All published articles of this journal are available on ScienceDirect.

Knowledge and Skill Needs in E-course Training of an Expanded Program for Immunization Staff in Thailand: A Mixed-method Design
Abstract
Background:
This study was conducted to examine essential content needs in E-course training to improve the knowledge and skills of immunization staff members in Thailand.
Methods:
This study used a mixed-method research design. Quantitative methodology was used to study 449 staff members of government care facilities in the Expanded Program on Immunization (EPI). Surveys were conducted by using the perceived needs for immunization training questionnaire. Qualitative methodology employed in-depth interview guidelines on immunization content that were used to interview 14 staff members at EPI. The quantitative data were analyzed by using descriptive statistics and one-way analysis of variance (ANOVA). Interview data were analyzed in content analysis.
Results:
The participants were immunization staff members of three positions: registered nurses, pharmacists and public health technical officers. The participants had different E-course training content needs concerning vaccine-report registration, administering the vaccines and dealing with adverse events following immunization (AEFI) with a statistical significance of .05. This was consistent with the findings from in-depth interviews, which showed staff members had both varying and connected work responsibilities, giving members from all three groups a need for the same basic knowledge pertaining to immunization. In some aspects, staff members required different training content details depending on job descriptions. Public health technical officers were found to require details on vaccine-report registration. Nurses required knowledge dealing with AEFI and administering the vaccines. Pharmacists needed details on the cold-chain system the most.
Conclusion:
Executives at the policy level should specify essential content requiring development for each position in addition to designing training models to meet the needs of EPI staff, enabling access and promoting effective use.
1. INTRODUCTION
Immunization is at the core of severe communicable disease control and prevention in Thailand because immunization or vaccinations suppress the spread of many types of infectious diseases. Therefore, vaccines are of no less importance for the health of an individual than medications. Thailand has been praised by the World Health Organization in providing immunization services as one of thirteen countries worldwide that was successful in developing a system for monitoring access and use of vaccinations for preventing diseases in children [1]. In practice, however, many problems persist. For example, according to an immunization assessment by the Ministry of Public Health’s Disease Prevention Vaccine Division of the Department of Disease Control, primary care units in Thailand’s government sector earned assessment scores of only 63.90 percent consistency with standards, meaning vaccination services remain incomplete according to all immunization standards. When categorized by activity, immunization service delivery was found to have the highest mean score (90.1%), followed by vaccine management and cold chain monitoring, while information system management had the lowest score [2]. The vaccine management problem showed an immunization service that was inconsistent with standards, causing a loss of vaccine efficiency and ineffective immunization services.
Success in developing immunization services in Thailand depends on four main elements: 1) vaccines; 2) budgets; 3) management of production, storage, transportation and service units; and 4) immunization staff or service providers, which is highly important as the main mechanism in working according to achieve goals [3]. Findings from the studies on service knowledge and skills of the Thai EPI staff found most of the staff possessed confidence in their skills but displayed improper practices in vaccine storage and cold-chain system, scheduling immunization appointments and vaccine screening. Furthermore, the staff was found to lack confidence and conducted improper practices in vaccine estimation and dealing with AEFI, causing erroneous vaccine disbursement in data management and registration, lacking procedures to assist patients with abnormal symptoms and providing care for emergency patients who had anaphylaxis. Problems were also found in cold chain system management for vaccine storage and improper vaccination services [4]. Similarly, the findings from research conducted abroad found most EPI staff to lack knowledge and understanding of vaccine estimation and vaccine-report registration due to a lack of proper training on providing vaccination services. Thus, performance has to be monitored and assessed, and training has to continually be provided to enhance knowledge among staff [2, 5]. The data mentioned above reflected inaccurate knowledge, understanding and skills, causing immunization staff to have an insufficient capacity for immunization work.
