All published articles of this journal are available on ScienceDirect.

The Effectiveness of eHealth Interventions-based Self-care on Health-related Quality of Life for Patients with Heart Failure
Authors Info & Affiliations
Abstract
Background
Heart failure (HF) affects health-related quality of life (HRQoL) and is a public health concern. For people with heart failure, effective self-care practices are crucial.
Aim of the Work
to assess how EHealth interventions-based self-care affect heart failure patients' health-related quality of life.
Methods
Research design: To achieve the study's goal, a quasi-experimental approach was employed.
Setting
The Al-Quwayiyah General Hospital's outpatient clinic in Al-Quwayiyah City, Riyadh, the Kingdom of Saudi Arabia (KSA), was the source of heart failure.
Subjects
60 cases with Heart failure were recruited.
Tools
Tools of gathering data: Researchers created and employed four instruments: 1) Clinical data sheet and patient evaluation; 2) Knowledge assessment sheet; 3) Personality-Maintenance of Heart Failure Index (SCHFI); and 4) Minnesota Living with Heart Failure Questionnaire (MLHFQ).
Results
The patients under study ranged in age from 35 to 65, with 63.3% of them being female. After receiving eHealth Interventions-Based Self-Care, there were statistically significant changes in knowledge, self-care, and health-related quality of life between the pre-and post-tests (P<0.05*).
Conclusion
The study's patient population's degree of knowledge, self-care, and health-related quality of life had all considerably improved thanks to EHealth interventions-based self-care.
Recommendation
Through the implementation of patient-centered care programs, nurses play a proactive role in increasing the understanding of patients with HF regarding self-care and health-related quality of life.
1. INTRODUCTION
A common symptom of cardiovascular disorders is heart failure (HF) [1], which has a significant impact on patients, families, and healthcare systems globally. It lowers the quality of life (QoL) associated with health for HF patients while raising the cost of morbidity, mortality, and healthcare [2, 3].
An estimated 5.8 million Americans have heart failure (HF). Every year, about 550000 new cases are diagnosed. By 2040, 1.5 million additional cases are expected to be reported annually [4, 5]. The valued incidence of HF in Saudi Arabia is 32,200 cases per year, with an extrapolated prevalence of 455,222 patients [6].
Exercise training and CHF disease-related self-care counseling are both recommended by the American Heart Association (AHA) and the American College of Cardiology (ACC) as beneficial [7]. Effective self-care is essential to keeping physiological stability and refining health outcomes in patients with CHF. Several studies have demonstrated the benefits of CHF self-care counseling [8].
For best CHF self-care, a patient must be well-informed, actively engaged in preserving their health, and stick to prescribed treatment regimens, which may include medication and behavioral counseling [9]. Self-care activities are commonly taught to patients with HF as part of their everyday management of the condition. Self-care can refer to a wide range of terms that are used interchangeably to describe the actions or behaviors that patients are urged to participate in order to maintain their health and well-being, such as self-management, self-regulation, self-monitoring, adherence, and compliance [10, 11].
New developments in eHealth technology present excellent chances to support numerous facets of HF self-care. It is crucial to take into account patient use and interest in utilizing eHealth for self-monitoring and HF symptom control [12].
One aspect of eHealth is telemedicine, and one of the most cutting-edge methods in telecardiology in terms of viability and clinical proof is the use of telemedicine in HF patients [13]. The application of information and announcement technologies to health-related issues is referred to as “E-health” [14].
Politicians and healthcare professionals frequently view eHealth as a critical “enabling” technology to improve care and the experience of care for individuals living with chronic conditions, especially during a period of limited healthcare funding. EHealth has the potential to offer creative solutions to health issues [8].
The use of evidence and statement technologies (ICTs) to promote health and health-related activities is referred to as e-health. According to the eHealth action plan for 2012–2020 by the European Union TEMP, there is still a lot of unmet potential for ICT to boost productivity, enhance quality of life, and spur innovation in the health sectors [8]. It is simple to locate technologies that can accurately assess a physiological characteristic or capture a patient's account of symptoms or quality of life, then transmit this information back to the medical personnel [15].
