All published articles of this journal are available on ScienceDirect.

Determinants of Parents’ Knowledge, Attitudes, and Practice toward Childhood Vaccination: A National Study
Authors Info & Affiliations
Abstract
Background:
Childhood vaccination is one of the World Health Organization's strategies to reduce vaccine-preventable diseases and children's mortality and morbidity rates. Adequate and accurate knowledge, as well as positive attitudes regarding vaccination, may increase parents’ compliance with their children’s vaccines.
Objective:
This study aimed to identify the determinants of parents’ knowledge, attitude, and practice toward childhood vaccination in Jordan.
Methods:
This is a descriptive cross-sectional study. The stratification method of sampling technique was used to split Jordan into three regions. The sample included 1477 participants. A total number of eleven Maternal and Child Health Care centers were selected as the study’s site.
Results:
Results showed that parents have sufficient knowledge regarding the importance of vaccines in maintaining a child’s health, with a mean percentage of correctly answered questions of 78.7%. However, they have inadequate knowledge regarding the adverse reactions (57.5%) and the contraindications of vaccines (61.8%). Parents had positive attitudes regarding the National Immunization Program where 97% agreed with it. However, 83% of parents had negative attitudes toward vaccine safety. Parents’ work, residency, income, and age are significant determinants of parents’ attitudes, knowledge, and practice regarding children's vaccines.
Conclusion:
The study may motivate nurses to implement more educational interventions regarding children’s vaccination to upgrade parents' knowledge with particular emphasis on parents with a low level of education and the residents of rural areas.
1. INTRODUCTION
Vaccination is a significant component of primary health care services to prevent and control infectious disease outbreaks [1]. Among children, death caused by infectious diseases is reduced by 2-3 million each year by using vaccines [2]. Therefore, childhood vaccination is one of theWHO’s strategies for reducing vaccine-preventable diseases, children mortality and morbidity rate, and medical costs related to infectious diseases, which may guarantee a better quality of life for children [3-5]. The WHO has established a framework; the Global Vaccine Action Plan; that aims to have a world free of vaccine-preventable diseases by 2020; unfortunately, most children around the world- especially in developing countries- did not reach the targeted global vaccination coverage of 90% [6, 7].
1.1. Background
The vaccination programs start vaccines during the neonatal period to help infants develop proper immunity against many communicable diseases. Most of these programs in Middle Eastern countries were launched by the WHO and were focused on the first 24 months of life [8]. Parents’ accurate knowledge and positive attitudes regarding children’s vaccines are crucial factors in increasing the rate of vaccination coverage. Although vaccines are broadly known as a major contemporary means to prevent diseases, people still have conflicting attitudes toward vaccines' benefits and safety. Many sources might be available where parents can get information about vaccines, which may lead to inaccurate information and many misconceptions regarding vaccines [9]. Providing good communication channels between parents and healthcare providers would minimize this issue [8]. The high vaccination coverage rates do not necessarily indicate the absence of parental concerns regarding the vaccination of their children. Therefore, assessing parents’ knowledge, attitudes, and practices (KAPs) toward vaccination would be worthy to identify their misconceptions [4]. In addition, assessing parents’ characteristics and their effect on vaccination coverage is essential to identify determinants associated with their KAPs toward children's vaccines, which may help decision-makers establish successful vaccination plans [5, 6].
Parents’ lack of knowledge and negative attitudes regarding children’s vaccines were found in different countries and were associated with poor immunization status of children [4, 5, 10]. There is a cultural belief that vaccines may cause autism and mild illness, resulting in a delay in children's vaccination schedules [3, 6, 11]. Unfortunately, higher incidences of vaccine-preventable diseases such as poliomyelitis and measles were reported among children in different countries such as; Malaysia, Nepal, Pakistan, Nigeria, and South Sudan [12-15], which could be related to the fear that western countries developed vaccines to harm Muslims or that vaccines contain parts from pigs [16]. Other reasons could be concerns about the safety of vaccines, fears related to possible adverse events following vaccination, and the current powerful anti-vaccine movements in some communities [9]. Other studies reported that parents had inadequate knowledge about vaccines but showed positive attitudes toward them [3, 16]. Socio-demographic factors such as parents’ age and educational level, family income, and family size were reported as associated factors of parents’ KAPs towards children's vaccines [4, 6, 8, 10]. For example, negative attitudes among parents were higher among those with higher educational levels, older ages, and living in towns [16]. A recent systematic review regarding parental vaccine attitudes and beliefs measured parents’ intentions to vaccinate their children for one or more antigens, they found 16 studies directly asking parents about their intentions, among these the highest report was from Canada where 98% of the 54 participating parents intended to vaccinate their children, and the lowest was 75% in a study included 200 parents in the United States [17].
