All published articles of this journal are available on ScienceDirect.

Changes in sleeping habits during the pubertal years; A descriptive study conducted in Jordan
Abstract
Background:
There is limited information about changes in sleeping habits during the pubertal years of development among adolescents in Jordan.
Objective:
This study examined sleeping habits at the onset and end of puberty.
Methods:
This study utilized data from a nationwide survey in Jordan.
Participants: Sleeping habits were obtained from 3,661 adolescents aged 11(onset of puberty) and 15 years (end of puberty) and their mothers using a self-reported questionnaire. The number of hours slept and bedtimes and wake-up times on both school and non-school days were examined.
Results:
On school days, 60% of 11-year-old and 34% of 15-year-old adolescents slept between 8:00-10:00 pm. On school days, the 11-year-old adolescent group reported sleeping significantly longer than the 15-year-old adolescent group, and the proportions of adolescents who met the minimal recommended sleeping hours were 64% and 54%, respectively. Sleeping hours were long for both groups attending government schools; for the 15-year-old adolescent group, sleeping hours varied with family income and maternal education. In the case of both groups, on non-school days sleeping hours varied with gender, family income, and type of school.
Conclusion:
At the end of pubertal years, adolescent sleeping habits differ significantly from those of adolescents at the onset of puberty. On school days, insufficient sleep is much evident in the case of both 11 and 15-year-old adolescent groups, but more pronounced in the latter. Nursing initiatives to address poor sleeping habits among adolescents are warranted, given their efficacy in promoting healthy growth and development within this age group.
1. INTRODUCTION
Adolescents represent 21.5% [1] of Jordan’s population. Adolescence is considered a bridge between childhood and adulthood that constitutes a critical stage in human growth and development. Healthy behaviors adopted during childhood and adolescence work to promote normal growth and development. The technological revolution of the last two decades that ushered in smartphones and computer games has dramatically altered adolescent lifestyles, impacting healthy behaviors, including consuming nutritious food, exercising regularly, and sleeping at least 8 hours daily. On the global stage, sleep deficits represent a public health concern, given that in many countries, 30 to 70% of all adolescents experience poor sleep habits [2, 3], and many adolescents fail to obtain the recommended sleeping hours [4].
Normally, sleep occupies one-third of an adolescents’ day. Its duration, quality, depth, and timing constitute the determinants of sleep health [5]. Adequate sleep is pivotal to achieving optimal human growth and development and essential to the health and well-being of adolescents, affecting their physical health, academic performance, and emotional regulation [6, 7]. Poor sleep is linked to physical health problems such as headaches and obesity [8, 9], anxiety, depression [8, 10], risky behaviors [11], and poor academic performance [8, 12]. All this underscores the need to learn more about adolescent sleep.
Adolescent sleeping habits or patterns,e.g., bedtimes, wake-up times, and duration, vary across cultures [2, 3, 13-15]. And they are also informed by sociodemographic differences [16]. Studies conducted in several countries show that older vis-à-vis younger adolescents retire later and receive less sleep on school days while sleeping longer on non-school days [2, 15, 17]. In addition, male adolescents retire later than female adolescents [4, 13, 17, 18]. Across many countries, poor sleep is more common within lower socioeconomic strata [3, 13, 19].
Most of the literature on the health behaviors of Jordanian adolescents focuses on diet, physical activities, and substance abuse, with little attention given to sleep [20, 21]. Even when this phenomenon represents the focal point of a study, its context is limited. For example, Haddad et al. examined only sleep duration among 13-year-old Jordanian adolescents while failing to account for how school and non-school days and bedtimes and wake-up times, among other factors, affect this phenomenon [22].
According to the American Academy of Pediatrics [23], adolescence is sometimes divided into three stages: early (11-14 years of age), middle (15-17 years of age), and late (18-21 years of age). During the early stage, the major physical change is the onset of puberty, which affect all aspects of adolescent life, including sleep. Puberty ends during the middle stage of adolescence. Thus, the current study focuses on adolescents’ sleeping habits at the onset of puberty (11 years old) and the end of puberty years (15 years old). Both school and non-school-day sleep habits are examined, in addition to variations in sleeping hours linked to sociodemographic variables, including gender, school type, family size and income, and maternal education and employment. Understanding changes to sleep habits during these stages is crucial to designing nursing health promotion programs aimed at enhancing healthy sleep habits and patterns during this critical period of physical and mental development.