For these reasons, immunization staff knowledge and skills development is considered essential in effective vaccine management. The development of staff depends on systematic and effective staff methods. Training in essential knowledge and skills to meet work requirements is a major factor in enabling the staff to work effectively and with confidence leading to a high standard of work. Knowledge and skills development, in particular, has significant effects on the development of immunization work competency [6, 7]. However, data from a survey on Immunization Program Evaluation, monitoring and assessment found that 90 percent of the staff received vaccination knowledge from in-service training, while the remaining 10 percent received practical knowledge and skills development from the Disease Prevention Vaccine Division and the National Vaccine Institute [8]. Training on immunization has not been given to all staff members. Furthermore, turnover rates due to transfers or resignations are another major barrier to immunization staff development, causing many new staff members to enter the system each year and creating a threat to developing overall immunization staff capacity. Therefore, a staff training model capable of supporting immunization staff with broad training access and no limits to the number of trainees in each class needs to be developed in accordance with budget allocations.
The immunization service provider development plans of the National Vaccine Institute emphasize lifelong learning. In addition, the Thailand 4.0 policy emphasizes generative learning and innovation. Therefore, the use of technology to create learning innovations is a good option for reducing or eliminating barriers, as well as providing EPI staff members with sufficient knowledge and skills to provide immunization services. E-learning is an effective option allowing participants from various fields to gain more knowledge and understanding as well as enable the application of their knowledge at work [9]. According to Labeau [10], training medical staff online on the topic of hospital infection prevention was able to help medical staff or personnel acquire knowledge and understanding about infection prevention. Therefore, the use of e-learning technology to improve staff is a viable option for replacing previous models.
Another important issue in developing staff knowledge and skills is training course content. According to an evaluation by the “Capacity Building Workshop Program for Expanded Program Immunization Staff” Project, recommendations were provided by trainees from professions such as pharmacists, registered nurses and public health technical officers. Additionally, some topics were considered inappropriate and unnecessary in training, such as vaccine estimation and vaccine-report registration [8]. Similarly, Rutchanagul [11], who studied nurses’ content needs in immunization services, found nurses do not require all the immunization content in the training that is included in the staff development policy of the National Vaccine Institute. This resulted in observations on how models of training content could be developed to improve immunization staff knowledge and skills for training models and content to be consistent with the real needs and requirements of staff members in each profession.
With these issues in mind, the researcher was interested in focusing on E-course training content to improve immunization staff knowledge and skills by using a mixed method research methodology combining quantitative and qualitative research. This study aims to explain and build a clearer understanding of knowledge and skill needs for designing suitable E-course training learning content and educational media for staff in diverse professions. Furthermore, this study will seek data from staff members’ work experience and needs at both the policy and practitioner levels. The findings will provide empirical knowledge for developing integrated knowledge and meeting staff needs at every level. These findings will be important for developing and creating applicable knowledge media, leading to self-improvement and effective immunization work development. In addition, this study will provide evidence-based practice that can serve as policy recommendations for future immunization staff development in Thailand.
2. PURPOSE OF THE STUDY
(1) To study E-course training content needed for improving the knowledge and skills of immunization staff members in the positions of registered nurse, pharmacist and public health technical officer.
(2) To study and compare differences in content needs among the positions of the registered nurse, pharmacist and public health technical officer.
(3) To study E-course training models for improving immunization knowledge and skills.
3. MATERIALS AND METHODS
3.1. Study Design
This study involved the research and development of self-learning models via E-course training by using a mixed method with a convergent triangulation design. This approach makes use of both quantitative data (from a questionnaire survey) and qualitative data (from an in-depth interview). The data were collected separately in a single phase, and results from both the survey and interview were then converged by comparing the overall results obtained. The combination of findings aided in determining accuracy as they provided a complete understanding of E-course training content needs for improving immunization staff knowledge and skills. This study was thus divided into the following phases: In the quantitative method phase, E-course training content needs among immunization staff in each profession were explored to develop an online learning model; and (2) In the qualitative method phase, E-course training content needs were explored from the perspective of immunization agency supervisors or immunization experts by using a qualitative descriptive approach as the research design.
