women and their families [1-3]. Although it is a moment that is often expected and desired, around 80% of pregnant women have some degree of childbirth fear, with approximately 14% experiencing severe or phobic fear [4-6]. Childbirth fear is a psychological phenomenon, a physical and emotional state of intense anxiety that affects the health and well-being of a woman, with negative short- and long-term consequences for herself—further affecting her relationships with her partner, family, and baby [2, 6-8].
The causes of this situation include fear of the unknown, the possibility of complications for the mother and baby, the use of interventions, and concerns about dealing with pain [1, 3, 4, 9]. Not identifying and managing this feeling can result in prolonged labour, lower pain tolerance, higher intervention rates (e.g., increased use of analgesia and elective caesarean sections), a higher frequency of lousy birth experiences, postpartum depression, and difficulty bonding with the baby [3, 4, 6, 7, 9].
This understanding calls for the development of appropriate and early interventions to improve the birth experience not only for women but also for their families, encompassing the obstetric care provided. For this cause, some instruments to measure childbirth fear have been proposed and validated in other countries; most of them are administered during the gestational period and only to women [10-14]. The most widely used is the Wijama Delivery Expectancy/Experience Questionnaire (W-DEQ) [5, 6, 8, 15], developed in Sweden in 1998, whose main objective is to measure childbirth fear in pregnant, nulliparous, and multiparous women during and after pregnancy, corresponding to versions A and B, respectively [10].
The experience of pregnancy can have a significant impact on the life of a woman. Additionally, it is important to recognize that men can also experience anxiety about childbirth [16, 17]. Considering that everyone involved in this process is affected, the Childbirth Fear Prior to Pregnancy (CFPP) scale can measure childbirth fear in men and women before pregnancy without age limitation. It is the only instrument adapted and validated in Brazil for this purpose and is also validated in Germany, Australia, Canada, the United States, England, Iceland, and Portugal [17-19]. The original scale comprised six items and assessed childbirth fear among Canadian university students in 2013. Currently, it has 10 items [20].
In the cross-cultural adaptation process in Brazil, the CFPP was administered in printed form and showed favourable psychometric properties [19]. However, an online version of this scale has become relevant due to the increasing use of the internet and social networks as a form of communication and interaction between individuals. This implies that these technologies are increasingly being incorporated into teaching and learning in several areas of knowledge, mainly because they enable greater access to data collection in research [21, 22].
Changing the instrument format from print to online results in visual changes from a horizontal to a vertical model, adapted for visualisation in several technological devices. These modifications can influence the response behaviour of those being assessed. This is because individuals tend to respond more extremely to surveys when the items are presented compactly. For instance, the responses are related to the effects of the visual distance between response categories, affecting essential parameters for evaluating the scale, including its internal structure [23, 24].
Furthermore, according to the Standards for Educational and Psychological Testing of the American Educational Research Association, the American Psychological Association, and the National Council on Measurement in Education, internal structure analysis can indicate the degree to which the relationship between items and components of the test conform to the construct proposed for score interpretations [25]. Therefore, this study aimed to assess the internal structure of the Brazilian online version of the CFPP scale.
2. METHODS
2.1. Type of Study
This was a methodological study focused on assessing the validity of the internal structure of the CFPP scale. This type of study aims to obtain, organize and analyse data to obtain valid and reliable instruments. The scale showed good psychometric properties in the validation study with the face-to-face application, and the aim was to evaluate the scale for application in the online modality [26].
2.2. Population and Sample
The inclusion criteria for research participants covered men and women aged 18 or over, who were not currently experiencing pregnancy at the time of data collection and expressed an intention to have children in the future. Participants under 18 years of age were excluded, as were questionnaires that did not provide answers to all questions. Furthermore, participants who indicated that they did not wish to have children and responded negatively to the initial question about this intention had their participation in the research automatically terminated.
Two instruments were used for data collection. The first consisted of an online form covering sociodemographic data, socioeconomic, behavioral identification, health and obstetric information. The second instrument was the Fear of Childbirth Scale (CFPP), which was translated, adapted, and validated in the Brazilian context, totalling a sample of 553 participants.