In Jordan, the Ministry of Health (MOH) is the main sector that offers free-of-charge vaccines to all eligible children regardless of their nationality. The vaccination coverage rate was 98% for all scheduled vaccines of the National Immunization Program (NIP), which was high compared to that in developed countries [18]. Children under the age of two-year-old should complete the following doses of vaccines: One dose of Bacillus Calmette-Guerin (BCG) soon after birth; four doses of diphtheria, tetanus, and pertussis (DTP) at second, third, fourth, and 18 months; three doses of Rota, Hepatitis B virus, Haemophilus influenza type b, and Inactivated polio vaccines (HBV, HiB, IPV) are given at second, third, and fourth months of age respectively; four doses of oral poliovirus (OPV) at third, fourth, ninth, and 18 months; one dose of Measles at nine months; and two doses of mumps, measles, and rubella (MMR) at 12 and 18 months [19]. Despite the importance and literature’s strong indication that parents play a significant role in their children’s vaccination, studies that targeted parents' KAPs regarding children's vaccines and their determinants in Jordan are not well addressed by research. Therefore, this study aimed to examine this issue and assess parents' compliance with the NIP and the determinants that may affect their compliance. Nurses have a vital role in childhood vaccination as children’s vaccines are often administered by them. Therefore, the study findings may motivate nurses and other healthcare providers to implement effective health education programs to enhance parents’ KAPs regarding children’s vaccines.
1.2. Research Questions
This study aims to answer the following questions:
(1) What knowledge, attitudes, and practices do parents have regarding children’s vaccines?
(2) Are there significant differences in Jordanian parents' knowledge, attitudes, and practices to vaccination based on their demographic characteristics?
(3) Are parents compliant with the National Immunization Program?
2. METHODOLOGY
2.1. Design
A descriptive cross-sectional design was used to assess parents’ KAPs regarding children's vaccines using a self-reported questionnaire. Another retrospective design was used to investigate parents' compliance with the NIP.
2.2. Methods
A stratification method of sampling technique was used to split Jordan into three regions (south, middle, and north) based on the administrative division of Jordan into these regions. A total number of eleven Maternal and Child Health Care (MCHC) centers were selected using a random sampling method by choosing every fifth center out of a list containing all the available centers ordered alphabetically. Three MCHC centers from the south, three from the north, and five from the middle region were chosen; because the middle region contains the largest number of MCHC centers in Jordan. Data were collected from December 2018 to June 2019.
Parents from the selected settings were chosen conveniently to participate in the study. The inclusion criteria were; a parent (mother, father, or relative) who can read and write the Arabic language, has one or more healthy children aged two to five years and referring to one of the MCHC centers in Jordan. On the other hand, parents who had children under the age of two years were excluded because of the incomplete vaccination status of their children, in addition to parents who had children with chronic diseases because those children have a different vaccination program.
Data were gathered using a self-administered questionnaire which consists of four parts; the first part asked about the parent’s socio-demographic characteristics and was developed by the researchers after reviewing different literature related to the topic. The second one assessed parents’ knowledge about vaccination which included 11 statements, and the responses to the statements were recorded as “Yes”, “No”, and “Do not Know” [11]. The third part examined parents' attitudes toward children's vaccines using three point-Likert scale items with the following responses: “Agree”, “Not Sure”, and “Disagree” [10]. The last part evaluated the parents’ practices toward children's vaccines with six closed-ended questions [11]. The knowledge and practice scales were used in a study conducted in Saudi Arabia [11], and the attitude scale was used in a study in Yemen [10], both reported pre-testing of the scales. In the current study, a pilot test was conducted to evaluate the psychometric properties of our version, Cronbach’s alpha for the knowledge and practice scales were .76 and for the attitude scale, it was .73. Almost 15 minutes were needed to complete the questionnaire.
The questionnaire was translated into the Arabic language (the native language of the participants) using forward and backward translation. Two bilingual researchers translated the questionnaire from English to Arabic language, and then a third researcher translated it back from Arabic to English. Later, two colleague faculty members compared the meaning equivalency of the two versions. Few incongruities were found, and the researchers agreed on the final wording. Lastly, a consultation with an expert in instrument development was sought. Furthermore, the translated questionnaire was used in the pilot study to ensure that it is comprehensible to the participants and feasible to be used in data collection. The pilot study results did not reveal a need for any changes.