The data used in this study are obtained using a nationwide, cross-sectional survey conducted from March 2015 to June 2016. The current nationwide survey aimed to evaluate sleeping habits, among adolescents at two developmental points, namely which are the onset and end of puberty. The aim of this study is 1) to present those survey findings that are related to the school and non-school-day sleeping habits of both adolescents at the onset of puberty and adolescents at the end of puberty stages, and 2) to examine whether there are differences in their respective sleeping habits.
2. METHODS
Given that more than half of Jordan’s population resides in the central region of the country, a proportional sampling protocol was used to obtain a representative sample. According to population distribution, around 60% of the sample was obtained from the central region of the country, 30% from the north region, and 10% from the south region. All students in grade five (aged 11 years) and in grade ten (aged 15 years), along with mothers, were eligible to participate in the study. Students with chronic diseases were excluded to eliminate the possibility that their illness might impact their sleeping habits, as were mothers who were illiterate or had a mental illness.
Twenty-six primary and secondary schools with an enrollment of ≥ 500 students were randomly selected from the Ministry of Education database for government and private schools. From each of these schools, two grade-five and two grade-ten classes were randomly selected. Data were collected from the students on the first day of school, which in Jordan is a Sunday, using a self-reporting questionnaire. The survey consisted of two parts: the first focused on adolescent sleeping habits; the second featured demographic questions relating to the students’ families to be completed at home by their mothers and returned to the school staff.
2.1. Ethical Considerations
The study protocols were approved by two Institutional Research Board committees located at a government university and the Ministry of Education, respectively. Upon approval, letters of invitation were mailed to the participating mothers. The letters contained detailed information about the purpose of the study, protocols, the rights of participants, and the measures to be taken to ensure confidentiality. The students were required to provide verbal consent; the parents were required to sign consent forms for their children and themselves. Participation in the study was voluntary, and the participants were free to withdraw at any time without consequences. The study protocols involved no identified risks to the participants.
2.2. Study Outcome Measurements
A self-report questionnaire aimed at assessing school and non-school day sleeping habits among the participating students was developed by drawing on the relevant sleep literature. The face and content validity of the sleeping habits questions were approved by five experts in community and pediatric health. The Cronbach’s alpha for the sleeping habits questions was found to be 0.803.
2.2.1. Sleeping Habits
Sleeping habits were assessed based on adolescent bedtimes and wake-up times. The participating students were asked to provide their usual bedtimes and wake-up times on both school and non-school days. The estimated average number of sleeping hours for both days was then calculated. For this study, minutes were converted into decimals, for example, 09:15 was expressed as 9.25 and 09:30 as 9.50. In referring to the National Sleep Foundation and The American Academy of Sleep Medicine, the proportions of adolescents who met the minimum recommended sleeping hours, i.e., nine hours for the 11-year-old adolescents’ group and at least eight hours for the 15-year-old adolescent group [5, 24] were examined.
2.2.2. Sociodemographic Variables
Information about participating students, including age, gender, family size, whether living with one or both parents, school type (government/private) and location of residence, was gathered. In addition, data related to the maternal level of education and employment status as well as family income were obtained from the mothers.
2.3. Data Analysis
All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) for Windows, Version 25, with a standard alpha level ≤ 0.05 to determine statistical significance. Descriptive analyses employing frequencies, means, and standard deviations were used to describe the sleeping habits of the participants. The independent t-test and analysis of variance (ANOVA) tests were used to examine differences in adolescent sleeping hours on both school and non-school days. To manage missing values among variables, the exclude cases pairwise option in the SPSS was selected that excludes only participants if they are missing data required for a specific analysis.
3. RESULTS
For this study, 4,400 students were invited to participate in the survey. The response rate reached 89%, and only 129 students were excluded due to chronic diseases. Only questionnaires with complete information regarding adolescent sleep habits were utilized in this report. The final sample was 3,661 students; of these, 46.6% were 11-year-old and 53.4% were 15-year-old adolescents. Around 60% of mothers in the study completed the second part of the questionnaire. Table 1 shows the participants’ demographic characteristics.
