All published articles of this journal are available on ScienceDirect.

Effect of Urogenital Infection Educational Program on Women Knowledge and Practices
Authors Info & Affiliations
Abstract
Background:
Urogenital infection is generally regarded as a silent epidemic. It is one of the major public health problems among women that causes a considerable proportion of gynecological morbidity and maternal mortality in developing countries.
Aim:
The aim of this study is to evaluate the effect of an educational program on women’s knowledge and practices about urogenital infection.
Methods:
A quasi-experimental research design was utilized in this study and was implemented at El Hadaka Maternity and Children’s Hospital (MCH) in Fayoum, Egypt. A purposive sample consisting of 50 women with ages ranging from 30 to 45 years old was considered for this study.
Two tools were used to conduct this study: a structured interview questionnaire consisting of the respondents’ demographic characteristics, knowledge, and practices regarding urogenital infection and a scale that aimed to assess their lifestyle.
Results:
The results revealed that 96% of the women have unsatisfactory knowledge about urogenital infection during the pre-intervention stage, 94% of them have satisfactory knowledge post-intervention, and 90% of them have satisfactory knowledge at follow-up, with a highly statistically significant difference at p-value < 0.01. The results also showed that 82% of the respondents have unsatisfactory practices at pre-intervention, 96% have satisfactory practices at post-intervention, and 98% of them have satisfactory practices at follow-up, with a highly statistically significant difference at p-value < 0.01.
Conclusion:
There was a significant improvement in women's knowledge and practices related to urogenital infection post-intervention and at follow-up with a p-value < 0.01. Likewise, a high positive correlation between total lifestyle, level of knowledge, and practices was noted during the pretest with a p-value < 0.01.
There is a need to provide different educational programs regarding knowledge and self-care practices for women with urogenital infection in different women's care settings.
1. INTRODUCTION
Genitourinary infections may arise by hematogenous dissemination or as an ascending infection, usually because of instrumentation, urinary catheterization, or surgery. These infections include cystitis, pyelonephritis, micro abscess, perinephric abscess, vaginitis, and vaginitis abscess. Genitourinary infections affect the bladder, urethra, vagina, and infection of the uterus [1] and occur mainly among women and girls owing to the shortness of their urethras and (closer) its proximity to the rectum, making it easier for the bacteria to enter the genitourinary tract. Poor hygiene was identified as the main risk factor for such infections [2]. Patients experience symptoms like pain or burning sensation while urinating, frequent urination, feeling the need to urinate despite having an empty bladder, bloody urine, pressure or cramping in the groin or lower abdomen, fever, itching, and irritation in the vagina and vulva, redness and swelling of the vulva, vaginal pain and soreness, vaginal rash, thick white odor-free vaginal discharge, and watery vagina discharge [3].
Annually, it is estimated that one billion women around the world suffer from non-sexually transmitted urogenital infections, including bacterial vaginitis, yeast vaginitis, and urinary tract infection (UTI). Although most patients respond to antimicrobial treatment, the recurrence rate is high and is associated with side effects. Urogenital infections are the most common type of bacterial infection in women, affecting at least 20% of women [4], but seniors may experience different and more severe symptoms than younger adults like agitation, mental confusion, and sudden changes in behavior. When left untreated, it can cause serious problems, including permanent kidney damage and sepsis, a generalized and potentially life-threatening infection [5]. This condition can cause major medical problems for women such as yeast vaginitis, bacterial vaginitis, and urinary tract infection. Although antimicrobial therapy is generally effective in eradicating these infections, there is still a high incidence of recurrence. The patient’s quality of life is affected, and many women become frustrated by the cycle of repeated antimicrobial agents, as its effectiveness is diminished due to increased microbial resistance [6].
Health education is one of the key components of primary health care and is a significant part of a nurse's job in building patients’ knowledge, understanding, and preparedness for self-management. The patients’ knowledge and understanding of their condition empower them to improve their health status. In fact, patients are more likely to engage in interventions that may increase their chances of positive outcomes when involved in their care. The nurses’ close interaction with patients in any setting has placed them in a strategic position to implement such interventions to impart knowledge about urogenital infection, recommended treatment, risky behavior change, and even preventive measures of such infections [7]. This vital educational role can help patients gain an in-depth understanding of urogenital infection, treatment regimen, measures to adopt healthy lifestyle practices, thereby preventing further complications. Improving the women’s knowledge of how these infections develop can greatly affect their practices toward its prevention, thereby reducing their chances of acquiring the infection [8].