Parents’ compliance with the NIP was evaluated retrospectively by reviewing the children’s vaccination records available in the MCHC centers. A child with a complete record according to the NIP with no missing doses was considered compliant, while the child with partial immunization with at least one missing dose was considered non-compliant.
Cohen's table (1992) [20] was used to calculate the sample size as follows; a small effect size to have more accurate results, Power= 0.80, and α= .05, and using Analysis of Variance (ANOVA) test with four groups based on the type of setting where parents seek vaccination healthcare. Sample size estimation showed the need for 274 participants for each group which was 1096 for four groups. 35% was added to overcome the attrition rate. Eventually, 1500 participants were asked to be part of the study.
2.3. Analysis
The Social Package for Social Sciences (SPSS, version 23.0) was used to enter and analyze the study’s data. Data screening and cleaning were conducted prior to the data analysis process. Descriptive statistics, including means, frequency, and percentage, were used to describe parents' demographics and the main study variables, parents’ KAPs toward vaccination, and compliance with the NIP. In addition, a series of Student T-tests for independent groups and analysis of variance (ANOVA) tests were conducted to describe the significant differences in the parents’ KAPs toward vaccination based on their demographics. Moreover, linear and multiple regression were used to assess the factors associated with the parent's compliance with the NIP. The total percentage for some questions from the included data in the analysis is less than 100%, which indicates that the missing data were not replaced as these were less than 5%.
3. RESULTS
A total of 1500 questionnaires were distributed among the participants. The returned questionnaires were 1486. After data screening, nine questionnaires were omitted because of missing data. The final number of questionnaires included in the analysis is 1477, with a response rate of 98.4%. The sample included 1226 (83%) mothers and 186 (12.6%) fathers. The highest percentage of the participants have a university education degree 831 (56.3%), 589 (39.9%) are employed, and 1115(75.5%) are working in the non-medical field. However, Table 1 shows further details about the participants' characteristics.
3.1. Parents' KAPs toward Vaccination
Data revealed that parents have sufficient knowledge about vaccination. The correctly answered questions ranged from 57.5% to 92.5%, with a mean percentage of 78.7% (Table 2). The highest two percentages were for the question that asked “vaccination is very important for children from the first day of birth” 1366 (92.5%), and the question “vaccination could maintain child health” 1342 (90.9%). On the other hand, the lowest two percentages were for the question that asked about convulsions and skin rash as the adverse reactions to vaccination 850 (57.5%) and for the question that asked about malnutrition, low-grade fever, and diarrhea as the contraindications for vaccination 913 (61.8%).
Regarding attitudes, results showed that parents have positive attitudes toward vaccination with a high percentage of 90% (Table 3). Generally, 1432 (97%) of the parents agreed with the NIP, and 1377 (93.2%) of them perceived that vaccination is essential for children. The lowest percentage of attitudes scores was about vaccinations being safe for children 1226 (83%).
Regarding parents’ practices (Table 4), the mean score of the good practice patterns was 77.5%. Furthermore, data showed that the best practices were regarding parents' commitment to the NIP 1370 (92.8%) and using antipyretics to manage fever resulting from vaccination 1361 (92.1%). Conversely, the lowest practice score was for searching for other available vaccines than those in the NIP 529 (35.5%). For data distribution, data were normally distributed while the skewness for knowledge, attitudes, and practice scales were (.78, -.26, and 1.3, respectively).