It is thought that the methodical evaluation of HRQOL will improve the promotion of patient-centered treatment. It prioritizes the viewpoint of the patient and can point out areas that require particular attention. This promotes collaborative conclusion-making and guarantees that the patient's choices are taken into account when making management decisions [16].
A crucial outcome indicator for patients with heart disease is their quality of life (QOL), which is a measure of their public, psychological, and physical functioning [17]. People with heart failure need to practice good self-care in order to get the best outcomes and eminence in life [9]. Improved self-care and education among patients with heart failure can be facilitated by nurses [18].
By conducting thorough patient assessments, developing patient-centered goals, evaluating results, supporting EHealth telemonitoring interventions as health promotion, and providing self-care education, nurses can significantly contribute to the improvement of self-care. Furthermore, conventional medical care should continue to employ effective methods while also incorporating self-care for patients with HF guidance [19].
By offering health care interventions based on self-care for HF patients, our study aims to regulate the impact of EHealth interventions-based self-care on health-related quality of life for patients with heart failure. The influence on quality of life is measured as an outcome evaluation. Thus, the objective of the current study was to determine the needs of the patients, plan and carry out EHealth interventions-based self-care for heart failure patients, and assess the impact of these interventions on the patients' health-related value of life. The research hypothesis was that these interventions would have a positive impact on the patient's health-related quality of life.
2. SUBJECTS AND METHODS
2.2. Setting
The study was conducted in the Al-Quwayiyah General Hospital's outpatient clinic in Al-Quwayiyah City, Riyadh, Saudi Arabia.
2.3. Subjects
After agreeing to participate in the trial, convenient samples of sixty heart failure patients were gathered. The researchers recruited the patients by enrolling them according to the inclusion and exclusion criteria. Patients who met the following requirements were included in the study: they had to be at least eighteen years old, female or male, diagnosed with HF and possibly other conditions, stable, unable to undergo myocardial revascularization surgery within the previous thirty days, and able to use social media and be reached by smartphone. Patients with learning difficulties, those getting psychiatric treatment, those under a care order or receiving other social service intervention, and those who did not employ eHealth treatments for self-care were omitted from the study.
2.4. Sample Size
The following statistical formula was used to select the sixty patients with heart failure. Z1-1/2 = is the standard regular variate; at 5% type 1 error (P<0.05), it is 1.96. p = Expected proportion in the population based on prior research. n = Z1-∞/22 P (1-P) /d2. d = Absolute precision or inaccuracy (5%).
3. TOOLS
Data relevant to this investigation were gathered using four distinct instruments (online questionnaire). Among them were the following:
3.1. Patient's Assessment and Clinical Data Sheet: It Contains Two Parts
Part 1: The goal of the data collection was to give descriptive information about the age, sex, marital status, and educational attainment of the patients who were the subjects of the study.
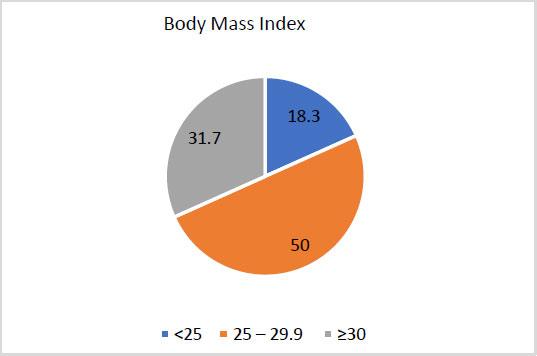
Part 2: The researchers created the form to collect data on smoking behaviors, family history, disease history, and body mass index (BMI).
3.1.1. Scoring System
The body mass index was calculated [20], by dividing the square of the height in meters by the weight in kilos. Underweight: <18.5, Standard weight: <18.5-<24.9, Pre-obesity: 25.0–29.9, Obesity class I: 30.0–34.9, Obesity class II: 35.0–39.9, and Obesity class III: Above 40 were the categories into which the total was divided.