A slightly higher proportion of male students made up the sample, with 53% and 53.4% at the onset of puberty and end of puberty stages of development, respectively. The average age was 10.81 years (SD=0.36) for adolescents at the onset of puberty and 15.82 years (SD=0.42) for their adolescent counterparts at the end of puberty. Most of the students attended government schools. More than half resided in the middle region of the country and reported living in families of six or fewer members. And almost all lived with both parents. To allow for further analysis, we divided the students into two categories based on family size: six or fewer family members, i.e., the average and below-average family size, and more than six family members, i.e., the above-average family size. Most of the mothers comprising this sample were housewives, and more than half had a primary or secondary school education. Around 65.9% and 58.1% of mothers of the onset of puberty group and end of puberty group, respectively, reported an average family income of 500 JD ($704.00 US) or less.
|
Onset of Puberty Stage (N=1706) |
End of Puberty Stage (N=1955) |
|||||||
| 95% CI | 95% CI | |||||||
| f (%)* | Total N | Lower bound | Upper bound | f (%) | Total N | Lower bound | Upper bound | |
| Age (mean (SD)) | 10.81(.36) | 15.82(.42) | ||||||
| Gender | 1706 | 1955 | ||||||
| Male | 904(53%) | .51 | .55 | 1044(53.4%) | .51 | .55 | ||
| Female | 802 (47%) | .45 | .49 | 911(46.6%) | .45 | .49 | ||
| School type | 1706 | 1955 | ||||||
| Governmental | 1278(74.9%) | .73 | .77 | 1544 (79%) | .77 | .81 | ||
| Private | 428 (25.1%) | .23 | .27 | 411 (21%) | .19 | .23 | ||
| Family size | 1702 | 1955 | ||||||
| Five and Below | 951(55.9%) | .53 | .58 | 963(49.3%) | .47 | .51 | ||
| Above Five | 751(44.1%) | .42 | .47 | 992(50.7%) | .49 | .53 | ||
| Living with both parents | 1698 | 1946 | ||||||
| Yes | 1616(95.2%) | .94 | .96 | 1814(93.2%) | .92 | .94 | ||
| No | 82(4.8%) | .04 | .06 | 132 (6.8%) | .06 | .08 | ||
| Mother’s education | 1271 | 1033 | ||||||
| Elementary/Secondary | 761(59.9%) | .57 | .63 | 583(56.4%) | .53 | .59 | ||
| College/University | 510(40.1%) | .37 | .43 | 450 (43.6%) | .41 | .47 | ||
| Family Income** | 1245 | 1018 | ||||||
| 300JD ≥ | 346(27.8%) | .25 | .30 | 226(22.2%) | .20 | .25 | ||
| 301-500JD | 474(38.1%) | .35 | .41 | 365(35.9%) | .33 | .39 | ||
| 500 < | 425(34.1%) | .32 | .37 | 427(41.9%) | .39 | .45 | ||
| Mother’s Employments | 1244 | 1012 | ||||||
| Housewife | 998(80.2%) | .78 | .82 | 848(83.8%) | .81 | .86 | ||