| Variable | n(%) |
|
Age <18 year 19-40 year > 40 year |
148 (10) 1126 (76.2) 150 (10.2) |
|
Relationship Father Mother Other |
186 (12.6) 1226 (83) 55 (3.7) |
|
Marital Status Married Divorced Widowed |
1275 (86.3) 115 (7.8) 67 (4.5) |
|
Number of Children One 2-3 >3 |
326 (22.1) 793 (53.7) 333 (22.5) |
|
Education Level Illiterate School University |
63 (4.3) 574 (38.9) 831 (56.3) |
|
Employment Status Employed Unemployed |
589 (39.9) 830 (56.2) |
|
Parents' Profession Medical field Non-medical field |
339 (23) 1115 (75.5) |
|
Family Income <300JD 300-600JD 600-1000JD >1000JD |
373 (25.3) 750 (50.8) 269 (18.2) 66 (4.5) |
|
Decision Maker Father Mother Both |
101 (6.8) 693 (46.9) 622 (42.1) |
|
Residency Urban Rural |
810 (54.8) 618 (41.8) |
|
Governorate South Middle North |
304 (20.6) 600 (40.6) 573 (38.8) |
|
Settings Public medical center Public hospital Private clinic Private hospital |
1437 (97.3) 19 (1.3) 12 (.8) 4 (.3) |
| No. | Question | n (%) |
| 1 | Vaccination is very important for children from the first day of birth | 1366 (92.5) |
| 2 | Vaccination prevent infectious disease | 1175 (79.6) |
| 3 | Vaccination decreases the rates of mortality and disabilities | 1229 (83.2) |
| 4 | Vaccination could maintain child health | 1342 (90.9) |
| 5 | Diphtheria, Tetanus and pertussis could be controlled by vaccination | 1161 (78.6) |
| 6 | Hepatitis B virus could be prevented by vaccination | 1061 (71.8) |
| 7 | The childhood vaccines could control Measles | 1102 (74.6) |
| 8 | Malnutrition, low fever and diarrhea are not contraindications for vaccination | 913 (61.8) |
| 9 | Some vaccines are associated with fever and pain | 1276 (86.4) |
| 10 | Vaccination could result in convulsions and skin rash | 850 (57.5) |
| 11 | Even healthy child need vaccination | 1312 (88.8) |
| No. | attitude | n(%) |
| 1 | In favor of vaccination program | 1432 (97) |
| 2 | Child vaccination is important | 1377 (93.2) |
| 3 | Vaccination is more beneficial than harmful | 1272 (86.1) |
| 4 | Vaccines for child immunization are safe | 1226 (83) |
| 5 | Important to follow vaccination schedule | 1359 (92) |
| 6 | Vaccination keeps your child healthy | 1356 (91.8) |
| No. | Practice | n(%) |
| 1 | Do you follow the obligatory vaccination programs? | 1370 (92.8) |
| 2 | Will you search for other available vaccines for your children? | 529 (35.8) |
| 3 | Will you manage swelling by cold compress? | 1148 (77.7) |
| 4 | Will you use analgesics for swelling and pain after vaccination? | 1199 (81.2) |
| 5 | Will you use cold compress for fever resulting from vaccination? | 1261 (85.4) |
| 6 | Will you use antipyretics for fever resulting from vaccination? | 1361 (92.1) |
3.2. Differences between Parents' KAPs Based on their Demographics
Further analysis suggested several significant differences in parents' KAPs scores based on their characteristics; using an independent student t-test revealed that parents who are working in medical fields have significantly higher knowledge and practice scores (M= 9.1, SD= 2.5, P <.001; M= 4.8, SD= 1.1, P <.001, respectively) than those working in a non-medical field. In addition, parents who are living in rural areas have significantly higher knowledge and attitudes scores (M=9, SD= 2.2, P <.001; M=5.5, SD= 1.0, P <.001, respectively) than those living in urban areas. One-Way ANOVA with Tukey Post Hoc for multiple comparisons test showed that parents older than 40 have significantly lower KAPs scores than younger ones (P <.001, P <.001, P= .001, respectively). Moreover, other relatives who came with children for vaccination have significantly lower knowledge and attitudes scores than parents (P <.001, P <.001, respectively). Married parents significantly have higher knowledge, attitudes, and practice scores (P <.001) than divorced and widowed parents. Furthermore, illiterate parents have lower knowledge and attitudes scores (P <.001) than other parents with school or university educational degrees. However, Table 5 showed the differences in parents' knowledge, attitudes, and practice mean scores based on their demographics. Additional analysis using Pearson's correlation proved that there is a significant positive relationship between knowledge and attitudes (r = .59, P <.001), knowledge and practices (r = .35, P <.001), and attitudes and practices (r = .25, P <.001).
