All published articles of this journal are available on ScienceDirect.

The Effect of Virtual Reality and Hugo Point Massage on the Pain and Anxiety of School-aged Children with Cancer: Crossover Clinical Trial
Authors Info & Affiliations
Abstract
Background:
Venipuncture and peripheral intravenous cannulation are two of the most common invasive procedures in children that generate pain and distress. Previous studies have confirmed the effect of distraction and acupressure on reducing pain and anxiety in children; however, the effectiveness of these two methods has not been compared.
Objective:
The aim of this study was to compare Virtual Reality and Hugo point massage on the pain and anxiety of children.
Methods:
This crossover study was conducted in the oncology unit of a children’s hospital. Participants included 30 children aged 6-12 with cancer who were randomly assigned to one of the three groups: (routine, Virtual Reality, and acupressure). All children experienced these three methods. The scores of children’s pain (VAS scale) and anxiety (FAS scale) were measured.
Finding:
The result showed that the Virtual Reality method significantly reduced pain and anxiety compared to Hugo’s point method (P <0.001).
Implications for Nursing:
According to the present study, non-pharmacological methods such as Hugo point massage and virtual reality were effective in reducing pain and anxiety in school-aged children. Therefore, nursing managers can encourage nurses to use these methods based on the child's preferences to relieve the pain by providing the necessary facilities and equipment. Furthermore, they can increase nurses' knowledge by introducing new pain management methods in children through workshops.
Conclusion:
The present study showed that VR and Hugo’s point massage were effective ways to reduce pain and anxiety resulting from intravenous cannulation in school-age children.
Clinical Trial Registration Number: IRCT20100823004617N14.
1. INTRODUCTION
Cancer is the second leading cause of death in children and adolescents [1]. Cancer cause 20.1% of all deaths in children aged 5-9 years [2]. Cancer treatment is time-consuming and often requires the child to be hospitalized. During hospitalization, the child is exposed to invasive and repeated painful procedures [3, 4]. Children with cancer undergo several potentially painful procedures, such as accessing the peripheral or central venous or bone marrow aspiration [5]. These procedures can cause pain in the child [6]. Pain has numerous psychological effects, such as stress, fear, and anxiety [7]. Anxiety is a mental, emotional response to stressful factors [8].
Conducting painful medical procedures in these children is unavoidable [9, 10]. Venipuncture and peripheral intravenous cannulation are two of the most common invasive procedures in children [11-14] that generate pain and distress [15, 16]. Management of pain and anxiety during venipuncture is performed using pharmacological and non-pharmacological methods [17].
Non-pharmacological methods are recommended to relieve pain related to venipuncture /peripheral intravenous cannulation in children [15, 18]. These methods include Physical (sensory), Psychological, and Spirituality and religious interventions [19].
Among non-pharmacological methods, distraction is one of the most practical, straightforward, and cost-effective methods for relieving pain and anxiety [20-22]. Distraction is the shift of attention from painful stimuli to more attractive or pleasurable ones [23]. According to a study, distraction techniques can reduce pain and anxiety in children [24-26]. There are numerous types of distraction, including visual, auditory, tactile, and mental [22], and choosing a distraction type is directly related to the age of the child [21]. Virtual reality (VR) is one of the ways of distraction. In this method, computerized technology is used to immerse a person in a multi-sensory, three-dimensional environment [27]. A systematic review recommended further research on the effect of VR associated with medical procedures due to insufficient research in this field [28].
Another non-pharmacological method in the physical intervention group is acupressure [21, 24, 29]. This safe, straightforward and inexpensive method is recommended by the World Health Organization [30, 31]. The points used in acupuncture are massaged [30]. Hugo point (LIIV) is the most important analgesic point of the body, located between the first and second metacarpals bones [32, 33]. According to the gate control theory of pain, massage can effectively close the gate. In other words, by stimulating the large nerve fibers, the perception of pain changes, preventing the transmission of painful stimuli [34]. According to the American Academy of Pediatrics, pain is an intrinsic multifactorial experience and should be evaluated and treated [24]. Preventing pain in children is a moral commitment [18], and nurses have an influential role in pain management. Therefore, their pain management program might impact patients' pain experience [35].
Previous studies have confirmed the effect of distraction and acupressure on reducing pain and anxiety in children; however, the effectiveness of these two methods has been less compared. Thus, the aim of this study was to compare the effectiveness of the two non-pharmacological techniques, namely Virtual Reality and Hugo’s point massage, on the pain and anxiety of children undergoing intravenous cannulation.
