All published articles of this journal are available on ScienceDirect.

A Cross-validation of the Revised Moral Virtue Scale for Thai Nursing Students: Confirmatory Factor Analysis and Multiple-Group Approach
Abstract
Background:
Ethics must be deemed essential in the nursing profession when becoming a nursing student to raise awareness of the importance and the need for professional development. In evaluating nursing students’ moral behavior, it is essential to have a well-developed instrument that reflects the actual moral behavior of nursing students.
Objectives:
This study aimed to overcome the limitations of the preliminary Moral Virtue Scale for Thai Nursing Students by developing and evaluating the construct validity and reliability of the revised scale.
Methods:
An extensive literature review and the preliminary scale were used to synthesize and develop the moral virtue definition, domains, items, and hypothesized model. The revised scale was tested on 1,000 nursing students from two nursing education institutes. The sample was split into a calibration sample (n = 489) and a validation sample (n = 511) to examine the construct validity and reliability using confirmatory factor analysis and multiple-group analysis.
Results:
Confirmatory factor analysis and a multiple-group approach provided evidence of construct validity and construct reliability. Both calibration and validation groups supported a consistent factor structure. The calibration group satisfied Cronbach’s alpha coefficients of ten domains from 0.75 to 0.87. A full scale was 0.97. In the validation group, Cronbach’s coefficient values ranged from 0.78 to 0.92, and the full scale was 0.98.
Conclusion:
Providing a valid and reliable instrument in this study may benefit nurse educators. The revised scale can potentially measure and monitor Thai nursing students' moral behavior.
1. INTRODUCTION
Moral virtue is behaving concerned with the practical life that is right and good and following society's standards [1, 2]. The nursing profession has principles and codes of ethics for all nurses to conduct accordingly because moral behavior is a crucial element of nursing practice. Nurses can employ moral virtues to guide and promote their moral behavior [3]. Since nurses' duties mainly focus on patients, nursing ethics offer a guideline to help them ensure the safety and high-quality care for the patients [4]. In practice, nurses accept the accountability of caring for clients with a high level of nursing and moral competency for the provided care. Therefore, nurses must behave ethically and provide care that reflects high moral standards [3, 5].
Ethics must be deemed essential in the nursing profession when becoming a nursing student to raise awareness of the importance and the need for professional development. It is necessary to develop students' moral virtues in nursing education programs [4, 6]. As nursing students are involved in academic and clinical environments, they should be committed to learning, accepting, and following the ethical standards of conduct of the profession. Ethics education and ethical-based practice can assist nursing students in providing ethical nursing care and meeting the faculty's expectations regarding moral and professional conduct [6-8]. These can increase the ability of nursing students to reflect ethical knowledge in their practice. After graduation, they become ethical practitioners, which reflects their professional development [9].
In evaluating nursing students' moral behavior, it is essential to have a well-developed instrument that reflects the actual moral behavior of nursing students. The researchers developed a preliminary Moral Virtue Scale for Thai Nursing Students in 2010 [10]. However, the scale had a few limitations regarding the psychometric properties of some indicators of moral virtue. For these reasons, it is necessary to overcome the limitations of the preliminary scale by refining the moral virtue definition and measurement and evaluating the psychometric properties of the revised scale. This research aimed at developing and evaluating the revised instrument's construct validity and reliability tests.