| Variable | Knowledge | Attitudes | Practices | |||
| M(SD) | P | M(SD) | P | M(SD) | P | |
|
Parents' Profession* Medical field Non-medical field |
9.1 (2.5) 8.4 (2.3) |
<.001 |
5.5 (1.0) 5.4 (1.1) |
.099 |
4.8 (1.1) 4.5 (1.1) |
<.001 |
|
Residency* Urban Rural |
8.3 (2.4) 9 (2.2) |
<.001 |
5.3 (1.2) 5.5 (1.0) |
<.001 |
4.7 (1.1) 4.6 (1.1) |
.625 |
|
Age** <18 year 19-40 year > 40 year |
8.8(2.6) 8.8(2.2) 7.1(2.7) |
<.001 |
5.2 (1.3) 5.5 (1.0) 4.9 (1.3) |
<.001 |
4.9 (1.1) 4.6 (1.1) 4.4 (1.0) |
.001 |
|
Relationship** Father Mother Other |
8.5 (2.5) 8.7 (2.3) 6.7 (3.0) |
<.001 |
5.3 (1.1) 5.4 (1.0) 4.6 (1.6) |
<.001 |
4.5 (1.3) 4.6 (1.1) 4.5 (1.2) |
.10 |
|
Marital status** Married Divorced Widowed |
8.8 (2.2) 7.3 (3) 7.0 (2.8) |
<.001 |
5.5 (1.0) 4.7 (1.5) 4.6 (1.5) |
<.001 |
4.6 (1.1) 4.1 (1.3) 4.4 (.97) |
<.001 |
|
Education level** Illiterate School University |
7.4 (3.1) 8.5 (2.5) 8.8 (2.1) |
<.001 |
4.5 (1.6) 5.3 (1.2) 5.5 (.93) |
<.001 |
4.5 (1.3) 4.6 (1.10) 4.6 (1.1) |
.823 |
|
Family income** <300JD 300-600JD 600-1000JD >1000JD |
8.3 (2.8) 8.7 (2.3) 8.8 (2.0) 8.8 (1.8) |
.034 |
5.1 (1.4) 5.5 (1.0) 5.5 (.88) 5.5 (1.1) |
<.001 |
4.7 (1.1) 4.6 (1.1) 4.5 (1.1) 4.5 (1.1) |
.231 |
|
Decision maker** Father Mother Both |
8.4 (2.9) 8.6 (2.5) 8.6 (2.1) |
.70 |
5.1 (1.3) 5.3 (1.1) 5.4 (1.1) |
.002 |
4.8 (1.20 4.6 (1.1) 4.6 (1.1) |
.222 |
|
Governorate** South Middle North |
9.7 (1.4) 7.4 (2.6) 9.2 (1.9) |
<.001 |
5.8 (.54) 4.9 (1.4) 5.7 (.82) |
<.001 |
5.0 (1.1) 4.4 (1.1) 4.6 (1.10 |
<.001 |
|
Settings** Public medical center Public hospital Private clinic Private hospital |
8.6 (2.3) 9.4 (2.1) 9.1 (2.6) 7 (2.3) |
.195 |
5.4 (1.1) 5.5 (1.2) 5.2 (1.5) 3.0 (1.8) |
<.001 |
4.6 (1.1) 4.8 (1.3) 5.0 (.95) 4.2 (.5) |
.553 |
|
Compliance with vaccine* Yes No |
8.5 (2.3) 8.1 (2.7) |
.192 |
5.4 (1.1) 5.2 (1.2) |
.331 |
4.6 (1.1) 4.0 (.97) |
<.001 |
**The mean difference is significant at the .05 level using ANOVA test
3.3. Parents' Compliance with NIP
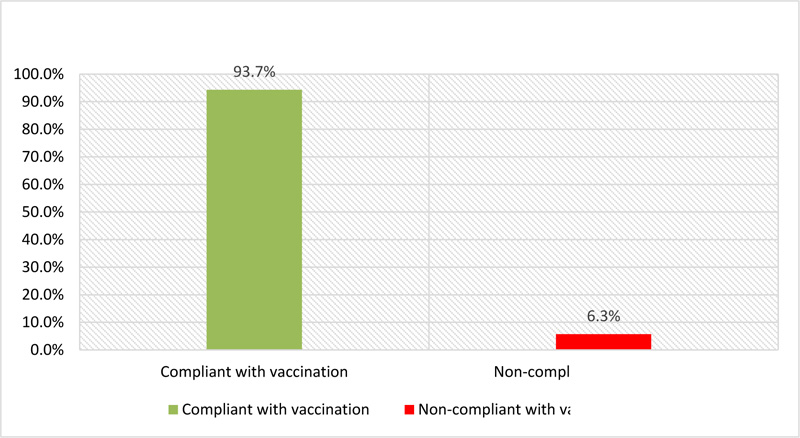
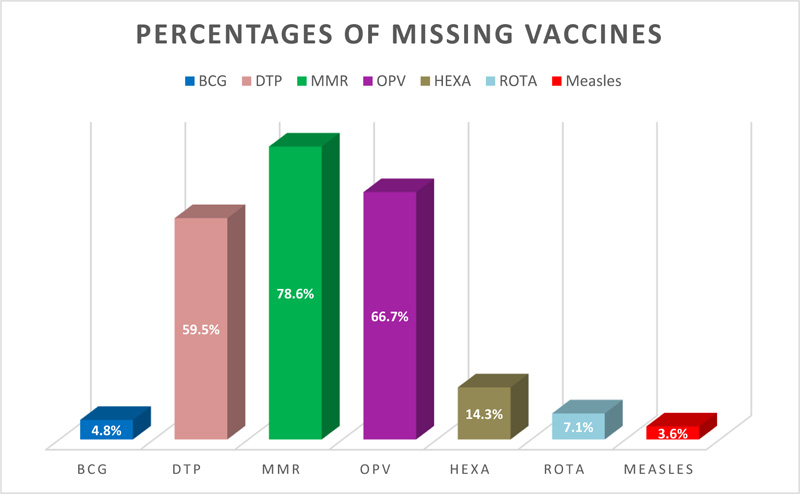
A total of 1340 questionnaires were included in the analysis of parents' compliance with the NIP, while others (137) were excluded due to missing data. However, data proved that 1256 (93.7%) were compliant with the NIP, while 84(6.3%) were not (Fig. 1). Regarding those who were not compliant, results showed that the MMR vaccine was the most common missed vaccine 66 (78.6%), and the least missed vaccine was measles 3 (3.6%); Fig. (2) shows the percentage for each missing vaccine. Regarding the reason for missing vaccination, 51 (60.8%) of the parents reported child health-related reasons such as having a fever 15 (17.9%), runny nose 14 (16.7%), and general sickness 10 (11.9%). Other reported parents-related reasons 26 (31.1%) ‘being busy’ 15 (17.9%) and changing residency 5 (6%). Significantly, data showed that parents who are compliant with vaccination have higher mean practice scores (M=4.6, SD= 1.1, P < .001) than those who are not (M= 4.0, SD= .97. Otherwise, differences in knowledge and attitudes mean scores between these two groups were insignificant (Table 5).