3.2. Patient's Knowledge Assessment Sheet
The researchers created it after reading relevant literature to gauge patients' level of understanding about the definition, risk factors, clinical manifestations, diagnostic procedures, anatomy and physiology of the heart, and strategic plan of heart failure management before and after eHealth interventions-based self-care implementation [21-23]. Cronbach's alpha was charity to assess the tool's dependability (r=0.86).
3.3. Self-care of Heart Failure Index (SCHFI)
Self-care conduct was measured using the Brazilian variety of the Self-Care of Heart Failure Index (SCHFI). The SCHFI is a self-care measure that consists of 23 questions divided into 3 scales: confidence in self-care (6 items), self-care management (6 items) linked to patients' behavior when symptoms arise and self-care maintenance (11 items) regarding behaviors to maintain physiological stability [24]. To ensure correctness, it was translated into Arabic and then back into English. It was used twice, both before and during the implementation of self-care based on eHealth treatments. Cronbach's alpha was second hand to assess the whole tool's dependability (r=0.85).
3.4. Minnesota Living with Heart Failure Questionnaire (MLHFQ)
The MLHFQ is a self-administered, disease-specific tool for patients with heart failure. The 21 questions on the questionnaire focus on various ways that heart failure might negatively impact a patient's life on a physical level (2-7,12,13), emotional level (17-21), and socioeconomic level (1,8-11,14-16). Whether a heart failure treatment improves patients' quality of life by lessening the negative effects of heart failure can be ascertained using this patient-reported outcome evaluation method [25]. To ensure correctness, it was translated into Arabic and then back into English. Cronbach's alpha was used to assess the whole tool's dependability (r=0.88).
3.4.1. Scoring System
The total score can vary from 0 to 105, with higher scores denoting a more serious deterioration in health-related quality of life. Every question is rated on a 6-point Likert scale (0 to 5). The MLHFQ has two domains: the emotional domain (five items, 0 to 25 points) and the physical domain (eight items, 0 to 40 points).
3.5. Validity and Reliability of the Tool
A panel of seven specialists in medical-surgical nursing received the data-collecting instruments and assessed them for validity in terms of “content coverage, clarity, phrases, length, format, and general appearance.” The internal consistency of the instrument was assessed using reliability analysis. With multipoint questions, Cronbach's alpha coefficients were computed to assess measurement reliability. Nothing was changed.
3.6. Pilot Study
Approximately 10% of the study's total sample was used in the pilot trial. It was carried out to assess the content validity, relevance, and clarity of the instruments used to collect data; to gauge how long it took patients to complete the study's instruments; and to identify any potential roadblocks or issues that might arise and prevent the researchers from gathering data. Since the instruments were not changed, the patients who participated in the pilot trial were also included in the main study sample.
3.7. Procedure
After obtaining formal authorization, the researchers began gathering data from the patients who satisfied the requirements for inclusion. In order to get the participants' cooperation and oral consent to be included in the research, the study's methodology was presented to them. The researchers spent three days a week from 9:00 a.m. to 12:00 p.m. at the outpatient clinic. The study was carried out through implementation, evaluation, and recruiting and interviewing.
3.8. Recruitment and Interviewing
Patient recruitment began in October 2022 and was finished by March 2023. The purpose of the study and its methodology were explained to each patient during the roughly 30-minute interview. Every patient that was recruited was split up into five groups, each consisting of 10 to 15 people on average. The name (self-care) and a mobile WhatsApp application were used to create each group. It was stated that the purpose of this WhatsApp app was to facilitate patient contact and provide patients with appropriate health information regarding self-care.
3.9. Implementation
Zoom was used for the online sessions that all of the study patients had. The researchers had reviewed extensive literature and evidence-based research before developing the sessions' content, which focused on self-care. Researchers questioned patients in each online session about whether they had modified the prior instructions. The patient was once more asked to ask questions prior to the online sessions coming to a close. The remaining portion of the session focused on providing information concerning heart failure. There was one online session per week. Each group had an average of four online meetings per month, lasting between thirty and forty-five minutes each. The sessions included group discussions, a PowerPoint presentation, and fliers that were sent via smartphone support services.
3.10. An Evaluation
underlined the importance of measuring, both before and after (after three months), the impact of eHealth interventions-based self-care on patients' knowledge and health-related quality of life.