2. LITERATURE REVIEW
Moral virtue focuses on the character and behavior of the person. From an Aristotelian perspective, a person of good character will tend to behave in ways consistent with their character [11]. In the nursing profession, moral virtue is a concern with nurses' professional character and behavior. Good character and behavior of nurses appropriate for duty-based practice can help enhance the client's well-being. A literature review of instruments measuring the moral virtue of nursing students in Thailand and western countries found that several instruments measure nursing students' moral or ethical behavior. Each instrument measures specific perspectives of moral virtue. For instance, Jormsri and Sripusanapan developed the Moral Competence Scale (MCS) for measuring moral competency in nursing practice and tested the psychometric properties in 163 fourth-year nursing students in Thailand. The MCS resulted in eight components and 43 items comprising 1) caring and finding ways for patients to receive happiness and medical care according to their needs (7 items), 2) acceptance of the patient's feelings, needs, and rights toward awareness of the illness and its treatment (5 items), 3) providing the best nursing care and acceptance of one's actions and consequences (4 items), 4) acceptance of one's own mistakes and promoting colleagues to have responsibility for their duties (6 items), 5) wishing for the patient not to suffer and encouraging colleagues to take pride in telling the truth (4 items), 6) proud of acknowledging one's mistakes and appreciating colleagues for doing the right thing (4 items), 7) keeping the promise, adhering to it, and developing care to help patients feel comfortable (8 items), and 8) wishing for patient happiness is based on accepting the patient's needs and condition (5 items). In summary, the MCS has been accepted as a valid and reliable scale for measuring moral competency in nursing practice among Thai nursing students [12]. Perngyai, Chaowalit, Nasae, and Scheider developed the Moral Commitment Scale for baccalaureate nursing students in Thailand (MCS-Thai) and examined its psychometric properties in 809 baccalaureate nursing students. The results revealed that the MCS-Thai contained six factors and 81 items comprising 1) respect for patient privacy and keeping patient information confidential (22 items), 2) respect for patients (25 items), 3) providing care equally to each patient (9 items), 4) causing no harm to patients (12 items), 5) doing good for patients (8 items), and 6) telling the truth to patients and the healthcare team (5 items). Findings supported the MCS-Thai as a valid and reliable instrument for assessing moral commitment in Thai nursing students [13]. Muramatsu, Nakamura, Okada, Katayama, and Ojima developed and validated the Ethical Sensitivity Questionnaire for Nursing Students (ESQ-NS). The sample comprised 525 Japanese nursing students. The results confirmed that the ESQ-NS was composed of three factors and 13 items comprising: 1) respect for individuals (8 items), 2) distributive justice (3 items), and 3) maintaining patients’ confidentiality (2 items). The ESQ-NS, which was developed to evaluate the ethical sensitivity of nursing students, showed good validity and reliability [14].
In order to have an operationalized definition of moral virtue covering every domain suitable for nursing students, the researchers reviewed the related literature, existing research instruments, and prior versions of the Moral Virtue Scale for Thai Nursing Students by using document analysis [10, 12-23]. As documents are controllable, practical, easily accessible, and reliable data sources, document analysis is valuable for acquiring data. Moreover, documents are non-reactive and steady data sources. The researchers can read and reread material several times. Furthermore, the researchers or the research process does not alter documents [24, 25].
The researchers analyzed and synthesized the definition of moral virtue, domains of moral virtue, and indicators of each domain from an extensive literature review. The synthesized definition and domains of moral virtue were used to refine the preliminary scale and guide the development of the revised Moral Virtue Scale for Thai Nursing Students (MVSTNS). In this study, “moral virtue” means behaving in a habitual, routine, and natural way according to moral principles and nursing profession standards. Among the domains of moral virtue (MOV) are: 1) discipline (DIS), 2) responsibility (RES), 3) honesty (HON), 4) patience (PAT), 5) appropriateness (APP), 6) justice (JUS), 7) caring (CAR), 8) cooperation (COO), 9) sacrifice (SAC), and 10) diligence (DIL). “Discipline” demonstrates the behaviors of nursing students that respect rules, regulations, good values, and adherence to traditions of institutions, professions, and society. “Responsibility” reflects the behaviors of nursing students that know, focus, and commit to their duties and accept the consequences of their actions. “Honesty” means the behaviors of nursing students that adhere to the truth, correctness, and goodness, being sincere, keeping secrets and promises, avoiding conflicts of interest, being ashamed, and being afraid to do bad things. “Patience” constitutes the behaviors of nursing students who perform various activities to achieve their goals, are invincible to problems and obstacles, accept and understand their feelings and thoughts, control their emotions and behaviors, and adapt even when faced with difficulties. “Appropriateness” acts on the behaviors of nursing students that show good manners in verbal expressions, gestures, and proper conduct with people, times, occasions, and places. “Justice” represents the behaviors of nursing students that show respect for thought and treat others with equality and fairness in decision-making. “Caring” reflects the behaviors of nursing students that show love, benevolence, wishing others to be happy, respect human dignity, and assist others. “Cooperation” means the behaviors of nursing students that focus on working with others for a shared goal, making good relationships with others, providing assistance, and promoting and supporting the activities/work of others, institutions, professions, and society. “Sacrifice” constitutes the behaviors of nursing students that show the sacrifice of physical power, willpower, wealth, and wisdom for the benefit of others and society. “Diligence” acts on the behaviors of nursing students that express a strong strive for success, devoting both physical and mental strength to oneself, others, and society without being tiresome to achieve better results. Later, the hypothesized measurement model of moral virtue was constructed, as shown in Fig. (1).