2.3. Data Collection and Instrument
The data were collected through online research between January and April 2022. The questionnaire was publicised through virtual media, such as e-mails, social networks (Facebook and Instagram), and personal contacts (WhatsApp), spreading through a multiplier propagation effect. The invitation sent to the participants included the objective of the study and a link to the Google Forms platform. Specifically, when clicked, it gave the participant access to the Informed Consent Form (ICF), the electronic instrument for collecting socioeconomic, obstetric, and behavioural data, and to the CFPP scale. Online media was used to remotely collect primary data via the Internet when social distancing was required. The advantages of this method include low cost, easy implementation, fast planning, result publishing, and the immediate inclusion of individuals from different geographical regions [27].
The Childbirth Fear Prior to Pregnancy (CFPP) scale was developed in 2016 by Kathrin Stoll as an instrument to investigate the presence of fear of natural birth among young adult men and women who are not pregnant. The dimensions addressed by the scale include fear of pain during childbirth, fear of loss of control and inability to deal with labor, as well as fear of birth complications and bodily harm. The instrument is characterized by its accessible language and quick application [17]. This tool aims to provide a comprehensive understanding of the fear of childbirth before pregnancy, contributing to the assessment and understanding of this psychological dimension in non-pregnant young adults.
During the process of cross-cultural adaptation of the CFPP to the Brazilian version, the instrument proved to be useful, presenting good evidence of validity and reliability for measuring fear of natural birth in the population of young adults before pregnancy. This adaptation work was conducted by Tomazin et al. in 2021, highlighting the commitment to making the scale applicable and accurate for the Brazilian reality. By adapting the CFPP to the Brazilian context, the study conducted by Tomazin and colleagues contributed to ensuring the cultural relevance and effectiveness of the scale when assessing the fear of childbirth before pregnancy in young adults in Brazil [19].
The Brazilian version of the CFPP is composed of a short and simple measure, being unidimensional and composed of 10 items. Each item corresponds to a statement about the fear of childbirth. The scale uses the Likert format, in which participants indicate their level of agreement on a five-point scale: (1) completely disagree, (2) disagree, (3) partially disagree, (4) agree and (5) completely agree. This approach aims to provide a comprehensive assessment of the fear of childbirth before pregnancy [19].
The Checklist for Reporting Results of Internet E-Surveys (CHERRIES) proposed by Eysenbach was used to build the tool in a virtual or web environment, assuring the quality of the reports [28]. The questionnaire was distributed on pages, and participants could check, revise, and change their answers using the back button. Mandatory questions were identified by an asterisk (*) [28].
The validation questionnaire was previously tested for comprehensibility, easy response, programming aspects, and database generated. After pre-testing, the questionnaire was corrected online (Google Forms), and the participants were recruited.
2.4. Data Analysis
A combination of Exploratory Factor Analysis (EFA) and Confirmatory Factor Analysis (CFA) was used for statistical analysis. The Kaiser-Meyer-Olkin (KMO) ≥ 0.70 and Bartlett’s Test of Sphericity (BTS) were considered to indicate sample adequacy in this study [26]. EFA used parallel analysis based on a polychoric matrix [26, 29]. Factor extraction was carried out using the Robust Unweighted Least Squares(RULS) technique [30], with Promin rotation and minimum factor loadings and communalities ≥ 0.40. The Bootstrapping technique was used to test robustness, with sample extrapolation to 5,000 [31].
CFA included chi-square ratio by degrees of freedom (χ2/df<5), Non-Normed Fit Index (NNFI) >0.95, Comparative Fit Index (CFI) >0.95, Goodness of Fit Index (GFI) >0.95, Adjusted Goodness of Fit Index (AGFI) >0.95, and Root Mean Square of Residuals (RMSR) <0.08 as indices for assessing the goodness of fit of the model [[32]. Reliability was assessed using Cronbach’s Alpha [33] and McDonald’s Omega [34], and all the data obtained were analysed using Factor 12.02.01 and JASP 0.16.4 statistical software.
3. RESULTS
The Brazilian online version of the CFPP had a mean response time of 5 min. A total of 648 individuals answered it. Of these, 95 had to be excluded, resulting in 553 participants, primarily women (451, 81.5%), white (358, 64.7%), with a mean age of 27.2 years (standard deviation 11.3), living in the Southeast region (347, 63.2%). Moreover, they had a high level of education, predominantly with 13 years or more of study (396, 71.7%). A large proportion of the sample reported having a partner (331, 59.9%), and half of the participants were health professionals (270, 49.7%), some of them directly working in childbirth care (24, 4.4%) (Table 1).