1.1. Significance of the Study
Urogenital infection (U.I) in women, although widespread, has been virtually ignored. It is estimated that one-third of all women will experience U.I in their lifetimes. Its prevalence in the general population of women between the ages of 18 and 50 years is high [9]. In Egypt, the prevalence of U.I cases with bacteria among girls and women ranged from 22 to 35% in 2019 and increased to 53.5% in 2020. E. coli is the most common bacterium causing 80-90% of community-acquired UIs and 30-50% of nosocomial-acquired UIs [10].
1.2. Aim of the Study
This study aimed to evaluate the effect of urogenital infection educational program on women’s knowledge and practices through:
(a) Assessment of women's knowledge and practices about urogenital infection,
(b) Assessment of the lifestyle of women.
(c) Development and implementation of an educational program for women according to their needs, and
(d) Evaluation of the effects of the educational program on women's knowledge and practices.
2. SUBJECTS AND METHODS
2.1. Research Design
A quasi-experimental one group pre/post-test research design was utilized in this study.
2.1.1. Settings
The current study was carried out at El Hadaka Maternity and Children’s Hospital (MCH) in Fayoum, one of the districts in Egypt because the turnover of women is satisfactory for the study. This institution is composed of one building with two floors. The first floor contains outpatient clinics of gynecology, emergency unit, medicine, pediatrics, and administration offices. The second floor contains a laboratory, dermatology clinics, and a children's care home.
2.1.2. Sampling
A convenience sample consisting of all the 50 available patients who qualified for the inclusion criteria, were considered for the study. For an experimental study, the required sample size is supposed to be above 50; however, this study only considered 50 respondents owing to the fact that most of the gynecologic patients were sent home due to the coronavirus pandemic.
2.1.3. Inclusion Criteria
Women who suffer from urogenital infection with ages ranging from 30 to 45 years old, with different educational attainment, fully oriented, did not attend previous training courses about urogenital infection and those who granted their consent for participation were considered for this study. The tools of data collection include:
2.1.4. Tool I: A Structured Interview Questionnaire (pre/post/follow up)
The questionnaire was adopted from previous studies [11, 12] and modified by the researchers in a simple, clear Arabic language based on the related literature review and experts' opinions in the light of relevant references to assess women's knowledge and reported practices about urogenital infection. This consists of three parts:
- √ Part I: Demographic characteristics of the women: This includes the respondents’ age, residence, educational status, marital status, chronic disease, and body mass index (BMI).
- √ Part II: Women's knowledge about urogenital infection: This includes seven questions about the meaning, causes, risk factors, symptoms, complications, preventive measures, and treatment regimen of urogenital infection (Figs. 1 and 2).
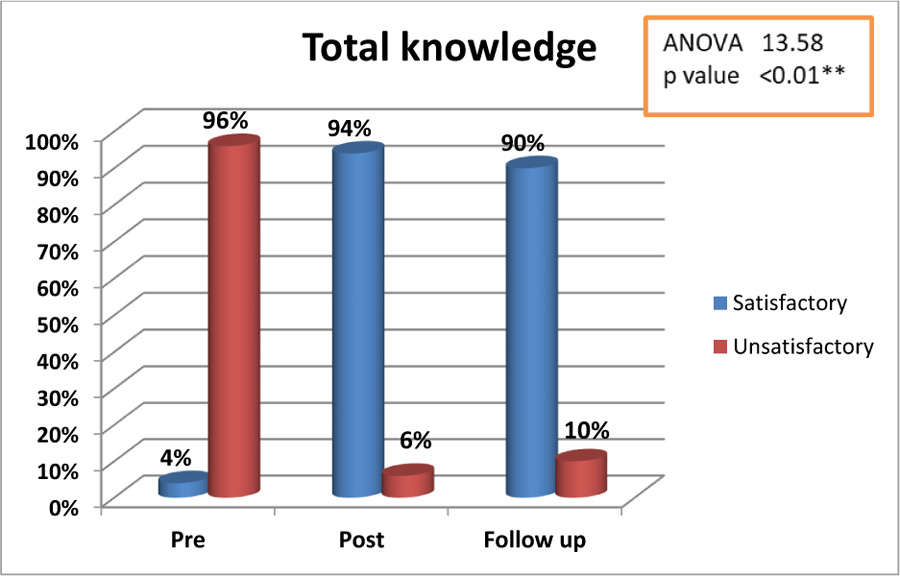
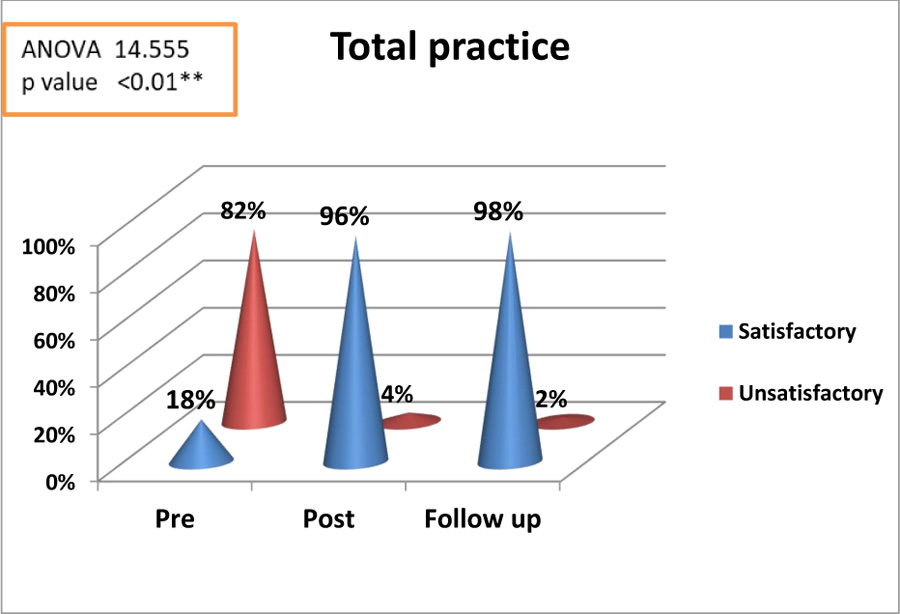
Fig. (1) showed that 96% of the studied women had unsatisfactory knowledge level about urogenital infection pre intervention, while 94% of them had satisfactory knowledge at the post intervention and 90% of them had satisfactory knowledge follow up, stage with highly significant difference with (p value <0.01**).