3.11. Ethical Consideration
Prior to the study, the Shaqra University Research Ethics Standing Committee (ERC_SU_20220080) and other pertinent organizations granted permission to carry out the investigation. Furthermore, permission was acquired by asking study participants to check a “Yes, I agree to participate” box on the questionnaire to indicate that they agreed to participate. They received guarantees of confidentiality and anonymity, as well as the freedom to leave the study at any moment. It was further revealed that the results of the study were to be published in an approved publication and distributed through conference presentations. To preserve participant confidentiality, codes were used instead of names. Questions from the participants were welcome.
3.12. Data Analysis
After the aforementioned technologies finished collecting the data, the data were computed and examined. Version 26 of the Statistical Package for Social Sciences (SPSS) was used to analyze the data. After calculating the frequency distribution, percentages, mean, and standard deviation, the inception of statistical significance which was set at p < 0.05 was described using the Paired Sample T-test and Chi-square test. It will be categorized, totaled, and examined by an appropriate statistical significance test.
4. RESULTS
Table 1 demonstrates that the patients under study ranged in age from 35 to 65, with over one-third (36.7%) being over 60. In terms of gender, women make up fewer than two-thirds (63.3%). Furthermore, just 70% of them—less than three-quarters—were married. Of them, two-thirds (66.7%) were unemployed. Not only that, but less than thirty of them (31.7%) were village residents and sixty-five percent held a bachelor's degree. Furthermore, they do not smoke currently, and their respective negative smoking rates are 63.3% and 81.7%.
According to Body Mass Index (BMI) statistics, Fig. (1) shows that half of the study's patients fell between the range of 25.5 and 29.9, and fewer than one-third (31.7%) of them were over 30.
| Items | No = 60 | % | |
|---|---|---|---|
| Age | Less than 40 | 9 | 15 |
| 40 - 60 | 29 | 48.3 | |
| More than 60 | 22 | 36.7 | |
| Range | 35-65 | ||
| Sex | Male Female |
22 38 |
36.7 63.3 |
| Work status | Job / Business Not working |
20 40 |
33.3 66.7 |
| Social state | Married Unmarried |
42 18 |
70.0 30.0 |
| Education level | Reads and writes Diploma education Bachelor's degree Post-university qualification |
18 18 19 5 |
30.0 30.0 31.7 8.3 |
| Live in | City Village |
21 39 |
35.0 65.0 |
| Do you smoke now? | Yes No |
11 49 |
18.3 81.7 |
| Negative smoking | Yes No |
22 38 |
36.7 63.3 |
| Previously, are you smoking? | Yes No |
20 40 |
33.3 66.7 |
| Items | No = 60 | % | |
|---|---|---|---|
| Duration since diagnosis | < 1 year | 20 | 33.3 |
| From1 to 2 years | 15 | 25.0 | |
| From 2- to 3 years | 7 | 11.6 | |
| > 3 years | 18 | 30.0 | |
| Comorbidities other than cardiovascular diseases (CVDs) | Yes No |
22 38 |
36.7 63.3 |
| Previous surgery | Yes No |
17 43 |
28.3 71.7 |
| Family history of heart disease or chronic diseases? | Yes No |
27 33 |
45.0 55.0 |
Less than one-third (30.0%) of the study participants experienced heart failure for longer than three years, and more than one-third (36.7%) of them had comorbidities other than cardiovascular diseases (CVDs). This information is shown in Table 2. Furthermore, over 25% (28.3%) of the patients had undergone prior surgery.
Fig. (2) illustrates how eHealth interventions focused on self-care for study participants affected their degree of satisfaction with knowledge. Following eHealth interventions, the majority of study participants (80.0%) had a sufficient level of knowledge with a statistically significant change.