4. DISCUSSION
The current study investigated determinants of parents’ KAPs and compliance with the NIP of their children.
4.1. Parents' KAPs Regarding Vaccination
The majority of parents had adequate knowledge regarding the importance of vaccines to maintain their children’s health. Similar findings were reported by a previous national study [21] and other studies from Arab countries [3, 11]. In Canada, parents have adequate knowledge regarding the rotavirus vaccine [22]. On the other hand, parents had lower to moderate levels of knowledge regarding vaccinations in the studies from Yemen, Iraq, and Malaysia [5, 8, 10]. Scientifically, the adverse reactions of vaccines fall into three general categories: local, systemic, and allergic. The most common types of adverse reactions are local reactions, such as pain, swelling, and redness at the injection site. Allergic reactions may be caused by the antigen of the vaccine itself or some other vaccine component. Systemic adverse reactions are more generalized events and include fever, malaise, muscle pain, headache, loss of appetite, skin rash, and convulsion [23]. In the current study, a significant number of parents did not know about the adverse reactions of vaccines, such as rash and convulsion. According to CDC (2020), rash is a systematic adverse reaction that occurs following receiving live attenuated vaccines. Moreover, convulsion with or without fever, occurring within three days of a dose, is considered a permanent precaution to further doses of pediatric DTaP vaccine. This result suggests that parents of the current study may not pay attention to the seriousness of convulsion as an adverse reaction to DTaP vaccines. Therefore, they may need more education regarding this fact urgently. In the same way, the majority of parents recognized that some vaccines are linked with fever and pain; however, nearly half of them confirmed that skin rash and convulsion are not adverse reactions to vaccines [11]. In another study, more than half of participating parents strongly agreed or agreed that vaccination is associated with adverse reactions [3].
In the current study, more than two-thirds of parents believed that malnutrition, low-grade fever, and diarrhea are vaccination contraindications. According to this misconception, children may be exposed to risk when vaccines are postponed if the child has these conditions. Therefore, parents of the current study may need more information regarding the contraindications of vaccines. Similar findings were reported previously [3, 5, 10].