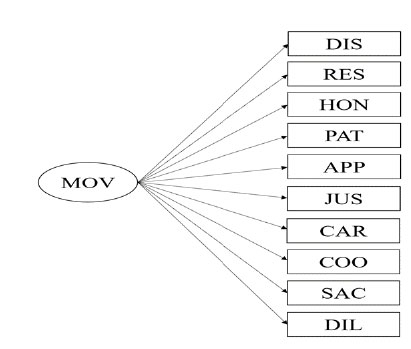
Abbreviations: MOV = Moral virtue; DIS = Discipline; RES = Responsibility; HON = Honesty; PAT = Patience; APP = Appropriateness; JUS = Justice; CAR = Caring; COO = Cooperation; SAC = Sacrifice; DIL = Diligence
3. MATERIALS AND METHODS
3.1. Design
This research was a scale development study. The main objectives were to overcome the limitations of the preliminary Moral Virtue Scale for Thai Nursing Students by refining the moral virtue definition and measurement and evaluating the revised instrument's construct validity and reliability tests.
3.2. Sample and Settings
A total of 1,000 nursing students have been recruited using proportional quota sampling stratified by the institute, one university nursing school, and one nursing college of the Ministry of Public Health and year of study, the first year to the fourth year. Student nurses who enrolled in the 2nd semester of the academic year 2020, could communicate in Thai, and were willing to participate voluntarily in the study, were included based on the proportion of the institute and year of study. There were 489 participants; 93 first-year students, 112 second-year students, 107 third-year students, and 177 fourth-year students from the university nursing school, and there were 511 participants; 154 first-year students, 117 second-year students, 139 third-year students, and 101 fourth-year students from the nursing college of the Ministry of Public Health.
The sample size was calculated using the power analysis for the structural equation model, with an anticipated effect size of 0.65 [10] at a 0.001 probability level and desired statistical power level of 0.80. The number of latent variables was equal to 10, and the number of observed variables was equal to 68. The recommended minimum sample size was approximately 400 participants [26]. Nevertheless, this study employed the multiple-group analysis to test the invariance of factor structure between the calibration and validation groups. A hundred samples per group is a commonly suggested size for minimum recommendations [27]. After all, planning to deal with the violation of multivariate normality requires a larger sample size to increase the robustness of the standard errors and parameter estimates and result in reliable results. A total of 1,000 participants were suggested as an appropriate sample size [28-29].
For confirmatory analysis of a 68-item moral virtue scale developed in this study, the sample was split into two groups. The first group was a calibration sample comprising 489 student nurses from the university nursing school, and the second group was a validation sample comprising 511 student nurses from the Ministry of Public Health nursing college.
3.3. Ethical Consideration and Data Collection
Before collecting data, this study requested approval from the Institutional Review Board, Faculty of Medicine Ramathibodi Hospital, Mahidol University. Also, the researchers made a letter requesting permission to collect data from the director of each institute.