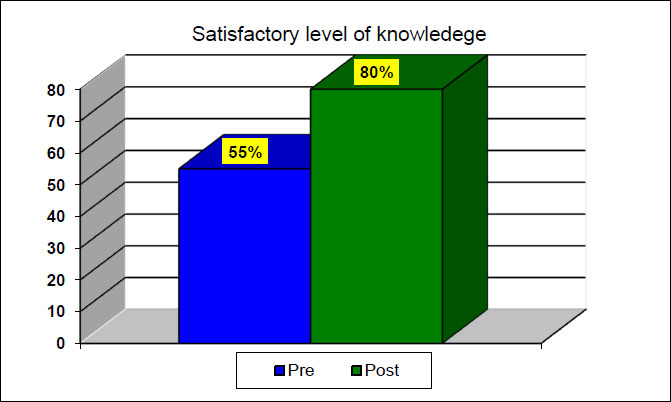
Table 3 presents the patients with CHF enrolled in the study's pre- and post-treatment perceptions of self-care maintenance, management, and trust. With one exception—“forget or fail to take any of your medicines”—all 11 self-care maintenance items had a mean of less than 2.50 in the pre-study, but the mean rises to more than 4.00 in the post-study, with a significant statistical significance (p < 0.001). According to self-care management, all six of its items aside from “Take a further diuretic” had means of more than 3.0 with positive high statistical significance (p < 0.001). Regarding confidence in self-care, four items were found to have strong statistical significance (p < 0.001): “Take action to alleviate your symptoms.” Take action to alleviate your symptoms. Take action to alleviate your symptoms and evaluate the efficacy of a medication with a p-value of less than 0.05.
| Items | Pre (n=60) Mean ± SD |
Post (n=60) Mean ± SD |
χ 2 | P |
|---|---|---|---|---|
| Self-care maintenance | ||||
| Do you weigh yourself? | 1.92 ± 0.85 | 4.37 ± 0.71 | 17.07 | .000 |
| Do you check if your ankles are swollen? | 2.05 ± 0.85 | 4.33 ± 0.47 | 18.45 | .000 |
| Do you try to avoid getting sick (for example: being vaccinated against flu, avoiding contact with sick people)? | 1.87 ± 0.94 | 4.43 ± 0.50 | 19.59 | .000 |
| Do you practice any physical activity? | 2.03 ± 0.92 | 4.45 ± 0.67 | 16.01 | .000 |
| Are you assiduous in the consultations with the doctor or nurse? | 2.20 ± 0.89 | 4.47 ± 0.74 | 15.10 | .000 |
| Do you ingest a low-salt diet? | 1.67 ± 0.79 | 4.33 ± 0.65 | 20.59 | .000 |
| Do you exercise for 30 minutes? | 1.93 ± 0.83 | 4.65 ± 0.48 | 22.37 | .000 |
| Do you forget or fail to take any of your medicines? | 4.63 ± 0.58 | 2.13 ± 0.87 | 17.17 | .000 |
| Do you request foods with a little salt when eating out or visiting someone? | 2.10 ± 0.87 | 4.53 ± 0.59 | 17.46 | .000 |
| Do you use a system (pillbox or reminders) to remind you about your medicines? | 1.63 ± 0.75 | 4.50 ± 0.59 | 22.21 | .000 |
| Keep on deep breathing exercise | 2.00 ± 0.82 | 4.45 ± 0.74 | 16.62 | .000 |
| Total score – Self-care maintenance | 24.03 ± 4.7 | 46.65 ± 3.5 | 31.73 | .000 |
| Self-care management | ||||
| How quickly did you recognize them as symptoms of heart failure? | 2.38 ± 0.61 | 3.10 ± 1.00 | 4.26 | .000 |
| Reduce the salt in your diet | 2.42 ± 0.69 | 3.10 ± 1.00 | 4.26 | .000 |
| Reduce fluid intake | 2.33 ± 0.68 | 3.23 ± 0.98 | 5.12 | .000 |
| Take a further diuretic | 2.03 ± 0.66 | 2.43 ± 1.19 | 2.37 | .021 |
| Contact your doctor or nurse for guidance | 2.30 ± 0.64 | 3.10 ± 1.00 | 5.08 | .000 |
| Think of one of the above features you tried the last time when you had trouble breathing or swollen ankles. Are you sure this feature helped you? | 2.28 ± 0.64 | 3.27 ± 0.97 | 6.58 | .000 |
| Total score – Self-care management | 13.75 ± 2.39 | 18.23 ± 4.03 | 6.96 | .000 |