The participants were immunization staff members working in Thailand’s government sector public health care facilities who met the following inclusion criteria: 1. The participant is an immunization staff member directly responsible for administering vaccines or an immunization service provider; 2. The participant worked at a government sector public health care facility. Participants who were temporarily assigned to help with work or as a substitute for staff in specific tasks were excluded.
3.2. Sample Sizes for Quantitative Research
The sample size was determined using Cochran’s formula for calculating sample size when the population is infinite. A sample size of 385 samples was required to achieve a power of 0.95. Because the response rate in postal mail surveys is usually low, the number of samples was increased by 50%. Accordingly, the expected sample size contained a total of 578 participants.
3.2.1. Sampling Method
The researcher randomly selected participants by stratified random sampling. The first strata divided population characteristics into six groups based on regions of Thailand. The researcher performed simple random sampling by drawing lots for two provinces/regions. In the second strata, the researcher randomly selected districts from each province to represent each region using simple random sampling. In the third strata, the researcher conducted random sampling based on service characteristics which were divided into District Public Health Offices, Provincial Health Offices, central hospitals, general hospitals, community hospitals and Sub-district Health Promotion Hospitals in each province. In Strata 4, data were collected from the staff in randomly selected agencies. Each region had a sample size of 96 participants. When consideration was given to the ratios of healthcare workers in Thailand, nurses were found to have the highest ratio. Therefore, in this study, registered nurses made up 50 percent of the participants, public health technical officers made up 30 percent and pharmacists made up 20 percent.
3.3. Sample Sizes for Qualitative Research
Fourteen healthcare providers involved in immunization services from the six regions were selected through purposive sampling for the in-depth interviews.
3.4. Research Instruments
Research instruments consisting of the demographic questionnaire and the perceived needs for immunization training questionnaire were employed for the quantitative phase. Guidelines for the in-depth interviews were used in the qualitative phase.
The demographic questionnaire contained data on gender, age, level of education, occupation, agency characteristics, experience in work related to immunization and experience of immunization training.
The perceived need for an immunization training questionnaire was developed by Rutchanagul [11] to develop an immunization learning mobile application. In this study, the researcher reviewed the literature concerning content within the framework of practical courses for immunization staff prepared by the National Vaccine Institute to provide guidelines for developing questions. Questions were divided into seven content sections consisting of the following: 1. Basic knowledge pertaining to immunization; 2. Vaccine-preventable infectious diseases; 3. Vaccine estimation; 4. Vaccine-report registration; 5. Vaccine storage and cold-chain system; 6. Making preparations and administering the vaccines; and 7. Dealing with adverse events following immunization. Responses to this questionnaire were rated on a 5-point Likert scale containing the following: 5 (Highest Need), 4 (High Need), 3 (Low Need), 2 (Least Need) and 1 (No Need). The questionnaire had a total of 65 questions. High scores meant a high need for learning media content on that topic. The researcher had five qualified experts with immunization expertise to test the content validity of the perceived needs for immunization training questionnaire and in-depth interview questions. In addition, the researcher piloted the instruments with 30 EPI staff withqualifications similar to the sample in order to evaluate the reliability of the instrument. The perceived needs for immunization training questionnaire had an excellent content validity index for scale (CVI was 1.00). The result of internal consistency using Cronbach’s alpha was 0.92.
The in-depth interview guide in immunization knowledge development needs to consist of open-ended opinion questions concerning content for each profession needing knowledge and skills development or focus points to create capacity in the staff. The interview questions were tested and verified by five experts. The pre-testing was conducted with two EPI staff workers to test their understanding of the questions.
3.5. Ethical Considerations
This study received approval from the Human Research Ethics Committee of Thammasat University (Science), Thailand (COA No. 072/2563). Before data collection, the researcher explained the rights of participants in the study. If the participants agreed to participate in this study, they were instructed to sign the consent form for research participation and send it back by post along with the questionnaire. Furthermore, data would be identified, aggregated and disclosed in the form of an overall conclusion of the findings without disclosure of the names of the participants or place of work. Their personal information was kept confidential and secure in the researcher’s locked office.