2. MATERIALS AND METHODS
2.1. Trial Design
This crossover randomized clinical trial study was conducted from November 2019 to May 2020 in Iran.
2.2. Participants
Participants included 30 children aged 6-12 with cancer admitted to the oncology unit. The oncology unit is a referral center with approximately 40 beds, in which children with Anemia, leukemia (ALL, AML), Congenital coagulation diseases, Nephroblastoma, and Neuroblastoma are admitted. Participants were included in this study through a convenience sampling method.
2.2.1. Eligibility Criteria for Participants
Inclusion criteria included experience with peripheral intravenous cannulation, alertness, and the ability to communicate verbally. Children who had used pain relievers 8 hours before intravenous cannulation or had a previous injury at the site of Hugo’s point were excluded from the study.
2.3. Study Setting
This study was conducted in a children’s hospital, a referral center in East Azerbaijan, Iran.
2.4. Procedures
Peripheral intravenous cannulation was performed with peripheral IV catheter No.22-24 (Soha Company) for all children by a skilled and experienced nurse. In both groups, the mother was present at her child's bedside during the procedure.
2.4.1. Control Group
In the control group, the child was comforted only by the mother; consequently, before, during, and after the procedure, the mother performed multisensory interventions such as talking, touching, kissing, and eye-to-eye contact with the child.
2.4.2. Virtual Reality (VR)
In this method, in addition to maternal multisensory interventions, from five minutes before the intravenous cannulation, until the end of it, a “SpongeBob” cartoon was shown through a cyberspace camera placed over the patient's eyes and ears.
2.4.3. Hugo’s Point Massage
In addition to maternal multisensory interventions, five minutes before the intravenous cannulation, Hugo’s point in the opposite hand was massaged in a circular motion, in a clockwise direction, with moderate pressure by researcher who was previously trained in this field. The maximum pressure time was one minute at a time, and then the massage was interrupted for 10 seconds. This operation continued until the intravenous cannulation was completed.
2.5. Randomization and Allocation
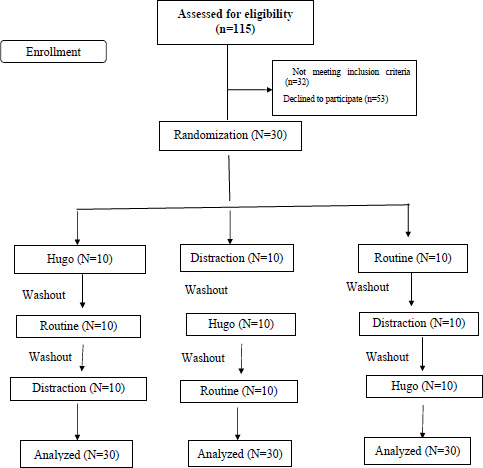
Randomization was conducted using a randomized block design with blocks of 6 and 9. Allocation concealment was performed using sealed envelopes with consecutive numbers. The child was asked to choose one of the sealed envelopes. Each envelope contained a triple block (A=VR, B = Hugo’s point massage, C= routine) showing the order of the intervention on the child. For example, if the blocking arrangement assigned to the child was ABC, the child would experience VR, Hugo’s point massage, and routine interventions sequentially. The washout period was considered to be 24 to 72 hours. If a child needed peripheral intravenous cannulation less than this time, he/she would be excluded from the study.
2.6. Outcome Measure
In this study, Visual Analog (VAS) [37] and Faces Anxiety Scales (FAS) were used to measure child pain and anxiety, respectively [38].VAS scale is a 10-cm horizontal line that includes a range from painless to most painful, in which the child is asked to mark the area on the line that best describes the amount of pain experienced immediately after the intravenous cannulation. The FAS scale is made up of drawings of five faces. The left and right images of the scale indicate the absence and the highest level of anxiety, respectively. The scores on the instrument range between 0-10.
Children’s pain and anxiety were measured five minutes before and one minute after the procedure. To calculate the child's pain score, one minute after the procedure, the researcher’s assistant asked the child to show the amount of pain during the procedure on the scale. The distance between the point indicated by the child and the pain-free point was measured with a ruler and recorded as the child's pain or anxiety score.
Blinding the participants was unattainable; however, the co-researcher responsible for collecting the data and those who analyzed the data were blind to the study groups.