| Trust in self-care | ||||
| Be free of the heart failure symptoms | 2.35 ± 0.65 | 3.40 ± 0.92 | 7.22 | .000 |
| Follow the recommended treatment | 2.55 ± 0.67 | 3.33 ± 0.95 | 4.96 | .000 |
| Assess the importance of your symptoms | 2.48 ± 0.65 | 3.17 ± 0.99 | 4.69 | .000 |
| Recognize changes in health if they occur | 2.40 ± 0.71 | 3.17 ± 0.82 | 5.20 | .000 |
| Do something that can relieve your symptoms | 2.87 ± 0.83 | 3.20 ± 0.84 | 2.17 | .034 |
| Assess whether a drug works | 2.67 ± 0.95 | 3.12 ± 0.86 | 2.84 | .006 |
| Total score – Trust in self-care | 15.31 ± 2.77 | 19.38 ± 3.63 | 6.48 | .000 |
| Total Self-Care Heart Failure | 53.10 ± 6.55 | 84.26 ± 8.55 | 21.39 | .000 |
| Items | Pre =60 Mean ± SD |
Post =60 Mean ± SD |
χ 2 | p-value |
|---|---|---|---|---|
| Swelling in ankles or legs | 1.06 ± 1.40 | 1.80 ± 1.23 | 3.255 | 0.002 |
| Sitting or lying down to rest during the day | 2.27 ± 1.55 | 1.52 ± 1.32 | 3.000 | 0.004 |
| Walking or climbing stairs is difficult | 2.23 ± 1.63 | 1.45 ± 1.39 | 3.492 | 0.001 |
| Working around the house or yard is difficult | 2.03 ± 1.65 | 1.62 ± 1.54 | 1.518 | 0.134 |
| Going places away from home is difficult | 2.28 ± 1.55 | 1.32 ± 1.26 | 2.241 | 0.000 |
| Sleeping well at night is difficult | 2.08 ± 1.58 | 1.38 ± 1.42 | 2.551 | 0.013 |
| Doing things with friends or family is difficult | 1.53 ± 1.39 | 1.28 ± 1.31 | 1.059 | 0.294 |
| Working to earn a living is difficult | 1.00 ± 1.20 | 1.55 ± 1.40 | 2.369 | 0.621 |
| Recreational pastimes, sports, or hobbies are difficult | 1.07 ± 1.24 | 1.62 ± 1.48 | 2.797 | 0.007 |
| Sexual activities are difficult | 1.33 ± 1.39 | 1.53 ± 1.52 | 0.809 | 0.388 |
| Eating less of the liked foods | 1.22 ± 1.25 | 1.92 ± 1.27 | 3.227 | 0.002 |
| Shortness of breath | 1.18 ± 1.26 | 2.11 ± 1.15 | 4.600 | 0.000 |
| Getting tired, fatigued, or having low energy | 1.16 ± 1.31 | 2.10 ± 1.32 | 4.213 | 0.000 |
| Leading cause for staying in a hospital | 1.13 ± 1.29 | 1.73 ± 1.20 | 2.819 | 0.007 |
| Costing money for medical care | 1.13 ± 1.29 | 2.13 ± 1.75 | 3.809 | 0.000 |
| Leading cause of side effects from treatments | 1.32 ± 1.40 | 2.20 ± 1.44 | 3.209 | 0.002 |
| Feeling a burden on family or friends | 1.30 ± 1.31 | 2.02 ± 1.44 | 2.798 | 0.007 |
| Feeling a loss of self-control in life | 1.20 ± 1.28 | 2.10 ± 1.42 | 3.666 | 0.001 |
| Leading cause of worry | 1.38 ± 1.26 | 2.25 ± 1.42 | 3.408 | 0.001 |
| Leading cause of difficulty concentrating or remembering things | 1.18 ± 1.20 | 2.03 ± 1.48 | 3.616 | 0.001 |
| Leading cause of feeling depressed | 1.28 ± 1.34 | 2.03 ± 1.52 | 3.072 | 0.003 |
The impact of CHF on QOL before and after self-care is displayed by mean and standard deviation in Table 4. There is statistical significance at p < 0.05 and high statistical significance at p < 0.001 in relation to quality of life for patients with CHF between pre and post.