Upon acceptance by the Institutional Review Board and permission for data collection from the two institutes, the researchers liaised with the heads of first-year, second-year, third-year, and fourth-year students in each institute to request an appointment with all students in each year of study. The researchers declared the research objectives, procedures, potential risks and benefits, protection of confidentiality, and the right to withdraw from the study to all participants before signing the consent form. If the participants felt uncomfortable answering questions, they could leave a blank. In addition, the study participants could withdraw from the research project at any time as needed without any consequences. Student nurses willing to participate voluntarily in the study responded to the online questionnaire via smartphone, tablet, laptop, or personal computer when they had free time.
3.4. Instruments/Tools
The MVSTNS was a principal instrument in this study. It is a revised instrument developed by the researchers and is comprised of 68 items in 10 domains: discipline (6 items), such as “I conduct myself according to the institution's rules and regulations”; responsibility (10 items), such as “I have accomplished the tasks that have been assigned to me”; honesty (9 items), such as “I do not copy other people's work”; patience (6 items), such as “I can control my emotions when things do not meet expectations”; appropriateness (5 items), such as “I use my words appropriately for people, times, occasions, and places”; justice (6 items), such as “I treat everyone fairly”; caring (9 items), such as “I can make others feel warm and comfortable”; cooperation (6 items), such as “I cooperate to the best of my ability in group work”; sacrifice (6 items), such as “I offered my assistance to individuals in need without anticipating compensation”; and diligence (5 items), such as “I devote all of my energy to studying and practicing” All items were rated on five-point Likert-type scales with verbal anchors of “very irrelevant” and “very relevant” at points 1 and 5, respectively. The participants were asked to evaluate how each item matched their perceptions. The total score for the revised MVSTNS ranged from 68 to 340, and a higher score indicated higher levels of moral virtue.
Document analysis was performed to define moral virtue, construct domains of moral virtue, define construct domains, and generate items for each domain. The process of document analysis began with searching, recording, and reading the related literature, existing research instruments, and the prior version of the Moral Virtue Scale for Thai Nursing Students [10, 12-23]. Then, the researchers organized information into categories following the predetermined issues using content analysis. Next, the researchers analyzed and synthesized the definition of moral virtue, domains of moral virtue, and indicators of each domain [25]. Finally, ten domains and 72 items were synthesized and generated in the first draft of MVSTNS.
The first draft of MVSTNS was verified for content validity by a panel of three experts, considering whether the items adequately provided the theoretical soundness of moral virtue. The expert panel was composed of two nurse instructors specializing in nursing ethics and an instructor specializing in research methodology. Out of 72 items, 68 items with I-CVIs greater than 0.80 were retained, and four were deleted. The final draft of MVSTNS was comprised of 68 items with an S-CVI/Ave of 1.00 [31, 32]. After that, a pilot study with 50 nurse students (the first to the fourth year) from the university nursing school was conducted for internal consistency reliability testing. It satisfied Cronbach’s alpha coefficients of ten domains from 0.68 to 0.94, and a full scale was 0.98.
3.5. Data Analysis
The researchers performed the psychometric evaluation, including construct validity and construct reliability tests of the final draft of MVSTNS in the calibration and validation groups, using confirmatory factor analysis (CFA). Further-more, the researchers confirmed the structural invariance of the model between the calibration group and validation group using multiple-group analysis.
Before evaluating the psychometric properties of the final draft of MVSTNS, the characteristics of the participants in the calibration and validation groups were analyzed by descriptive statistics, in terms of frequency, percentage, mean, and standard deviation, using the SPSS program. Next, each construct domain's validity with its indicators was examined in the calibration and validation groups. Later, the construct validity of the MVSTNS was tested in both groups separately using the Mplus program. Finally, The structural invariance of the model between the calibration group and validation group was employed using the Mplus program.