| Employed | 246(19.8%) | .18 | .22 | 164(16.2%) | .14 | .19 | ||
| Onset of Puberty Stage (n=1706) | End of Puberty Stage (n=1955) | ||||
| f (%)* | f (%) | ||||
| School days Sleeping Time | |||||
| 6:00pm-8:00 pm | 305 (18.2%) | 33(1.7%) | |||
| 8:01pm-10:00 pm | 1009 (60.1%) | 663 (34%) | |||
| 10:01pm-12:00 pm | 312 (18.6%) | 919 (47.1%) | |||
| 12:01-2:00 am | 46 (2.7%) | 229 (11.7%) | |||
| After 2:00 am | 8 (0.5%) | 107 (5.5%) | |||
| School days Wake-up time | |||||
| 4:00 am-5:30 am | 127 (7.6%) | 127(6.7%) | |||
| 5:31 am- 6:30 am | 713 (42.6 %) | 572(30.2%) | |||
| 6:31 am- 7:30 am | 780 (46.6%) | 1056(55.7%) | |||
| 7:31 am- 8:30 am | 53 (3.2 %) | 142(7.5%) | |||
| School days Sleep Duration (mean (SD) | 8.88(1.38) N=1663 | 7.68(1.39) N=1871 | |||
| Meet Recommended sleeping hours | 1069 (64.3%) | 1015 (54.2%) | |||
| Non-School days Sleeping time | |||||
| 6:00pm-8:00 pm | 36 (2.2%) | 11 (0.6%) | |||
| 8:010pm-10:00 pm | 303 (18.1%) | 87 (4.5%) | |||
| 10:01pm-12:00 pm | 702 (42%) | 665 (34%) | |||
| 12:01-2:00 am | 415 (24.8%) | 707 (36.2%) | |||
| After 2:00 am | 216 (13%) | 484 (24.7%) | |||
| Non-School Days Wake-up time | |||||
| 4:00 am-6:30 am | 105(6.3%) | 50(2.5%) | |||
| 6:31 am- 8:30 am | 437(26.3%) | 216(11.1%) | |||
| 8:31 am- 10:30 am | 685(41.3%) | 837(42.8%) | |||
| 10:31 am- 12:30 pm | 302(18.2%) | 582(29.8%) | |||
| After 12:31 pm | 130(7.8%) | 269(13.8%) | |||
| Non-school day Sleep Duration (mean (SD) | 9.45(2.03) N=1647 | 9.35(1.7) N=1828 | |||
| Meet Recommended sleeping hours | 1139 (69.2%) | 1570 (85.9%) | |||
| Sleeping parameters differences between school days and non-school days | |||||
| Sleeping time (mean (SD) | 2.44(1.93) | N=1655 | 2.02(1.54) | N=1810 | |
3.1. Sleeping Habits
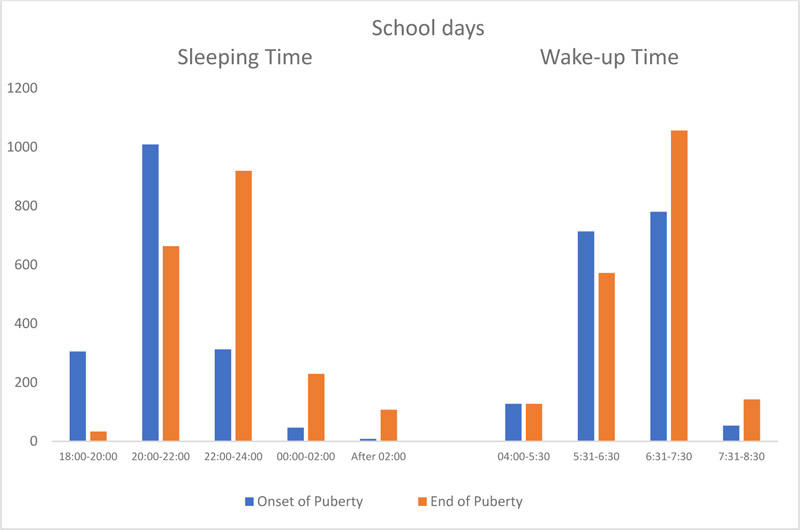
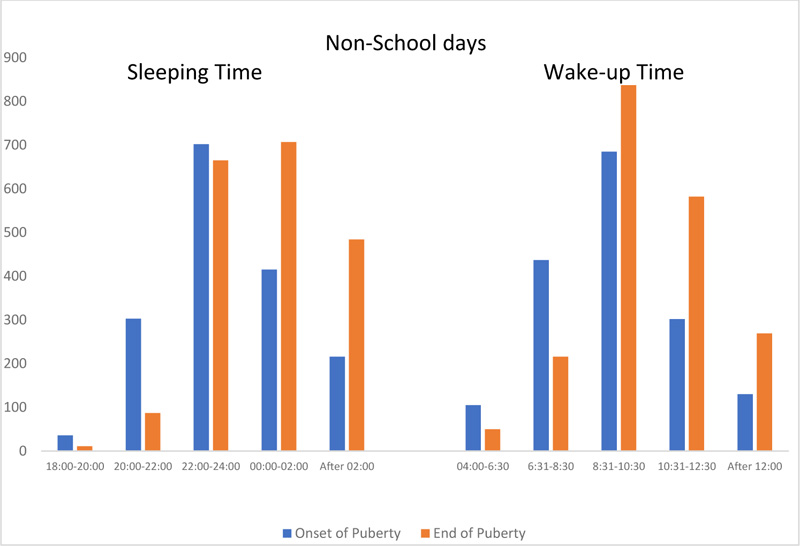
Table 2 shows that on school days, approximately 60% of the 11-year-old adolescents and 34% of the 15-year-old adolescents in the sample retire between 20:00 and 22:00 and that on non-school days these proportions fall to 18% and 4.5%, respectively, because the adolescents report retiring later on those days. In addition, the proportion of the 15-year-old adolescents that retire after 22:00 on school days (64.3%) is three folds greater than that of the 11-year-old adolescents (21.8%). On non-school days, these proportions skyrocket to 94.9% and 79.8%, respectively. The bedtime differences (social jetlag) between school and non-school days for adolescents in both developmental stages were found to be 2-2.5 hours.