3.6. Quantitative Data Collection and Analysis
(1) The researcher coordinated with research assistants in randomly selecting areas to explain research project information and design. Research assistants coordinated with supervisors in the area to ask for permission to collect data from participants for the study.
(2) The researcher and research assistants sent questionnaires to the participants by electronic mail and post at the participants’ convenience. The researcher and research assistants attached the project information sheet and the informed consent form allowing the participant to respond in two weeks. If the researcher did not receive a response, the researcher coordinated with research assistants to randomly select other participants in the area to have the desired number of questionnaires returned.
(3) The researcher checked the completeness of 470 sets of returned questionnaires. 21 sets of questionnaires were found to have incomplete responses for more than 20 percent of all questions. Therefore, the researcher excluded incomplete questionnaires, leaving 449 sets of questionnaires for use in data analysis.
The researcher analyzed the collected data using the SPSS for Windows as follows:
(1) Descriptive statistics were used to analyze demographic data and content needs to determine mean scores and standard deviation. Data were analyzed overall by content section and by area.
(2) The content needs of immunization workers in each profession were compared. Differences between staff members who were registered nurses, pharmacists and public health technical officers were analyzed using a one-way analysis of variance (ANOVA).
3.7. Qualitative Data Collection and Analysis
(1) The researcher selected two supervisors of immunization service agencies or immunization experts from the randomly selected provinces for in-depth interviews.
(2) The researcher coordinated with the participants to explain research information, ask for their cooperation in the study and explain the rights protection of the sample.
(3) The researcher conducted in-depth interviews individually. The in-depth interviews were conducted directly or via the Microsoft Teams application, according to the convenience of the participants. The researcher spent 40-60 minutes conducting each interview. The researcher asked the participants to make audio recordings and had research assistants take field notes describing the prevailing atmosphere of the interviews.
(4) The researcher collected data from 14 participants until the researcher achieved a data-saturation point.
The researcher transcribed data verbatim and performed content analysis to study E-course training content needs for immunization staff knowledge and skills development. During analysis, two researchers transcribed and read the dialogues several times to generate codes and categories. In this study, content analysis by ATLAS.ti 8.0 (computer-assisted qualitative data analysis software) was used for data analysis in order to organize coded data. The transcript summary was reviewed by three participants to ensure that the description accurately reflected their perspectives.
Quantitative data from ANOVA was compared to qualitative data from content analysis and linked for connection or consistency to summarize immunization content in E-course training needed by the participants.
4. RESULTS
4.1. Results from Quantitative Data Analysis
According to the findings, most of the participants who responded to questionnaires (449 subjects) were female (83.5%). Most were at the bachelor’s degree level (81.5%) with a mean age of 39.21 years (SD. 9.5). Most were younger than 30 years (26.28%), married (55.0%) and worked in the role of a professional nurse (52.6%). Most of the sample (46.1%) worked at sub-district health promotion hospitals with immunization work experience at an average of 8.5 years (S.D. 8.6 years). A majority of the participants (31.40%) had performed this work for 1-5 years.
Most of the participants (49.0%) had experience with immunization training. In the area of immunization knowledge and skills development methods, most of the participants were found to have used lectures (47.44%), followed by instructions from supervisors or colleagues (38.08%) and self-learning (34.08%).
Furthermore, almost all the participants (92.9%) were found to have other responsibilities outside of immunization, most of which (25.61%) were clinical responsibilities for patients at non-communicable disease (NCD) clinics and in home health care (Table 1).