The CFA's assumptions were tested, including multivariate normality, linearity, and multicollinearity. The linearity and multicollinearity requirements were met, but the multivariate normality was not achieved. However, as sample sizes grow, multivariate analysis becomes more robust to minor or moderate violations of normality [33]. The maximum likelihood with robust standard errors (MLR) approach requires a large sample size to produce robust standard errors and accurate parameter estimates [27]. There were 1,000 participants in all, which was sufficient for the analyses in this study.
The goodness of fit of each measurement model was evaluated following guidelines for the goodness of fit indices, including 1) insignificant p-value of chi-square statistic, 2) the ratio of the chi-square statistic to the respective degrees of freedom (χ2/df) less than 2, 3) comparative fit index (CFI) greater than 0.96, 4) Tucker-Lewis index (TLI) greater than 0.96, 5) standardized root mean square residual (SRMR) less than 0.05, and 6) root mean square error of approximation (RMSEA) less than 0.07 [27-29]. The statistical significance of indicators was evaluated by t-values that exceeded the critical values of ± 3.29 at the 0.001 significant levels. The construct reliability value of indicators was assessed using the squared multiple correlations (R2) for observed variables with a good recommendation of 0.50 or higher [27, 29].
4. RESULTS
4.1. Sample Characteristics
Most of the study participants for the calibration group were female (94.70%). The median age was 21 years (mean = 20.66; S.D. = 1.28). The mean cumulative grade point average (GPAX) was 3.14 (S.D. = 0.41). The participants were first-year, second-year, third-year, and fourth-year students in the following percentages: 19, 22.90, 21.90, and 36.20, respec-tively. In the same way, most of the study participants for the validation group were female (96.90%). The median age was 20 years (mean = 20.52; S.D. = 1.89). The mean cumulative grade point average (GPAX) was 3.00 (S.D. = 0.34). The participants were first-year, second-year, third-year, and fourth-year students in the following percentages: 30.10, 22.90, 27.20, and 19.80, respectively.
Table 1.
| Measurement Items | Parameter Estimates | ||||
|---|---|---|---|---|---|
| b | S.E. (b) | B | t | R2 | |
| 1. Discipline | 1.00 | <---> | 0.66*** | <---> | 0.44*** |
| 2. Responsibility | 1.69 | 0.10 | 0.78*** | 17.48*** | 0.61*** |
| 3. Honesty | 1.38 | 0.09 | 0.72*** | 15.68*** | 0.52*** |
| 4. Patience | 1.35 | 0.10 | 0.74*** | 14.08*** | 0.54*** |
| 5. Appropriateness | 0.81 | 0.06 | 0.66*** | 14.02*** | 0.44*** |
| 6. Justice | 1.25 | 0.09 | 0.77*** | 14.67*** | 0.59*** |
| 7. Caring | 1.93 | 0.13 | 0.85*** | 15.52*** | 0.73*** |
| 8. Cooperation | 1.48 | 0.09 | 0.85*** | 15.88*** | 0.73*** |
| 9. Sacrifice | 1.71 | 0.13 | 0.71*** | 13.72*** | 0.51*** |
| 10. Diligence | 1.35 | 0.09 | 0.77*** | 14.79*** | 0.59*** |
| χ2 = 15.65; df = 16; p = 0.477; χ2/ df = 0.98; CFI = 1.00; TLI = 1.00 ; SRMR = 0.01; RMSEA = 0.00; 90% CI for RMSEA = 0.00-0.04 | |||||
| Measurement Items | Parameter Estimates | ||||
|---|---|---|---|---|---|
| b | S.E. (b) | B | t | R2 | |
| 1. Discipline | 1.00 | <---> | 0.75*** | <---> | 0.56*** |
| 2. Responsibility | 1.84 | 0.08 | 0.83*** | 24.21*** | 0.69*** |
| 3. Honesty | 1.60 | 0.07 | 0.82*** | 22.69*** | 0.67*** |
| 4. Patience | 1.29 | 0.07 | 0.78*** | 17.71*** | 0.61*** |
| 5. Appropriateness | 1.00 | 0.06 | 0.81*** | 17.61*** | 0.66*** |
| 6. Justice | 1.29 | 0.07 | 0.87*** | 18.82*** | 0.75*** |
| 7. Caring | 1.91 | 0.09 | 0.90*** | 20.60*** | 0.81*** |
| 8. Cooperation | 1.44 | 0.07 | 0.92*** | 21.93*** | 0.85*** |
| 9. Sacrifice | 1.43 | 0.08 | 0.79*** | 17.68*** | 0.62*** |
| 10. Diligence | 1.17 | 0.06 | 0.83*** | 18.15*** | 0.68*** |
| χ2 = 8.02; df = 10; p = 0.627; χ2/ df = 0.80; CFI = 1.00; TLI = 1.00 ; SRMR = 0.01; RMSEA = 0.00; 90% CI for RMSEA = 0.00-0.04 | |||||
4.2. Confirmatory Factor Analysis