Given that in Jordan, the school day starts between 7:30 and 8:00 am, the majority of both the 11-year-old adolescents (89.2%) and 15-year-old-adolescent students (85.9%) awaken between 5:30 and 7:30 am, and, therefore, the average sleeping duration on school days is 8.88 and 7.68 hours, respectively. As Table 2 shows, wake-up times on non-school days are considerably later as more than 25% of the 11-year-old adolescents and more than 33% of the 15-year-old adolescents awaken after 10:30. The later non-school day wake-up times increase the duration of sleeping time by about 0.5 hours for the 11-year-old adolescents and 1.5 hours for the 15-year-old adolescents compared to sleeping hours on school days.
The proportion of 11-year-old adolescents meeting the minimum recommended sleeping hours (9 hours) on school days and non-school days were 64.3% and 69.2%, respectively, while for 15-year-old adolescents, the proportions meeting the minimum sleeping hours (8 hours) were 54.2% and 85.9%, respectively.
3.2. Differences in Sleeping Hours based on Developmental Stages
Based on independent t-test analysis, on school days the 15-year-old adolescents slept significantly fewer hours than their 11-year-old counterparts (t=25.85, p < .0001). However, while on non-school days there was no significant difference in sleeping hours between the two groups, (t=1.61, p = .108) the latter slept longer.
3.3. Variations in Sleeping hours based on Demographics Variables
Separate analyses based on demographic variables were conducted to examine variations between the two groups in sleeping hours on both school and non-school days.
3.3.1. School Days
As Table 3 shows, independent t-test analysis revealed that both the 11 and 15-year-old adolescent groups attending government schools slept significantly longer than their private school counterparts. Additional analyses using independent t-tests and ANOVA analysis based on demographic variables, including gender, single-parent or intact families, family income and size, place of residence, and maternal demographics, revealed no variations in sleeping hours for the 11-year-old adolescents group. However, variations in sleeping hours were evidenced among the 15-year-old adolescents. Maternal level of education is linked to 15-year-old adolescent sleeping hours; those adolescents whose mothers had less education (elementary or secondary school) slept significantly more than those whose mothers had college or university degrees. In addition, ANOVA post-hoc analysis showed that 15-year-old adolescents from families with an income greater than 500 JD slept significantly fewer hours than those from lower-income families.
3.3.2. Non-School Days
As shown in Table 4, the independent t-test revealed a significant difference in sleeping hours between male and female adolescents, with the former sleeping less than the latter. This difference was evident at both the onset of puberty (11-year-old adolescents) and the end of puberty (15-year-old adolescents) stages of development. Further independent t-test and ANOVA analyses based on the type of school, family income, maternal demographics and place of the residence revealed variations in sleeping hours. Thus, for example, on non-school days, both the 11-year-old adolescents and 15-year-old adolescents attending government schools slept longer than their private school counterparts. Moreover, students at either stage of development who were from families with incomes of 300 JD or less slept significantly longer than their higher family income counterparts.