Fig. (2) showed that 82% of the studied women had unsatisfactory reported practice at pre-intervention, while 96% of them had satisfactory reported practice at post-intervention and 98% of them had satisfactory reported practice at the follow-up stage, with high statistically significant difference with p-value <0.01**.
2.2. Scoring System
For knowledge, a correct answer was scored as one and an incorrect answer as zero. The scores were summed up and converted into a percentage score. Those who garnered a score of zero to less than 60% were interpreted as having an unsatisfactory level of knowledge. The satisfactory level was for those who gained more than 6%.
√ Part III: Reported practices of women about urogenital infection: This included eleven items such as handwashing before and after bathing, cleanliness of the genital area after each urination/defecation, drying of the genital area after cleaning them, wearing cotton and loose underwear, constantly changing of underwear, washing underwear using hot water, exposing clothes to sun rays, drinking plenty of water daily, frequent emptying of the bladder when full, and cleaning the perineum from front to back after elimination.
2.3. Scoring System
The practices that were carried out correctly will be given a score of one, while zero was given for the actions that were not completed. The scores were summed up and converted into a percentage score. Those who garnered a score of zero to less than 60% were interpreted as unsatisfactory reported practices, while the satisfactory reported practices for those who gained more than 60%.
√ Tool IV: The Lifestyle of Women Scale: This was adapted from a study [13] and were assessed by a 46 item self-report standard instrument with the following five subscales reflecting domains such as exercise (5 items), nutrition (14 items), prevention (15 items), stress management (5 items) and social relationship (7 items). All questions contain 5-point Likert scale (never, rarely, sometimes, often, and always), yielding a score from 1 to 5. A score of one was considered as high-risk behavior and five, for the best, healthy behavior. The minimum and maximum scores of the instrument were from 46 - 230; the high score means a good lifestyle. Kindly indicate how will you interpret the scores. Please include the scaling and the interpretation.
2.3.1. Fieldwork
- Before starting the study, an official letter was written to the Dean of the faculty of nursing from the Director of MCH Center to request his permission and cooperation to allow for data collection from the selecting setting.
- The effect of the urogenital infection educational program on women’s knowledge and practices was evaluated, a review of the available past and current literature and theoretical knowledge was done, using books, articles, and magazines to develop the tools for data collection.
- After approval was granted, one of the researchers conducted a documentary search and analysis of the MCH Center medical files and documents of women seeking care at the said institution to identify the total population and the sample size. A total of 72 women were selected through the convenience sampling method. Out of this number, 22 patients were excluded (12 patients did not meet the inclusion criteria and 10 patients declined to participate in the study).
The data collection was started thereafter using the research tools and lasted for six months (from July 2020 to January 2021) spanning from the pre-assessment until the implementation and evaluation phases. The interview among the respondents was conducted in one of the waiting areas of the MCH Center.