| Demographic Characteristics | Number (n) | Mean (SD.) | Statistic (P-Value) | ||
|---|---|---|---|---|---|
| Registered Nurse (n=236) | Pharmacist (n=66) | Public Health Technical Officer (n=147) |
|||
|
Gender Male |
15 | 11 | 44 | χ2=39.4 (.00) | |
| Female Do not care to respond |
220 1 |
55 0 |
100 3 |
||
|
Age (Years) ≤ 30 |
49 | 25 | 43 | 39.21 (SD. 9.5) | F = 12.59 (.00) |
| 30-40 | 51 | 20 | 42 | ||
| 41-50 | 93 | 18 | 37 | ||
| 51-60 Do not care to respond |
31 12 |
2 1 |
18 7 |
||
| Educational Level | χ2=15.4 | ||||
| Bachelor’s degree | 199 | 49 | 117 | (.004) | |
| Master’s degree | 36 | 11 | 21 | ||
| Others Do not care to respond |
0 1 |
5 1 |
5 4 |
||
|
Marital
Status Single Married Divorced/Widowed Do not care to respond |
66 141 27 2 |
33 28 4 1 |
57 77 10 3 |
χ2=14.2 (.007) | |
| Characteristics of Healthcare Service | χ2=128.2 | ||||
| Public Health Center Sub-District Health Promoting Hospitals |
33 110 |
7 2 |
5 94 |
(.000) | |
| Community Hospital | 50 | 41 | 18 | ||
| General Hospital | 14 | 15 | 5 | ||
| Others Do not care to respond |
28 1 |
1 0 |
21 4 |
||
| Duration of Work Experience in Immunization Service (Years) | 8.5 (SD. 8.6) | F =2.878 (.057) | |||
| ≤1 | 33 | 10 | 28 | ||
| 1-5 | 75 | 23 | 43 | ||
| 6-10 | 54 | 12 | 29 | ||
| > 10 Do not care to respond |
72 2 |
21 0 |
44 3 |
||
|
Having
Experience in Immunization Training No Yes Do not care to respond |
115 114 7 |
36 30 0 |
69 76 2 |
χ2=.88 (.642) |
|
|
Taking on
Additional Responsibilities No Yes Do not care to respond |
8 218 10 |
9 57 0 |
4 141 2 |
χ2=.13.37 (.001) |
|
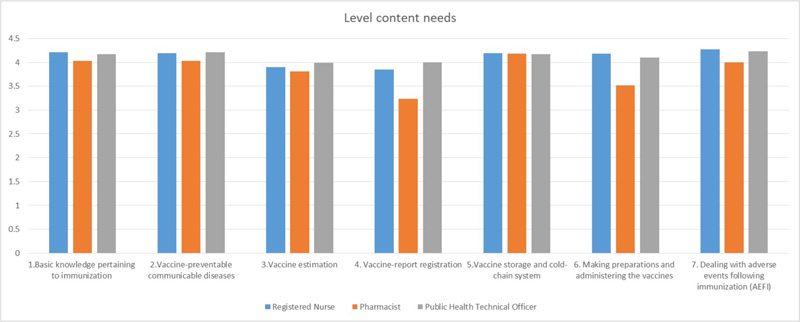
According to Table 2, the participants who were immunization staff members in the three professions of the registered nurse, pharmacist and public health technical officer were found to have different E-course training content needs on the topics of vaccine-report registration, making preparations and administering the vaccines and dealing with AEFI with statistical significance of .05.
According to Fig. (1), the content section on vaccine-report registration showed public health technical officers to have the greatest need for content while pharmacists had the least need for content. On the topic of making preparations and administering the vaccines, registered nurses had the highest need for content while pharmacists had the least need for content.
4.2. Results from Qualitative Data Analysis
The participants for this part of the research came from 14 EPI staff members in immunization services from the six regions of Thailand. 8 (57.1%) of the participants were female, and 6 (42.9%) were male. The participants’ ages ranged from 31 to 55 years, with a mean age of 40.93 years (SD=6.7). The majority (28.6%) of the participants worked within Health Provincial Office. Seventy-eight percent of the participants had completed their master's degree level education. Within this group of participants, 7 people (50%) were working as public health technical officers, 3 (21.4%) were pharmacists. The average length of time spent working in the area of immunization was 7.3 years (SD. = 5.2), and the participants’ duration of work ranged from 1-21 years.