As for obstetric characteristics, few participants had children (92, 16.7%), most undergoing caesarean sections in the last pregnancy (65, 11.7%), with no negative pregnancy experiences (61, 11.1%). Additionally, many participants sought information about childbirth during pregnancy, with a considerable proportion seeing health professionals (145, 35.3%) (Table 2).
| Variables | n | % |
|---|---|---|
| Sex | 553 | - |
| Women | 451 | 81.5 |
| Men | 100 | 18.1 |
| Not identified | 2 | 0.4 |
| Skin colour | 553 | - |
| White | 358 | 64.7 |
| Not white | 195 | 35.3 |
| Education - years of study | 553 | - |
| Up to 9 | 8 | 1.4 |
| 10–12 | 149 | 26.9 |
| 13 years or older | 396 | 71.7 |
| Marital status | 553 | - |
| No partner | 222 | 40.1 |
| With partner | 331 | 59.9 |
| State of residence | 549 | - |
| North | 24 | 4.4 |
| Northeast | 59 | 10.8 |
| South | 32 | 5.8 |
| Southeast | 347 | 63.2 |
| Centre-west | 87 | 15.8 |
| Health professional | 544 | - |
| No | 274 | 50.3 |
| Yes | 270 | 49.7 |
| Works in childbirth care | 545 | - |
| No | 521 | 95.6 |
| Yes | 24 | 4.4 |
| Variable | n | % |
|---|---|---|
| With children | 553 | - |
| No | 461 | 83.3 |
| Yes | 92 | 16.7 |
| Type of childbirth in last pregnancy | 552 | - |
| Normal | 27 | 4.9 |
| Caesarean section | 65 | 11.7 |
| Not applicable | 460 | 83.4 |
| Negative experience in last pregnancy | 551 | - |
| No | 61 | 11.1 |
| Yes | 31 | 5.6 |
| Not applicable | 459 | 83.3 |
| Source of information | 411 | - |
| Scientific articles | 77 | 18.7 |
| Printed material | 5 | 1.2 |
| Relatives/friends | 57 | 13.9 |
| Health professionals | 145 | 35.3 |
| Videos/Internet | 127 | 30.9 |
As for psychometric analyses, the online Brazilian version of the CFPP showed good sample adequacy, verified by the BTS (2,614.7, df = 45, p < 0.001) and the KMO test (0.81, CI95% = 0.767–0.839). The unidimensional characteristic of the instrument was confirmed by parallel analysis, with an eigenvalue of 4.04. Due to unidimensional means, the rotational techniques were not necessary for the factor matrix.
Factor loadings ranged from 0.47 to 0.73, indicating satisfactory and adequate correlation levels between variables. No collinearity or multicollinearity problems or Heywood cases were found. Communalities ranged from 0.22 to 0.53, with six items showing values above 0.40. The explained variance was 51.9%, showing the low explanatory power of the model. Table 3 shows factor loadings and communalities for each item on the scale (Table 3).
Table 3.