2.7. Sample Size
The sample size was determined based on Lestari et al.’s study, 2017. Considering the pain mean differences in the intervention group (4.11±1.79) and the control group 5.79±1.78), 95% confidence interval, a significance level of one-sided α = 0.05, 80% power, and 1: 1 allocation ratio, the sample size was obtained as 24 participants, which increased to 30 considering a 20% potential attrition rate [36].
2.8. Ethical Consideration
This study was approved by the Ethics Committee of Tabriz University of Medical Sciences (registered in the international center for the registration of clinical trials in (IRCT20100823004617N14). Researchers explained the purpose of the study to the child and his/her parents before collecting the data and then obtained informed written consent from them. Participants had the right to withdraw from the study at any stage.
2.9. Data Analysis
Data were analyzed using SPSS software version 26. The normality of the data was assessed using the Kolmogorov-Smirnov test. Descriptive statistic tests such as Frequency (percentage) and mean ± standard deviation were used to describe qualitative and quantitative data. In addition, a paired sample t-test was used to compare intra-group pain and anxiety scores before and after the intervention. One-way ANOVA was applied to compare children’s pain and anxiety scores between the groups. The level of statistical significance was considered less than 0.05% (Fig. 1).
3. RESULT
In the present study, 115 children were selected: 32 children due to lack of inclusion criteria (17 children due to having a central vein, 5 vision problems, 10 the first experience of venipuncture) and 53 children for decline to participate (20 child's restlessness, 8 parents' refusal to take the child's vein, 25 parents' lack of belief in the effectiveness of interventions) were excluded from the study. Finally 30 children were studied. The mean age of the children was 9.1±1.82. Children’s most common type of cancer was acute lymphocytic leukemia (ALL), with 13 cases (43.3%). The children’s demographic characteristics are provided in Table 1.
| Variable | - | N (%) |
| Gender | Boy | 16 (53.3) |
| Girl | 14 (46.7) | |
| Place of residence | City | 12(40) |
| Village | 18(60) | |
| Economic situation | Poor | 15(50) |
| Modrate | 10(33.3) | |
| Good | 5(16.7) | |
| Type of Cancer | ALL | 13 (43.3) |
| AML | 5 (16.7) | |
| Hodgkin's lymphoma | 4 (13.3) | |
| Sarcoma | 2 (6.7) | |
| Neuroblastoma | 6 (2) | |
| Mean ± Sd | ||
| Number of Hospitalizations | 2.9 ± 1.06 | |
| Number of Times chemotherapy | 3.23 ± 1.14 | |
| Variable | Method | Pre-test | Post-test |
Intra-group Comparison P-value |
| Mean± SD | Mean± SD | |||
| Anxiety | Virtual reality | 6.27 ± 1.79 | 3.07 ± 1.26 | P< 0.001* |
| Hugo | 6.67 ± 1.42 | 5.00 ± 1.72 | P< 0.001* | |
| Routine | 6.53 ± 1.73 | 6.13 ± 1.74 | P= 0.23* | |
| Inter-group comparison P-value |
P>0.05** | P<0.001** | ||
| Pain | Virtual reality | 1.43 ± 1.19 | 3.86 ± 1.11 | P< 0.001* |
| Hugo | 1.75 ± 0.91 | 5.31 ± 1.14 | P< 0.001* | |
| Routine | 2.15 ± 0.99 | 7.16 ± 0.96 | P= 0.888* | |
| Inter-group comparison P-value |
P>0.05 ** | P<0.001** | - | |
** One-away ANOVA.
| Variable | Method | Pre-test | Mean Difference (confidence limits) | P-value |
| Mean± SD | ||||
| Anxiety | Virtual reality | Hugo | 1.93 (-1.32 to -2.55) | <0.001* |
| Routine | -3.07 (-2.39 to -3.74) | <0.001* | ||
| Hugo | Virtual reality | 1.93 (1.32 to 2.55) | <0.001* | |
| Routine | -1.13 (-0.46 to -1.86) | <0.001* | ||
| Routine | Virtual reality | 3.07 (2.39 to 3.74) | <0.001* | |
| Hugo | 1.13 (0.46 to 1.81) | <0.001* | ||
| Pain | Virtual reality | Hugo | -1.52 (-1.01 to -2.04) | <0.001* |
| Routine | -3.31 (-2.75 to -3.86) | <0.001* | ||
| Hugo | Virtual reality | 1.52 (1.01 to 2.04) | <0.001* | |
| Routine | -1.78 (-2.15 to -1.42) | <0.001* | ||
| Routine | Virtual reality | 3.31 (2.75 to 3.86) | <0.001* | |
| Hugo | 1.78 (1.42 to 2.15) | <0.001* |
The intra-group comparison showed that the child's pain and anxiety scores decreased after intervention in VR and Hugo’s methods, which was statistically significant (P <0.001). Although the pain and anxiety scores decreased in the control group, it was not statistically significant (P <0.05). ANOVA test was used to compare the inter-group mean pain and anxiety scores. The results showed that children in Hugo’s and VR methods experienced less pain and anxiety than the control group, which was statistically significant (P <0.001) (Table 2).