Two major themes were identified as the findings of this study. All themes are supported by quotations from the interviews of participants. The details are shown in Table 3.
| Content | Level Content Needs: Mean (SD) | Df | F | Ρ-value | ||
|---|---|---|---|---|---|---|
| Registered Nurse (n=236) | Pharmacist (n=66) |
Public Health Technical Officer (n=147) |
||||
| 1.Basic knowledge pertaining to immunization | 4.25 (0.62) | 4.06 (0.75) | 4.21 (0.61) | (2,446) | 2.225 | .109 |
| 2.Vaccine-preventable communicable diseases | 4.25 (0.62) | 4.06 (0.75) | 4.21 (0.62) | (2,446) | 2.935 | .054 |
| 3.Vaccine estimation | 3.96 (0.76) | 3.83 (0.92) | 4.08 (0.70) | (2,446) | 2.504 | .083 |
| 4. Vaccine-report registration | 3.94 (0.81) | 3.31 (1.14) | 4.08 (0.74) | (2,446) | 19.486 | .000* |
| 5.Vaccine storage and cold-chain system | 4.25 (0.69) | 4.21 (0.92) | 4.28 (0.65) | (2,446) | 0.194 | .824 |
| 6. Making preparations and administering the vaccines | 4.24 (0.68) | 3.61 (1.02) | 4.22 (0.67) | (2,446) | 20.157 | .000* |
| 7. Dealing with adverse events following immunization (AEFI) | 4.33 (0.65) | 4.04 (0.98) | 4.33 (0.63) | (2,446) | 5.032 | .007* |
| Major Themes: 1. Knowledge Content Must be Suitable and Consistent with the Rules, Duties and Functions of Each Profession | |
| Sub-themes | Exemplar Quotes |
| 1.1 Basic Knowledge Required by Every Profession in Immunization | - It isnot that a person has to know everything. A person who works with vaccines needs to know many things, but not every detail, as in epidemiological work. Some professionals think this is unrelated to vaccines. We have to communicate to build an understanding that vaccination work is associated with several topics. We have to get them into why they have to know and what they have to do after they know, because they do not work alone. They have to know things across their fields of study like epidemiological concepts in immunization, basic knowledge pertaining to immunization, vaccine-preventable diseases, definitions and types of vaccines, each type of vaccine used in immunization plans for children and adults, including target group designations for calculations in administering vaccines.” |
| 1.2 Essential Knowledge for Each Profession | - “I want pharmacists to have knowledge about managing vaccine stocks, accurate estimates and VMI without guessing. Problems were also found about cold chain breakdowns caused by improper practices and human error.” - “For pharmacists, the standout issue is vaccine supply management. They don’t directly administer vaccines…pharmacists might give advice on proper storage or how to prevent vaccines from degrading prematurely because the people who store them might not be as well-trained as they are.” - “Mainly, public health technical officers oversee plans, projects, and governance like someone who takes care of a system, directs the system or looks at data systematically. In data systems, sometimes, the technicians are not good with IT systems, but the technical officers might help with this because they are already good with data management in many areas.” - “Nurses need to have the same knowledge as public health technical officers except for vaccination knowledge, which is unnecessary for public health technical officers because they don’t administer vaccines. Nurses need to know about vaccine storage, vaccine disbursement, AEFI and immunization knowledge. Public health technical officers should know about making stock cards, packing data, data system structures, recording programs and the details of each program.” - “Nurses should know what vaccinations are essential for patients of any age, restrictions, potential S/Es and how to manage if S/Es occur. They need to know what to do in the service unit and how to refer patients. They need to know about proper vaccination skills, vaccine management, how to carry vaccines, how to maintain the cold chain system and how to use vaccines after taking vaccines offsite without resorting only to disposal. Some nurses have the wrong concept with the understanding that they have to make the vaccine cold first by covering it with a lot of ice…” |
| 1.3 More Knowledge regarding Immunization Policies | - “Every profession should have a foundation on an understanding of national and global vaccination policies such as measles eradication, so they willknow why they have to do this and recognize the importance of their role.” - “Even vaccinators need more knowledge on some points such as policy or project plan views so that they can see how what they do corresponds with the big picture like in a disease eradication project, which is a big picture. You can see that they did well and correctly when vaccinating individuals. However, in the broader view, they might not have looked deeply.” |
| Major themes: 2. Models and Methods for Developing Immunization Staff at Basic and Advanced Levels Based on Work Experience | |
| Sub-themes | Exemplar quotes |