Regarding attitudes, most parents in the current study hold positive attitudes toward the NIP, and they perceived the importance of vaccination on their children’s health positively. Similar results came from the previous national study [21]. At an international level, parents have positive attitudes toward the rotavirus vaccine [22]. Collectively, parents from Malaysia, Sweden, England, Norway, Poland, and Spain believe that vaccines are crucial for children's health [5, 24].
Parents of the current study had significant concerns about vaccination safety, reflecting public misconception. This result is consistent with the finding that came from different cultures. For example, parents question the safety and necessity of routine childhood immunizations in Arab countries [3, 25]. The belief that vaccines may cause autism was the most prevalent parental concern in a survey conducted in the United States (US) [26]. In other studies, parents reported that their children are vaccinated against diseases that do not exist; however, they were worried about the adverse reaction of vaccines [6, 27]. Moreover, parents from Australia, England, Sweden, and Norway had doubts about MMR as a combined vaccine and seasonal influenza vaccine [24, 28]. These conflicting issues related to vaccine safety seemed to be a global dilemma since it is found in developed as well as developing countries.
Regarding practice, parents of the current study's best practices were reported in terms of their commitment to the NIP and the use of antipyretics to manage fever as an adverse reaction to vaccines. However, they showed better scores on knowledge and attitudes regarding vaccines than practice. An immunization card is the main requirement for children to enter school at six years of age in Jordan. Therefore, this may force parents to be committed to the NIP. Similarly, mothers have also positive attitudes regarding NIP in our country [21] and Saudi Arabia previously [11]. On the other side, findings reported from Iraq showed that more than 40% of children received partial immunization due to the non-compliance of parents with the immunization program [8]. The lowest practice by parents in the current study was in terms of searching for other available vaccines. Similarly, parents hesitated to vaccinate their children with hepatitis and meningitis as additional vaccines in France [27]. Inversely, the majority of parents (81.2%) searched for other vaccines in Saudi Arabia [11].
4.2. Differences between Parents’ KAPs Based on their Demographics
The current study showed differences in KAPs in relation to parents’ demographics. For example, parents working in a medical field have higher knowledge and practice scores than those working in a non-medical field. This result is expected because parents working in the medical field may be more oriented and confident in the scientific knowledge that they gained from their medical study regarding vaccines' safety and efficacy than others.
The other result showed that parents living in rural areas had significantly higher knowledge and attitudes than those living in urban areas. Inversely, a national study showed that people living in urban areas had better knowledge than people in rural areas regarding influenza vaccines [29]. Consistently, there were significant differences in knowledge and attitudes of parents living in the city than those residing outside the town in Saudi Arabia. The same study explained these significant differences in terms of dissimilarity in educational level and the quality of health services provided to people in urban and rural areas [3].
A further result from the current study showed that parents with ages more than 40 years had significantly lower KAPs scores than others. In comparison, being a younger parent was associated with more hesitancy to vaccinate children in Italy [6]. Furthermore, statistically significant differences were found in the mean score of parents’ knowledge with their age in Yemen [10]. On the other side, no significant differences were found in parents’ KAPs regarding vaccines according to age [8]. These contradicted results mandate further studies investigating the association between parents' age and their KAPs toward children’s vaccines.
In the current study, illiterate parents had lower knowledge and attitudes scores than other parents with school or university education degrees. Educated parents may have more likelihood to search for knowledge about children's vaccines than illiterate parents. Previous studies showed contradicting results regarding the association between parents' hesitancy towards vaccination and their level of education. In the same way, nearly 16% of parents in Indonesia hesitated to vaccinate their children because they doubted the vaccines' efficacy and safety. However, parents who have diplomas significantly have a decreased hesitancy [30]. Consistently, a study from the United States showed a negative association between mothers' vaccine hesitancy and their educational levels. However, mothers with higher educational levels (Diploma Degree) reported a higher prevalence of worries regarding the side effect and the number of vaccines [31]. On the other side, other studies reported no significant differences in parents' KAPs in relation to their educational level [8, 10].
In the current study, parents of families with income less than 300JD significantly have lower attitude scores than others. In the same way, high-income families had better knowledge of the influenza vaccine [29]. Similar findings came from Iraq as a significant association between parents’ attitudes and practice, and family income was found [8]. Inconsistently, mothers of low, moderate, and high-income families had similar attitudes regarding the commitment to vaccination schedule [27]. Parents of higher-income families may be able to engage with more health resources, and they also may display greater health literacy than those from low-income families.