| Item | F1 | Communalities |
|---|---|---|
| 1 | 0.67 | 0.45 |
| 2 | 0.67 | 0.45 |
| 3 | 0.71 | 0.51 |
| 4 | 0.72 | 0.52 |
| 5 | 0.54 | 0.30 |
| 6 | 0.73 | 0.53 |
| 7 | 0.68 | 0.47 |
| 8 | 0.49 | 0.24 |
| 9 | 0.56 | 0.32 |
| 10 | 0.47 | 0.22 |
| Classification | Score | N | % |
|---|---|---|---|
| No childbirth fear | 10 ≤ x ≤ 28 | 153 | 27.6 |
| Mild childbirth fear | 29 ≤ x ≤ 33 | 143 | 25.8 |
| Moderate childbirth fear | 34 ≤ x ≤ 37 | 111 | 20.0 |
| Severe childbirth fear | 38 ≤ x ≤ 50 | 146 | 26.4 |
| Total | - | 553 | 100 |
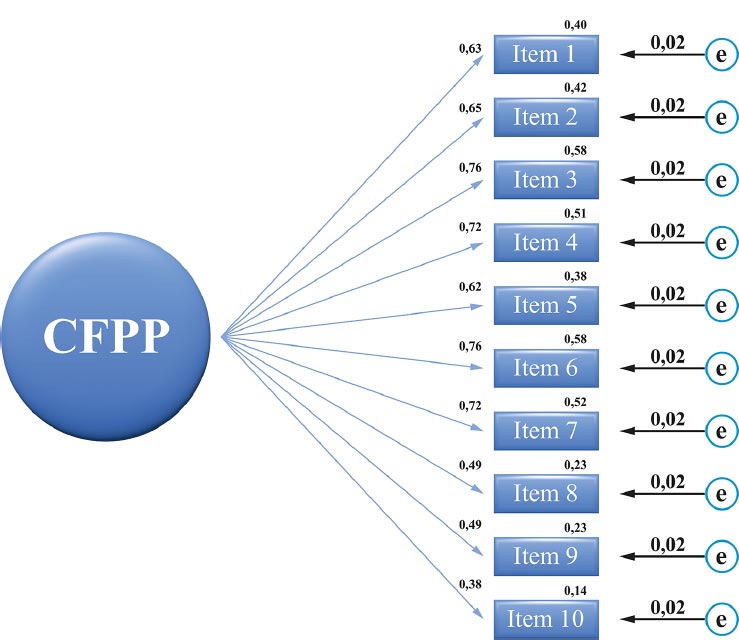
The CFA indices showed that the model fitted the following values: χ2/df=1.5, NNFI=0.97, CFI=0.98, GFI=0.98, and SRMR= 0.06. Fig. (1) shows a path diagram summarising the analysis. Factor loadings and predictive values were satisfactory (Fig. 1).
Cronbach’s Alpha and McDonald’s Omega reliability was 0.86. The score was obtained from the sum of the 10 items of the instrument, ranging from 10 to 50, the highest scores indicating greater fear of childbirth. The proposed scores revealed that 111 (20.0%) participants had a moderate fear of childbirth, 143 (25.8%) had a mild fear of childbirth, 153 (27.6%) had no fear of childbirth, and 146 (26.4%) % had a severe fear of childbirth. The CFPP results showed that 400 (72.3%) participants reported some degree of fear of childbirth (Table 4).
When evaluating each item, most participants agreed with items 1, 5 and 7, revealing that they worried that pain during childbirth might be very strong (n=471, 85.1%), something bad might happen to the baby (n=382, 69%) and were afraid of complications during labor and birth (n=422, 73.3%), respectively. Of the respondents, 274 (n=49.5%) disagreed with item 10 about the fear that the body would never be the same after delivery.
4. DISCUSSION
The objective of this study was to assess the psychometric properties of the Brazilian version of the CFPP scale using an online application to validate its internal structure, considering that changing the administration format from print to online caused visual changes that could influence the response behaviour of the participants, consequently affecting important assessing parameters, such as its internal consistency [23, 24].
The SQUIRE 2.0 tool contributed to the selection, ordering, and presentation of the most relevant information produced by this study. Based on the data collected and the statistical analyses used, the developed instrument showed evidence of internal structure validity and adequate reliability to assess childbirth fear in men and women before pregnancy. However, the instrument may not be suitable for the trans population. Therefore, it needs to be tested in this group, or another scale should be proposed, bearing in mind that this population also experiences childbirth fear and several other difficulties during the pregnancy-puerperium period, such as the risk of transphobic violence in healthcare [35].
EFA validation of its internal structure represents the degree to which the correlation between the items typically reflects the construct measured by the test. For instance, it informs the measurement precision of the instrument, ensuring that what was measured in a sample reflects the data of a given population [26, 36].
The study showed good sample adequacy indicators, continuing with the factor analysis. Thus, the factor loadings indicated satisfactory and adequate levels of correlation between variables, corroborating the results from other countries where the CFPP was validated [17-19]. In Australia, factor loadings ranged from 0.51 to 0.71, in Canada from 0.54 to 0.72, in Germany from 0.56 to 0.77, in Iceland from 0.53 to 0.77, in the UK from 0.52 to 0.81 and in the US from 0.51 to 0.71 [17]. In addition, in Portugal, it ranged from 0,49 to 0,91 [18], and in Brazil, the factor loadings of the printed version ranged from 0.5 to 0.7 [19].