Table 5 shows that there are high statistical significance related to total items for quality of life including” physical, emotional, and social” at p < 0.001.
| Items | Pre =60 Mean ± SD | Post =60 Mean ± SD | χ 2 | p-value |
|---|---|---|---|---|
| Physical | 16.65 ± 9.8 | 10.91 ± 8.43 | 4.00 | .000 |
| Emotional | 10.41 ± 6.66 | 6.35 ± 5.19 | 3.817 | .000 |
| Social | 14.48 ± 9.10 | 9.266 ± 8.27 | 3.565 | .001 |
5. DISCUSSION
Heart failure (HF) is a prevalent and intricate cardiovascular disorder with elevated morbidity and death rates that are anticipated to rise [26]. It significantly affects the HRQoL of the patients [27]. With an annual incidence of 32,200 cases, the estimated prevalence of HF in Saudi Arabia is 455,222 patients [6]. For patients with HF, practicing effective self-care is crucial [28, 29]. Applications for eHealth improve heart failure patients' clinical outcomes [30]. A higher quality of life is experienced by HF patients who take proper care of themselves [31, 32]. Therefore, the purpose of this study was to assess how well eHealth interventions based on self-care affected the health-related quality of life for heart failure patients.
Less than half of the patients under investigation were between the ages of 40 and 60, according to the study's findings. It could be inferred from this that cardiovascular disease is linked to advanced age. This result is consistent with that of another study [33], which discovered that fewer than half of the study's patients were between the ages of 40 and 60.
Less than two-thirds of the samples were female in terms of sex. This could be because female patients made up the majority of those who consented to take part in the study. This result conflicts with that of another study [34], which discovered that in their investigation; fewer than half of the patients with heart failure were female.
Over two-thirds of the patients included in this study were married. This could be because the patients under study ranged in age from 25 to 65. This result is consistent with that of another study [35], which discovered that in his study, over half of the individuals suffering from heart failure were married.
Less than one-third of the patients under investigation had bachelor's degrees, affording to the study's findings about the patients' educational backgrounds. This may have to do with the fact that educated patients find eHealth interventions to be user-friendly. This result disagrees with that of [36], who said that over 10% of the samples in his investigation had bachelor's degrees. Furthermore, about two-thirds of the patients came from rural regions. This result conflicts with that of another study [37], which discovered that roughly 25% of the study's patients came from rural areas.
According to the study's findings, two-thirds of the patients were not working. This may have something to do with the fact that more than one-third of the patients in the study were above 60 years old, and less than two-thirds of the patients were female. This result conflicts with that of another study [38] in which the authors discovered in their investigation that over one-third of patients with heart failure were not working.
In terms of smoking, it was discovered that the vast majority of the patients under investigation did not smoke. This finding may be related to the fact that the analyzed sample contained the biggest proportion of females, as smoking is not customarily associated with ladies in Saudi society. This outcome was in line with the findings of another study [33], which discovered that over 75% of the patients in their investigation did not smoke.
Less than one-third of the people in the research have been unwell for longer than three years. This may be explained by the rising death rate among HF patients, particularly those who smoke, have comorbidities, or are elderly. This finding was consistent with that of another study [36], which discovered that slightly over one-third of the patients in their investigation had been unwell for longer than three years.
More than one-third of the patients in the current study have comorbidities other than cardiovascular disease, according to the study's findings. This may have something to do with the fact that HF is often accompanied by comorbidities. This conclusion was corroborated by another study [38], which discovered that comorbidities other than cardiovascular disease were present in more than 25% of the research participants.
A noteworthy discovery from this investigation is that the BMI of almost 10% of the patients was less than 25. This may have to do with the fact that the leading cause of coronary heart disease development is fat. This result is consistent with that of another study [37], which discovered that the BMI of over 10% of the patients in the study was less than 25.