| Demographic Variables | Onset of Puberty Stage | End of Puberty Stage | ||||||||
| Category | Subcategory | N | mean | t/F* | P | N | mean | t/F* | P | |
| Sleeping hours | Gender | Male | 882 | 8.83 | 1.84 | 0.07 | 978 | 7.66 | 0.64 | 0.52 |
| Female | 781 | 8.95 | 893 | 7.70 | ||||||
| Type of School | Governmental | 1216 | 9.00 | 5.72 | 0.000 | 1454 | 7.77 | 6.14 | 0.000 | |
| Private | 447 | 8.58 | 417 | 7.34 | ||||||
| Living with both parents | Yes | 1577 | 8.88 | 0.18 | 0.86 | 1743 | 7.68 | 0.26 | 0.80 | |
| No | 81 | 8.85 | 123 | 7.71 | ||||||
| Family size | Average and below | 928 | 8.94 | 2.00 | 0.05 | 925 | 7.72 | 1.28 | .202 | |
| Above the Average | 734 | 8.81 | 946 | 7.64 | ||||||
| Mother’s Employments | Housewife | 970 | 8.94 | 1.04 | 0.300 | 810 | 7.85 | 0.91 | 0.365 | |
| Employed | 241 | 8.84 | 156 | 7.74 | ||||||
| Mother’s Education | Elementary/Secondary | 740 | 8.97 | 1.397 | 0.163 | 552 | 7.91 | 2.307 | 0.021 | |
| College/University | 496 | 8.86 | 432 | 7.71 | ||||||
| Family Income | 300JD and less | 336 | 8.94 | 2.035 | 0.131 | 209 | 8.03 | 7.654 | 0.001 | |
| 301-500JD | 460 | 8.99 | 353 | 7.94 | ||||||
| More than 500JD | 414 | 8.81 | 412 | 7.64 | ||||||
| Demographic Variables | Onset of Puberty Stage | End of Puberty Stage | ||||||||
| Category | Subcategory | N | mean | t/F* | P | N | mean | t/F* | P | |
| Sleeping hours | Gender | Male | 867 | 9.23 | 4.74 | 0.000 | 949 | 9.15 | 5.21 | 0.000 |
| Female | 780 | 9.70 | 879 | 9.56 | ||||||
| Type of School | Governmental | 1207 | 9.56 | 3.56 | 0.000 | 1418 | 9.40 | 2.72 | 0.007 | |
| Private | 440 | 9.16 | 410 | 9.16 | ||||||
| Living with both parents | Yes | 1561 | 9.44 | 0.52 | 0.607 | 1702 | 9.34 | 0.70 | 0.488 | |
| No | 81 | 9.56 | 121 | 9.47 | ||||||
| Family size | Average and below | 925 | 9.47 | .36 | 0.722 | 917 | 9.38 | .89 | .376 | |
| Above the Average | 721 | 9.43 | 911 | 9.31 | ||||||
| Mother’s Employments | Housewife | 964 | 9.52 | .67 | 0.502 | 799 | 9.43 | 0.68 | 0.506 | |
| Employed | 238 | 9.44 | 154 | 9.53 | ||||||
| Mother’s Education | Elementary/Secondary | 735 | 9.53 | .62 | 0.532 | 543 | 9.50 | 1.50 | 0.133 | |
| College/University | 493 | 9.46 | 428 | 9.34 | ||||||
| Family Income | 300JD or less | 328 | 9.75 | 3.26 | 0.039 | 209 | 9.64 | 3.66 | 0.026 | |
| 301-500JD | 459 | 9.40 | 347 | 9.49 | ||||||
| More than 500JD | 415 | 9.47 | 403 | 9.27 | ||||||
4. DISCUSSION
The current study examined the sleep habits of a sample consisting of a group of children at the onset of puberty and another group at the end of puberty stages. The sleep habits assessed included school and non-school day bedtimes, wake-up times and sleep duration. On school days, most of the 11-year-old adolescent (onset of puberty) group retired to bed at 20:00-22:00, whereas most of the 15-year-old adolescent (end of puberty) group retired after 22:00. On non-school days most of the 11-year-old adolescent group retired after 22:00, while most of the 15-year-old adolescent group retired after midnight. The discrepancy between school and non-school-day sleep (social jetlag) is prevalent among adolescents [25] and is most pronounced among the end of puberty group, which is consistent with the existing literature [2, 4, 16]. For both groups, social jetlag exceeded 2 hours, which is consistent with the findings of Gariepy et al. [16] and Saxvig et al. [4]. What the current study contributes to the literature is the finding that social jetlag is greater among 11-year-old adolescents than 15-year-old adolescents. One reason is that on school days the latter retire later than the former. Another possibility is that on non-school days the former group has more flexible bedtimes.