The unidimensional characteristic of the instrument was confirmed by parallel analysis, which was also ratified in the Brazilian printed version, which showed a moderate correlation between items and a strong correlation between all items and the total [19]. Although in other countries, the validated scale presented the possibility of obtaining three domains in the analysis, which was maintained in the Portuguese version [18], Kathrin Stoll et al. suggested maintaining only one since domains with fewer than three items are not recommended, conceptualising the CFPP scale as unidimensional by inter-item and item-total correlation analyses [17].
Communalities are the variance (correlation) of each variable explained by the factors. Thus, the higher the communality, the greater the power of the factor to explain that variable. Some items showed a communality below the cut-off point in this study. Nonetheless, factor loadings were adequate, and the other tests attested to the quality of the model, which supports keeping these items in the instrument.
The explained variance was obtained from the communalities, and the results showed low shared variance in some items. The presented variance is higher than the value obtained for the printed Brazilian version of the CFPP [19]. Nevertheless, further studies are needed to identify new childbirth fear aspects to broaden measurements to achieve a value higher than 60% [26]. CFA showed adequate adjustments to the model.
The Cronbach’s Alpha and McDonald’s Omega values indicated good reliability [37]. Two indicators were used to increase the reliability of the interpretation due to the reliability of inconsistencies with Cronbach’s Alpha [38]. Similar reliability values were obtained in other countries using the same Alpha coefficient [17-19].
The score obtained with the Brazilian online version of the CFPP showed that many men and women intending to have children in the future had childbirth fears ranging from mild to severe. The mean score (32.5) was slightly lower than CFPP scores in Australia, Canada, Iceland, and with the printed Brazilian version (36.6, 34.3, 35.1, and 35.4, respectively). The highest scores were in England (38.5) and the United States (37), and the lowest in Germany (29.8) [17, 19].
More than 40% of participants had moderate to high fear of childbirth, which could affect the type of delivery choices [1, 3, 7, 39, 40]. Several factors have been associated with the development of childbirth fear, in addition to concerns inherent in the dynamic nature of the process. These include previous individual or familial negative experiences, information dissemination, and psychological and sociodemographic factors [39].
Some studies show that certain interventions can help reduce childbirth fear, in particular, including cognitive-behavioural therapies, psychotherapies, prenatal education, hypnobirthing, relaxation, pilates, art therapy, interventions during labour (acupressure and music therapy), and improved and continuous obstetric care [39, 41]. However, more clinical studies with adequate methodological rigour are needed to confirm the effectiveness of these interventions in reducing childbirth fear. Furthermore, instruments for measuring these phenomena complement the professional healthcare provided, highlighting other aspects of the process. Nonetheless, healthcare should be integral, including active listening and welcoming individual needs.
CONCLUSION
The Brazilian online version of the CFPP scale showed evidence of internal structure validity and adequate reliability to measure childbirth fear in men and women before pregnancy. Furthermore, the online format reaches more individuals to identify and target modifiable factors related to childbirth fear. Furthermore, the early detection of this fear and associated factors can help plan and develop health education strategies to improve the quality of obstetric care.
LIST OF ABBREVIATIONS
| CFA | = Confirmatory Factor Analysis |
| EFA | = Exploratory Factor Analysis |
| AGFI | = Adjusted Goodness of Fit Index |
| CFI | = Comparative Fit Index |
| CFPP | = Childbirth Fear Prior to Pregnancy |
| df | = Degree of Freedom |
| GFI | = Goodness of Fit Index |
| KMO | = Kaiser-Meyer-Olkin |
| NNFI | = Non-Normed Fit Index |
| RMSR | = Root Mean Square of Residuals |
| RULS | = Robust Unweighted Least Squares |
| ICF | = Informed Consent Form |
| BTS | = Bartlett’s Test of Sphericity |
| W-DEQ | = Wijama Delivery Expectancy/Experience Questionnaire |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The Research Ethics Committee of the Hospital das Clínicas of the Botucatu Medical School approved this study (protocol no: 4.961.821).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT TO PUBLICATION
All participants signed an informed consent form (ICF).
STANDARDS OF REPORTING
CHERRIES guidelines were followed for the study.
AVAILABILITY OF DATA AND MATERIALS
The data of current study are available from author, [M.T.J] on a reasonable request.
FUNDING
This study was funded by the Coordination for the Improvement of Higher Education Personnel(CAPES) and the Federal Nursing Council (COFEN) - Notice No. 8/2021.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