The results of the current study presented that there was a statistically significant difference in patients' knowledge between pre- and post-eHealth interventions-based self-care in terms of their assessment of their knowledge. The present study's findings regarding knowledge gaps may be associated with the impact of eHealth interventions and the ease with which patients can obtain timely and comprehensive information via WhatsApp applications. This is comparable to the findings [39] that reported that following the adoption of a nurse-led education program, patients with heart failure showed improvements in their understanding.
The current study's findings concerning self-care exposed that there were statistically significant differences between the study group's before and after eHealth interventions-based self-care. These variations observed within the research population may be linked to self-care apps based on eHealth treatments, which encourage patients and may ultimately lead to better health outcomes. This result [40] found that patients' Self-care Heart Failure Index management scores improved more when they participated in an empowerment-based self-care teaching program. These results were consistent with [39] the discovery that self-care confidence, self-care management, and self-care maintenance were all enhanced in heart failure patients through nurse-led education programs.
In this study, the study group's health-related quality of life (hr-QOL) varied statistically significantly before and after the application of eHealth interventions-based self-care. The observed variation in HR-hr-QOL within the examined cohort may be associated with eHealth interventions; following eHealth interventions, patients acquired increased knowledge and abilities to prevent and handle problems and side effects. This was corroborated [41] with claims that the terms of improving the health-related quality of life for people with heart failure, home-based cardiac therapy is superior to mainstream care.
In summary, the study's findings are consistent with the research hypothesis, which states that cases with heart failure will acknowledge an improvement in their health-related quality of life if they practice self-care based on eHealth interventions. This is consistent with another study [42], which discovered that patients' HRQOL was higher after receiving cardiac rehabilitation.
CONCLUSION
The study's findings lead to the following conclusion, which is suggested: The self-care score of the Heart Failure Index (SCHFI), the Minnesota Living with Heart Failure Questionnaire (MLHFQ), and patient knowledge were significantly improved as a result of eHealth interventions-based self-care. These results suggested that eHealth interventions-based self-care, when used as an adjuvant intervention, may have been crucial in the management of HF patients who were receiving the right pharmaceutical therapy and were clinically stable. Self-care based on eHealth interventions raises the quality of life in relation to health.
RECOMMENDATION
In light of the study's findings, it is advised that nurses take an active part in promoting self-care awareness by putting healthcare programs into place. Patients should be given an illustrated self-learning package that is simplified to help them comprehend the course of therapy and how to take care of themselves. For HF patients to experience an optimal quality of life, education is essential. To generalize the findings, more investigation and a large sample size replication of this study are required.
AUTHORS' CONTRIBUTIONS
R.M.R., A.A., N.A. A., and E.H. contributed to the ideation, analysis, and writing of this manuscript. R.M.R. was assigned to data collection and funding acquisition with the Deputyship for Research and Innovation at Shaqra University. All authors had access to all derived datasets. All authors have read and agreed to the published version of the manuscript.
LIST OF ABBREVIATIONS
| HF | = Heart failure |
| HRQoL | = Health-related quality of life |
| MLHFQ | = Minnesota Living with Heart Failure Questionnaire |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was evaluated and approved by the scientific Research Ethics Committee at Shaqra University.
HUMAN AND ANIMAL RIGHTS
No animals were used that are the basis of this study. All the human procedure ware performed in accordance with the helsinki declaration.
AVAILABILITY OF DATA AND MATERIALS
The authors confirm that the data supporting the findings of this study are available within the article and its supplementary materials.
STANDARDS OF REPORTING
CORREQ guidelines were followed.
FUNDING
This study was funded by . Shaqra University, Funder ID. SU-ANN-202251, Awards/Grant number. Twenty thousand Saudi riyals.
CONFLICT OF INTEREST
The authors have declared no conflict of interest.
ACKNOWLEDGEMENTS
The authors extend their appreciation to the deanship of scientific research at Shaqra University for funding this research work through the project number (SU-ANN-202251). The authors would also like to acknowledge all the respondents, who helped the researchers in data collection but were not involved in the study design, analysis, interpretation of data, or writing of the manuscript.