The measurement model of moral virtue fits the empirical data, according to the CFA results for the calibration group (χ2 = 15.65; df = 16; p = 0.477; χ2/df = 0.98; CFI = 1.00; TLI = 1.00; SRMR = 0.01; RMSEA = 0.00; 90% CI for RMSEA = 0.00-0.04). Each of the ten indicators displayed significantly standardized factor loadings at p < 0.001. The standardized factor loadings had values between 0.66 and 0.85. Additionally, those indicators' construct reliabilities ranged from moderate to high, with R2 values between 0.44 and 0.73 (Table 1). The CFA results for the validation group also showed that the measurement model of moral virtue fitted the empirical data (χ2 = 8.02; df = 10; p = 0.627; χ2/df = 0.80; CFI = 1.00; TLI = 1.00; SRMR = 0.01; RMSEA = 0.00; 90% CI for RMSEA = 0.00-0.04). All ten indicators showed significantly standardized factor loadings at p < 0.001. The values of standardized factor loadings ranged from 0.75 to 0.92. Besides, the construct reliabilities of those indicators were moderate to high, with the values of R2 ranging from 0.56 to 0.85 (Table 2).
To sum up, the sizes of ten-factor loadings for both groups were statistically significant. In addition, the pattern and magnitude of factor loadings, standard errors, and construct reliabilities were similar. Both groups' most essential indicators of moral virtue were cooperation and caring. The cross-validation results between the calibration and validation groups exhibited that ten indicators could measure moral virtue for nursing students of the two institutes of nursing education. They support the construct validity of the revised MVSTNS.
4.3. Multiple Group Analysis
After conducting separate group CFA to determine the best-fitting measurement model for the calibration and validation groups, both fitted CFA models were combined for structural invariance of the model testing. The researchers conducted three invariance tests using multiple-group CFA: 1) configural invariance test, 2) metric invariance test, and 3) scalar invariance test. In the configural invariance test, most parts of the model were freely estimated in each group except for the number of factors and the relationship pattern between factors and indicators. The results showed that there were no differences between calibration and validation groups (χ2 = 23.67; df = 26; p = 0.595; CFI = 1.00; TLI = 1.00; SRMR = 0.01; RMSEA = 0.00; 90% CI for RMSEA = 0.00-0.03). Hence, these two CFA models could be combined. Later, the metric invariance was tested. All goodness of fit statistics indicated that when the researchers forced the equivalence of factor loadings across two groups, the metric invariance model was consistent with the data (χ2 = 49.51; df = 35; p = 0.053; CFI = 0.99; TLI = 0.99; SRMR = 0.04; RMSEA = 0.03; 90% CI for RMSEA = 0.00-0.05). The equivalence of factor loadings between the two groups indicated that calibration and validation groups could perceive and interpret the revised MVSTNS in the same way. This instrument could measure moral virtue for both groups on the same scale. Next, the scalar invariance test was conducted. All goodness of fit statistics indicated that when the researchers forced he equivalence of factor loadings and item intercepts between the two groups, the scalar invariance model was not consistent with the data (χ2 = 149.56; df = 44; p = 0.000; CFI = 0.98; TLI = 0.97; SRMR = 0.04; RMSEA = 0.07; 90% CI for RMSEA = 0.06-0.08). Lastly, the nested model comparisons were made to confirm the measurement models' invariance. The researchers needed to compare the three nested models sequentially: configural model vs. metric model, metric model vs. scalar model. The chi-square difference test (Δχ2) and change in CFI (ΔCFI) were obtained for each comparison. Even though the chi-square difference test revealed significant results, the CFI change was also used to evaluate invariance in multiple-group CFA. If the change was less than or equal to 0.01 between two nested models, it indicated the model invariance between the two groups [27]. Based on the results, the CFI changes were 0.00 and 0.01. These confirmed the structural equivalence between the calibration and validation groups (Table 3).