Sleep duration ranged from 8.88 to 7.68 hours on school days and 9.45 to 9.35 hours on non-school days for the 11-year-old adolescent and 15-year-old adolescent groups, respectively. These findings are consistent with BaHamman [26], who reports that 10-year-old children sleep an average of 8.37 hours on weekdays. Late bedtimes and very late wake-up times on non-school days allow adolescents to sleep longer, a pattern followed by both the adolescents at the onset and the end of puberty groups, albeit older adolescents experienced an even more pronounced shift in sleeping patterns, indicating that sleep regimens vary significantly with age [2, 15]. These findings reveal the operation of circadian rhythms whereby the adolescent tendency to remain awake well into the evening increases with age [27]. This tendency may be further heightened by smartphones that allow easy access to social media. A national cross-sectional survey in Norway revealed that electronic media usage in bed was prevalent among adolescents who were evening circadian type [28]. It is also possible that the greater social obligations and homework assignments that come with adolescents’ work to further delay bedtimes.
The current study used the American Academy of Sleep Medicine [24] criterion for sufficient sleep at both the developmental stages examined here. According to this criterion, the minimum sleeping hours for 11-year-old adolescents is nine hours and for 15-year-old adolescents is eight hours. On average the hours of school-day sleep reported in the current study are sufficient for the onset of puberty group but marginally less so in the case of the end of puberty. Specifically, the proportion of participants at both developmental stages who had sufficient school-day sleep hours is low compared to some countries, e.g., Norway (84.8%) [4] and Belgium (86.3%), but high compared to others, e.g., Poland (32%) [16]. However, on non-school days percentage of sufficient sleep hours is lower than in other countries, e.g., Greece (79.2%) and Belgium (92.4%) [16]. Our study clearly shows a significant decline in total school-day sleeping hours as adolescents age.
Gender differences in sleep duration on non-school days were noted among adolescents at both developmental stages. Male adolescents slept fewer hours than their female counterparts. Similar findings were found among adolescents in Slovenia where girls were found to sleep about 34 minutes longer than boys during non-school days [16]. Gender differences regarding sleeping patterns were also reported among Norwegian adolescents, e.g., boys reported later sleeping time on both school and non-school days than girls [4]. In Jordan it is acceptable for boys to stay up late outside the home on both school and non-school days, albeit this arrangement is more flexible in the case of non-school days.
This study found that adolescents at both developmental stages who attend government schools sleep longer on both school and non-school days than their private school counterparts. Although in both school systems classes begin at approximately the same time, i.e., between 7:45 and 8:00, private school adolescent students put in longer school hours owing to the greater number of subjects in the curriculum. This translates into additional homework, which may result in less sleep. According to the sleep literature, there exists an inverse relationship between homework assignments and hours of sleep [29].
Differences were found in adolescent sleeping hours based on demographic variables, including family income and level of maternal education. Adolescents with better-educated mothers slept less on school days, but this finding is not true for the 11-year-old adolescents, a finding supported by earlier studies [30]. And while some studies reported findings suggesting that adolescents with well-educated mothers slept longer [31], the age of the participants varied from 11-13 years. The speculation behind this finding is that well-educated mothers are more aware that secondary students receive more homework assignments and are thus more inclined to encourage their adolescent children to study longer hours resulting in less sleep.
In this sample, family income was a minor determinant of adolescent sleeping hours; between school and non-school days. Those 15-year-old adolescents whose families were relatively middle-to-high-income earners slept fewer hours on school days. At the same time, both the 11 and 15-year-old adolescents who reported low family incomes slept longer hours on non-school days. These findings are not supported by earlier studies that suggest that, for adolescents, lower socioeconomic status is associated with shorter sleep periods [3, 19]. On the other hand, findings from Gariepy et al. [16], based on surveys conducted in European and North American countries, are in line with ours. The current results may be explained by the tendency on the part of higher-income families to own more electronic entertainment devices that lead adolescents to stay up later on non-school days. Alternatively, 15-year-old adolescents from relatively affluent families are likely to have better-educated parents who encourage them to study longer hours.