The Post-Hoc Tukey test was used to determine the most effective method for relieving the child's pain and anxiety. The results showed that the lowest score of the child's pain and anxiety was related to VR, the pressure, and the control group, respectively (P <0.001) (Table 3).
4. DISCUSSION
The aim of this study was to investigate the effectiveness of two non-pharmacological methods, namely VR and Hugo’s point massage, on the pain and anxiety of children aged 6 to 12 years undergoing intravenous cannulation. The result showed that despite the effectiveness of both methods in relieving children's pain and anxiety, VR was more effective than Hugo’s point massage.
The effectiveness of acupressure on children's pain and anxiety resulting from venipuncture has been reported in previous studies [16, 41], in which the pain and anxiety scores in the acupressure group were lower than the control group.
In the present study, pain and anxiety scores in the VR group were lower than in the control group. These results are in line with previous studies. In this regard, studies showed that children in the VR group experienced less pain than the control group during painful procedures [7, 38-43]. Moreover, a study by Ryu, 2019 showed that VR was effective in reducing preoperative anxiety in children [44]. VR increases the pain threshold by diverting the child's attention [44-46].
In the study by Burns-Nader et al., using distraction was ineffective in reducing the pain and distress of children aged 4-11 years [47]. The probable reason for the difference between the findings of this study and the present study is the difference in the type of distraction. In this study, a tablet was used for child distraction.
In the present study, VR had a more significant effect in decreasing children's pain and anxiety than Hugo’s point massage. The researchers did not find a similar study in this regard.
VR offers an innovative method to manage pain through the integration of immersive visual and auditory techniques [48]. In fact, audiovisual distraction is a strong and effective intervention for pain relief in school-age children [25]. According to previous studies, distraction methods, such as three-dimensional VR glasses, are as effective in reducing pain, fear, and anxiety in children as medical techniques [49]. It seems that the VR method is a multi-sensory intervention and is, therefore, more effective than Hugo’s point massage, which is a mono-sensory intervention.
It is better to apply pain reduction techniques according to children’s age and mental and physical status. In school-age children vision development and coordination between the optic nerve and muscle have taken place, and the child is fascinated by exciting computer and electronic games [50]. A review study recommends the use of Hugo’s point massage at ages 6 to 12 and VR at ages 8 to 12 to reduce the pain of venipuncture in children [24].
To the best of the authors' knowledge, this was the first study to compare the effectiveness of Hugo’s point massage and VR. In this study, the crossover method was used, which is a powerful method for controlling confounders. One of the limitations of the present study was the participants’ limited age range. School-age children 6 - 12 years were studied, which resulted in a small sample size and a prolonged sampling period.
CONCLUSION
The present study showed that VR and Hugo’s point massage were effective ways to reduce pain and anxiety resulting from intravenous cannulation in school-age children. Therefore, nursing managers can encourage nurses/ occupational therapists to use these methods based on the child's preferences to relieve the pain by providing the necessary facilities and equipment. Furthermore, they can increase nurses' knowledge by introducing new pain management methods in children through workshops. In this study, the effect of VR and Hugo’s point pressure on children's pain and anxiety were compared due to the lack of studies in this field. It is suggested that more studies be conducted.
ETHICS APPROVAL AND CONSENT TO PARTI-CIPATE
The research was initiated after confirmation by the Ethical Committee (IR.TBZMED.REC.1398.115), of Tabriz University of Medical Sciences and registries in Iran Clinical Trial Registration Center (IRCT20100823004617N14)9).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from all participants
STANDARDS OF REPORTING
CONSORT guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
The datasets generated and/or analyzed during the present study are in Persian and are not publicly available due to the confidentiality of the participants, yet they are available from the corresponding author at reasonable request [M.J].
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
ACKNOWLEDGEMENTS
The authors would like to thank the Research Deputy of Tabriz University of Medical Sciences (Iran) for approving the research, as well as the mothers and children who participated in this study.