As shown above, the revised MVSTNS can be used for both calibration and validation groups based on empirical evidence. The psychometric properties of this instrument might not be changed between the two nursing education institutes.
5. DISCUSSION
The main objectives of this study were to overcome the limitations of the preliminary Moral Virtue Scale for Thai Nursing Students by refining the moral virtue definition and measurement and evaluating the construct validity and reliability of the revised scale. The researchers performed cross-validation to validate ten indicators of moral virtue in two separate groups using confirmatory factor analysis. The results in both groups provided good statistical indices for more applications for Thai student nurses. The factor loading values of the ten indicators were moderate to significant. These reflect the importance of ten indicators for measuring moral virtue in student nurses. According to empirical findings, the revised MVSTNS has strong construct validity [34-37]. The MVSTNS is a revised instrument to measure moral virtue in Thai student nurses. The researcher synthesized the constructed definition of moral virtue and its measurement through an extensive literature review using document analysis. The synthesized definition and domains of moral virtue were used to refine the preliminary scale and guide the development of the revised MVSTNS. These procedures provide a clear operational definition of moral virtue covering every domain suitable for nursing students in the Thai context, enhancing the construct validity and reliability of the revised instrument [35]. The analysis revealed good reliability, indicating the consistency of results across items within a scale. The internal consistency reliability values are high enough in the study samples because the length of the revised scale is suitable for student nurses to fill out. The items of the instrument do not stigmatize the respondents. The researchers also ensure standardization of the online questionnaire by protecting respondents’ concerns about confidentiality. Therefore, the study participants can complete the scale sincerely and honestly, raising instrument reliability [38]. In addition, the present study found no significant institute-based differences in factorial structure. The results revealed that the scalar invariance model was inconsistent with the data, but the comparisons of the three nested models exhibited structural equivalence between the calibration and validation groups. Based on the scalar invariance test, the researchers maintained the equality of factor loadings and item intercepts between the two groups. The results indicated that the item intercepts between the two groups were different. However, item intercept differences between the two groups were not of substantive interest. The structural equivalence between the calibration and validation groups was of interest in this study, supported by the metric invariance test and the nested model comparisons. Thus, this instrument can evaluate student nurses’ moral behavior for both nursing education institutes with the same psychometric properties. The results of this current study exhibited that the construct of the moral virtue of Thai student nurses was proper for validating the revised MVSTNS.
In baccalaureate nursing education, while nursing students recognize the ethical standards of conduct of the nursing profession, some might not perceive immoral or unethical behavior as a problem. Cheating the exams, violating others' rights, stealing others' ideas, plagiarism, misuse of social media, falsifying patients' documents, discussing their patients with others publicly, and recording unmeasured vital signs are examples of immoral conduct [39]. Nursing students who behave unethically can harm their learning in the classroom and clinical learning experiences. These immoral actions exacerbate unprofessional behavior and can significantly affect the quality of care and patients' safety. Therefore, preventing immoral or unethical behavior of student nurses is very crucial. The revised MVSTNS is a well-developed instrument that could be used to evaluate Thai nursing students' actual moral behavior.