Study findings highlight a public health concern pertaining to adolescents sleeping habits that necessitate intuitive interventions to promote healthy sleep. School nurses are in a pivotal position to initiate interventions encouraging healthy sleep habits taking into consideration developmental differences between the onset and end of puberty stages. Adolescents would benefit from sleep education programs regarding sleep health and sleep-promoting behaviors. Such programs were found to be successful in improving adolescents’ knowledge of sleep and sleep-promoting behaviors (e.g., total sleep time and, bedtime on both school and non-school nights) [32]. Knowledge about the recommended sleeping hours across adolescence years and the importance of consistent bedtime and wake-up time on school days and non-school days should be highlighted. Knowledge about possible health consequences of insufficient sleep and social jetlag would render healthy sleeping habits among adolescents. Special emphasis should be placed on male adolescents from high-income families as they showed more need for sleep education in the current study.
STRENGTHS AND LIMITATIONS
The main strengths of this study are threefold: 1) it is based on a nationwide survey, 2) the sample size is large, and 3) examine sleeping habits on school days and non-school days separately. Also, the study examined changes in sleeping habits at the onset and end of puberty stages of development, and something never studied in depth in a national context. In addition, we used standard questions to gather information on sleep and wake-up times on school and non-school days, which ensured the validity of the data. In addition, sleep quality (sufficient sleep) was assessed using the most recent evidence-based international guidelines about the recommended minimum hours of sleep for adolescents at the onset of puberty and the end of puberty. These strengths have the potential to provide us with a deep understanding of adolescent sleeping habits while increasing the external validity of the study findings. In addition, the current study contributes significantly to the sleep literature focusing on sociodemographic differences in sleeping habits at the onset and end of puberty stages of development. Regarding limitations, the data were obtained using a self-report questionnaire that may lack the precision of more objective methods, e.g., actigraphy [33, 34]. However, there is evidence to suggest a high level of correlation between self-report and actigraphy data [35]. Other factors may influence adolescents sleep, including such as dinner time, screen time and physical activity which were not within the scope of this study. Also, the current study did not include an assessment of the circadian typology a variable that many influence adolescents sleeping habits. Thus, the study could not address the possible interactions between pubertal stages, circadian typology and sleeping habits. Future studies are encouraged to investigate the influence of these factors on adolescents sleep during puberty. The cross-sectional design represents another limitation as this research design does not allow cause-effect conclusions. Lastly, our data were obtained from schools attended only by adolescents, which might limit the study’s generalizability.
CONCLUSION
This study shows that self-reported sleeping habits vary between adolescents at the onset of puberty (11-year-old group) and those who are at the end of this developmental stage (15- year-old group), albeit more so on school days vis-à-vis non-school days. Both groups had less than recommended sleeping hours, and this is more prevalent among 15-year-old adolescents. Sociodemographic variables i.e., school type, gender, family income and maternal education were linked to the number of hours of sleep among adolescents. Nursing health promotion interventions are required to address poor sleeping habits at both the onset and end of pubertal years of development
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The protocol for the research project has been approved by the Ethics Committee at Jordan University of Science and Technology (ref/493/2014) and permission from the Ministry of Education in Jordan.
HUMAN AND ANIMAL RIGHTS
No animals were used for studies that are the basis of this research. All the humans used were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was sought from parents and children.
STANDARDS OF REPORTING
STROBE guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
The data that support the findings of this study are available from the corresponding author [R.A], upon reasonable request.
FUNDING
The study was funded by the Deanship of Academic Research at Jordan University of Science and Technology for support (grant No: 20150032).
CONFLICT OF INTEREST
The author declares no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The author would like to thank the study participants; without them, the study could not have come to a successful conclusion. In addition, acknowledgment goes to the Deanship of Academic Research at Jordan University of Science and Technology for support.