| 2.1 Basic Knowledge and Skills Should be Included in Training for All Staff When Beginning Immunization Work | - “At the basic level, everyone should at least pass this course. The model can be online training or by any channel. At the basic level, it should be at least provide general knowledge about vaccines, providing vaccination services, vaccine tables, including maintaining cold chain storage and monitoring AEFI.” - “I think someone who will do EPI work should at least have basic training before work. It’s good to at least lay out a foundation for people who will do EPI work…………Basic knowledge and skills like properly vaccinating each person consistent with standard requirements.” |
| 2.2 Intermediate Knowledge and Skills Should be Provided after 3 Years of Work to Review Knowledge and Gain Knowledge and Skills in More Complex Practices | - “If they have E-learning and part of the training upon entry to work and then have training that focuses on practice, this will shorten the training time. Pharmacists need a short course of about one day on vaccine management, maintaining vaccine stocks, knowing each vaccine, care, storage, use, limitations and prohibitions for vaccines including cold chain systems and management of cold chain breakdowns along with knowledge about AEFI.” - “There might be practical skill training in the short term. An annual refresher course for people who worked for about three years at a high level that is separate from the basic course.” |
| 2.3 Advanced Knowledge and Skills Are Suitable for Vaccination Supervisor to Train Staff and Plan Work Systems | - “If it’s to be advanced training, it should be about specific programs or plans such as disease eradication. This might be a specific topic for someone who is at an advanced level. Or maybe an advanced level shouldn’t be limited only to vaccines but to EPI workers. Maybe vaccination response to disease outbreaks, disease investigations or topics that need some practicing for plans or analyses or research should be an advanced level?” - “For someone who already does EPI work, there should be something advanced and possibly more advanced training and development available. I think we can look at plan management or care at the area level.” |
5. DISCUSSION
Good immunization services that meet standards need an adequately trained workforce with relevant work skills for roles and duties. Staff training programs without sufficient quality were one of the main causes of suboptimal immunization program performance, making training interventions important mechanisms for improving immunization staff knowledge, skills and competencies [5, 12]. Therefore, staff training programs were highly important for suitability and consistency with necessary work skills [13, 14].
Under EPI contexts, immunization staff in the EPI of Thailand had three groups of staff members holding positions nurses, public health technical officers and pharmacists. Each group was responsible for different but connected work. Pharmacists stored and disbursed vaccines, registered nurses vaccinated patients, and public health technical officers dealt with AEFI, disease investigations and vaccine-report registration. Due to differences in roles, duties and responsibilities, each group of staff members had different views concerning necessary immunization knowledge and skills development. For example, public health technical officers needed more knowledge and skill content than other professions on the topic of vaccine estimation and vaccine-report registration, registered nurses needed more knowledge and skills content on vaccine preparation and administering vaccines, and pharmacists needed more knowledge and skills content on the topics of vaccines and the cold-chain system in order to support the roles, duties and responsibilities of each profession.
Based on the quantitative and qualitative findings in this study, the staff members of all three professional groups (registered nurses, pharmacists and public health technical officers) should receive the same basic knowledge and skills development on the following topics: 1. Basic knowledge pertaining to immunization; 2. Vaccine-preventable infectious diseases; 3. Vaccine storage and cold-chain system; and 4. Dealing with adverse events following immunization. In the meantime, content on certain topics such as vaccine-report registration making preparations and administering the vaccines should contain different knowledge details based on job characteristics. This was consistent with the findings of a study conducted by Arogundade [15] on the training needs assessment of health workers and pre-service tutors, which found that courses in the EPI did not meet staff needs because the staff needed the training to improve knowledge and skills pertaining to real work or duties and responsibilities. Furthermore, training content that every staff member must understand accurately should be clear on the topics of basic immunization concepts, data management and cold chain management [16]. Therefore, training course content for EPI staff must be consistent and suitable for duties and responsibilities.