| Model | χ2 | df | Δdf | Δχ2 | Δp-value | RMSEA | CFI | ΔCFI |
|---|---|---|---|---|---|---|---|---|
| Configural | 23.67 | 26 | - | - | - | 0.00 | 1.00 | - |
| Metric | 49.51 | 35 | 9 | 25.84 | 0.002 | 0.03 | 1.00 | 0.00 |
| Scalar | 149.56 | 44 | 9 | 100.05 | 0.000 | 0.07 | 0.99 | 0.01 |
CONCLUSION
This study contributes to the nursing ethics literature by revealing a consistent factor structure of moral virtue for Thai nursing students, which was cross-validated on the two samples based on confirmatory factor analysis and a multiple-group approach. The appropriate level of validity and reliability measures of the moral virtue scale developed in this study can be used as a quality tool to measure the moral virtue of Thai student nurses. Finally, this revised scale may also apply to other student nurses with similar Thai cultures.
IMPLICATIONS FOR NURSING EDUCATION
This study highlights the need to evaluate nursing students' moral behavior. Providing a valid and reliable instrument in this study may benefit nurse educators. The revised scale can potentially measure and monitor Thai nursing students' moral behavior. Also, strategies to maintain and promote the good moral behavior of Thai student nurses should be developed for professional development.
LIMITATIONS
Some limitations of this study should be acknowledged. Firstly, the results of this study depend on the participants’ sincerity and honesty. Voluntary participation, anonymity, and confidentiality were warranted to increase the integrity of responses. Secondly, this study investigated the cross-validation of the revised MVSTNS using empirical data. Future research should test the psychometric properties and factor structure stability with student nurses in other countries. Thirdly, the revised MVSTNS is limited to Thai nursing students. Fourthly, the majority of participants in both the calibration and validation groups were female student nurses. Therefore, the results of this study are limited generalizations for male student nurses.
LIST OF ABBREVIATIONS
| MCS-Thai | = Moral Commitment Scale for Thai Baccalaureate Nursing Students |
| MCS | = Moral Competence Scale |
| ESQ-NS | = Ethical Sensitivity Questionnaire for Nursing Students |
| MVSTNS | = Moral Virtue Scale for Thai Nursing Students |
| DIS | = Discipline |
| RES | = Responsibility |
| HON | = Honesty |
| PAT | = Patience |
| APP | = Appropriateness |
| JUS | = Justice |
| CAR | = Caring |
| COO | = Cooperation |
| SAC | = Sacrifice |
| DIL | = Diligence |
| CFA | = Confirmatory Factor Analysis |
ETHICS APPROVAL AND CONSENT TO PARTI-CIPATE
This study was approved by the Institutional Review Board, Faculty of Medicine Ramathibodi Hospital, Mahidol University (COA. MURA2020/551).
HUMAN AND ANIMAL RIGHTS
No animals were used that are the basis of this study. All the human experiments were performed in accordance within the Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Before each participant signed the consent form, the researchers explained the aims, methods, potential risks and benefits, confidentiality protection, and the right to withdraw from the study individually.
STANDARDS OF REPORTING
This study followed STROBE guidelines for reporting the research article.
AVAILABILITY OF DATA AND MATERIALS
The data that support the findings of this study are available from the corresponding author [P.O] on special request.
FUNDING
This study was funded by the Research and Innovation Unit of Ramathibodi School of Nursing, Faculty of Medicine Ramathibodi Hospital, Mahidol University, under project number 001/2020.
CONFLICT OF INTEREST
All the authors declare no conflicts of interest.
ACKNOWLEDGEMENTS
The authors would like to thank the participants for their contribution to this research. Moreover, all the authors would like to acknowledge the support of the Ramathibodi School of Nursing, Faculty of Medicine Ramathibodi Hospital, Mahidol University.