There is a significant positive relationship between parents’ knowledge and attitudes, knowledge and practices, and attitudes and practices in the current study. This confirms that parents with adequate knowledge have shown awareness about the importance of vaccination, which resulted in positive attitudes and practice patterns among most of them. Similar findings were reported in the study of Habib and colleagues [11]. Inversely, vaccination delay was reported by about more than one-third of mothers and was shown to be associated significantly with the lower scores on vaccination knowledge and attitude in Jordan previously [21].
4.3. Parents’ Compliance with the NIP
In the current study, the majority of parents were compliant with NIP. Among parents who are not compliant, the MMR vaccine is the most common missed vaccine, while the measles vaccine is the least missed one. Similarly, all parents adhered to the vaccine schedule due to safety and social responsibility issues, but half of them missed the seasonal influenza vaccine [28].
The occurrence of general illness, fever, and a runny nose among children following vaccination is the main child-related reason that made more than half of parents in the current study miss vaccines. Parents-related reasons are being busy and changing residency. Interestingly, parents who are compliant with NIP have better practices than those who are not compliant. Similarly, parents were not compliant with the hepatitis vaccine based on their personal experience [27].
5. LIMITATIONS
The main limitation of this study is the use of a cross-sectional design that examines the associations rather than the causal direction of the relationships. Using a self-administered questionnaire for data collection might generate response biases, and exposing the participants to social bias is another limitation. Though, this issue was possibly reduced by treating the study participants anonymously.
CONCLUSION
The current study results showed that parents had good knowledge, positive attitudes, and good practice on some aspects related to children’s vaccines; however, they had inadequate knowledge regarding the seriousness of the adverse reactions, contraindications, and safety of vaccines. The study results indicate a significant association between parents' work, residency, level of education, age, and income and their KAPs toward children’s vaccines. Therefore, nurses need to implement more educational interventions regarding vaccination safety, contraindications, and other aspects to upgrade parents' knowledge with particular emphasis on less educated, and residents of rural areas. Further qualitative studies are suggested to understand parents' KAPs towards vaccines better.
IMPLICATIONS
This study may provide evidence regarding current parents' KAP regarding their children's vaccines in Jordan. The study has an implication related to practice as nurses, and other health care providers are significant in influencing parents’ KAPs regarding children’s vaccines. They should adequately teach parents about vaccine safety, contraindications, and the harmful effect of non-compliance with vaccine schedules on children's health. Regarding research implications, this study may encourage nurses and other healthcare professionals to conduct more studies regarding children's vaccination in Jordan to provide more evidence-based data in this area to improve parents' KAPs regarding children’s vaccines. On the administrative level, decision-makers should recommend periodic assessments of vaccination rates and caregivers' knowledge, attitudes, practice, and commitment toward vaccination schedules. In addition, their attention should be shifted to gathering the efforts to design vaccination educational programs that target people's misconceptions regarding vaccines to maximize their compliance rate with NIP. Finally, this study may enhance more integrations and emphasize the children's vaccination programs in nursing curricula.
LIST OF ABBREVIATIONS
| KAPs | = Knowledge, Attitudes, and Practices |
| MOH | = Ministry of Health |
| NIP | = National Immunization Program |
| BCG | = Bacillus Calmette-Guerin |
| DTP | = Diphtheria Tetanus, and Pertussis |
| MMR | = Mumps Measles, and Rubella |
| MCHC | = Maternal and Child Health Care |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Approval from the Ethical and Scientific Committee at the School of Nursing at The University of Jordan and the Institutional Review Board (IRB) of the chosen settings (MOH REC 1800117) was obtained before collecting the study’s data.
The parents signed the consent form after reading a cover letter stating the study title, purpose, and participants' rights. Also, participants were told that their participation in the study was voluntary. The participants' identifications were not a requirement; therefore, anonymity was assured. Furthermore, parents were informed that the researchers would review their child’s vaccination record based on the record number they would provide to collect the required data for the study. After obtaining the required ethical approval, a pilot study was conducted to assess the study's feasibility and evaluate the appropriateness of the Arabic version of the questionnaire.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from all participants.
STANDARDS OF REPORTING
STROBE guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
FUNDING
This study was funded by The Deanship of Scientific Research at The University of Jordan.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
ACKNOWLEDGEMENTS
The authors express their appreciation to all Parents who participated in this study. In addition, the authors thank all of the participating healthcare institutions for their cooperation and contributions.