EPI training course content should be divided into two parts consisting of Part 1 – Necessary Content or Basic Knowledge Required for All Staff and Part 2 Knowledge Content of Responsibilities. This is consistent with the WHO concept which specified immunization competency domains in two parts consisting of: 1. Foundational competencies such as (a) management and leadership and (b) vaccine-preventable diseases and programs; and 2. Technical competencies on (a) effective communication on matters related to EPI, (b) monitoring, evaluation and data use, (c) vaccine service delivery and (d) vaccine supplies and logistics [17]. Therefore, immunization content in E-course training should consist of: 1. Foundational immunization knowledge such as vaccine-preventable diseases, vaccines, cold chain management and the handling of adverse vaccine events and 2.Technical knowledge (knowledge required to perform a specific role or task) such as EPI documentation (estimating EPI targets, calculating coverage), administering vaccines, cold chain monitoring, and supplies and logistics.
Furthermore, the findings from this study revealed training courses for improving staff knowledge and skills should be divided into the following three levels: basic, intermediate and advanced, depending on work experience. Basic knowledge and skills development should be included in training for all staff members regardless of the profession when beginning immunization work as it requires basic knowledge on the topics of immunization policy, epidemiological concepts, basic immunization knowledge, diseases that can be prevented by vaccines, each type of vaccine used in immunization plans for children and adults including new vaccines, target group designation and vaccine coverage. Intermediate knowledge and skills development should consist of knowledge reviews and more complex training. For example, nurses should have training focused on the topic of administering vaccines, while pharmacists should focus on vaccine storage and cold-chain system. Public health technical officers should have training focused on vaccine-report registration. Advanced knowledge and skills development should be suitable for educator staff members that educate and plan work systems vital to training content preparations which must be suitable for trainee experience levels in order to enable trainees to use knowledge from training in practice [18-21]. Currently, many countries have developed EPI training courses to have quality and effective immunization performance based on standards. However, problems were found, and training courses may not have met all staff members needs. For example, in a study conducted by Carrico [19], almost 50 percent of the sample determined training in immunization programs to be insufficient for real work, and gaps remained between knowledge and implementation in practice. Therefore, immunization programs need to be developed to be specific to responsibilities and consistent with key performance indicators of workers with experience at different levels. Staff experience was, therefore, another major factor that should be considered when designing EPI training courses to input details and determine the scope of content and knowledge on each issue to be consistent with staff experience to close gaps between vaccination theory and practice.
CONCLUSION
Immunization staff knowledge and skills development should be suitable for staff member roles and duties at each level in order to provide the participants with the necessary knowledge to reduce work problems and mistakes, leading to the achievement of immunization work standards. Therefore, workers at the policy level should specify the necessary content and skills. Specifically, they should describe in concrete terms those areas that are in need of improvement in each profession. Models tailored for diverse personnel with flexibility and suitability for individual staff characteristics should be developed.
IMPLICATIONS FOR NURSING PRACTICE
Nurses are expected to have practical management skills for making preparations and administering the vaccines, as well as a competency in vaccine storage and the cold-chain system. The immunization-training programs have focused on the levels of experience thus far obtained in order to design learning content and educational media for continuing the training and monitoring of personnel, and to support a system of supervision for the immunization workforce.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by The Ethical Review Sub-Committee Board for Human Research Involving Sciences, Thammasat University, Thailand, No. 3, (COA No. 074/2563).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from all participants.
STANDARDS OF REPORTING
COREQ guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
The data that support the findings of this study are available on request from the corresponding author [P.R].
FUNDING
This study was supported by National Vaccine Institute (NVI) [3/2563].
CONFLICT OF INTEREST
The authors declare no conflict of interest financial or otherwise.
ACKNOWLEDGEMENTS
The researchers wish to thank to all participants who given their useful information and National Vaccine Institute for providing funds of this study.