2.4. Content Validity and Reliability
The tools of the study were translated by the researchers into Arabic language and were validated by a jury to ensure the content validity of the translated version by the original one. The jury consisted of seven experts from faculty staff in the community health and maternity nursing fields. The required correlation and modifications were carried out accordingly. The developed tools were tested for reliability. The reliability test of the translated version was established by using Cronbach's alpha which showed good internal consistency construct validity. Cronbach's Alpha coefficient test for lifestyle was = (0.869) and for structured interview questionnaire, it was = (0.855).
2.4.1. Pilot Study
A pilot study was conducted before starting data collection on (five women) randomly from the previously mentioned setting. The purpose of the study was to estimate the time required for filling in the tools and checking the clarity, applicability, and relevance of the questions. Results were used as a guide to reconstruct the changes required in the data collection tools and were included in the study sample.
2.5. Ethical Considerations
Official permission to conduct the study was obtained from the medical director EL Hadaka M.C.H center at Fayoum. The researcher met the medical director to explain the purpose and the methods of the data collection. Informed consent was obtained from the participants in this study after explanation of the purpose of the study, and assurance of the subject about the privacy and confidentiality of the obtained data. A summary of the interventions was explained to all respondents who voluntarily agreed to participate in the study. They were likewise informed that they could withdraw from the study at any time without giving any reason. The respondents accomplishedthe structured questionnaire related to their demographic data (Table 1), which took about five to ten minutes. Then, the investigator started to measure the women's knowledge, reported practice, and lifestyle (Table 2) using a prepared pretest in the form of a questionnaire.
| Items | n | % |
|---|---|---|
|
Age: 30- 35- 41-45 y Mean SD 40±2 |
17 26 7 |
34 52 14 |
|
Residence: - Rural |
50 | 100 |
|
Educational level: Illiterate Primary Secondary and diploma University |
5 8 18 19 |
10 16 36 38 |
|
Marital status: Married Widow Divorced |
24 17 9 |
48 34 18 |
|
Chronic disease Yes No |
38 12 |
76 24 |
| BMI: ≤19 19-25 25-30 |
14 23 13 |
28 46 26 |
Table 1 revealed that mean age of studied women was (40±2), 100% of them were form rural areas, 38% of them had university education and 24% of them were married. Also, reported that 76% of them suffered from chronic disease and 46% of them had BMI ranged from 19 to 25.
| Lifestyle Domains | Mean SD | Min | Max |
|---|---|---|---|
| Prevention | 59.4±5.9 | 32 | 70 |
| Exercise | 11.9±2.7 | 5 | 23 |
| Nutrition | 48.12±7.1 | 21 | 55 |
| Stress management | 14.3±3.7 | 7 | 25 |
| Social relation | 24.1±5.5 | 10 | 28 |
| Total | 157.82±18.7 | 99 | 206 |
Table 2 showed that mean of preventive domain n was (59.4±5.9), mean of exercise domain was (11.9±2.7), nutrition domain was (48.12±7.1), stress management domain was (14.3±3.7) and social relation was 24.1±5.5. Also, detected that mean of total lifestyle was (157.82±18.7), with minimum score 99, while maximum score was 206.
2.6. Program Construction:
2.6.1. The Program Consisted of Four Phases
The program development phase was based on the results obtained from the interview guide, questionnaire, literature review, and the following education principles. The researcher started to implement the program for all the participants.
2.6.1.1. Assessment Phase
The program was designed by the researchers based on the results of the assessment (pre-test and using the interview guide).
2.6.1.2. Planning Phase
This phase included analysis of the pre-test findings; the researcher then designed the program objectives and content according to the women’s responses and learning needs. The general objective of the program is to evaluate the effect of urogenital infection educational program on women’s knowledge and practices.
2.7. The Content of the Program
The educational program was implemented by the researchers. General principles stated in this program were educating, ensuring, guidance, empathy, encouragement, and the chance to express emotions to promote social support from others.
2.8. Implementation Phase
Studied subjects were divided into 10 groups, with five members each. A focus group discussion was held for each group consisting of five women using speech and pamphlets. The subjects were given with an invitation letter containing vital information like the purpose, time, and place of the training. The sessions were held at the waiting area twice a week (during Saturdays and Mondays), one hour per session (10-11 a.m.), lasting for three consecutive weeks.
2.8.1. First Session
The participants were introduced to each other and were notified about the method and structure of the sessions. The subjects’ expectations from the training program were identified, and the questionnaires were completed by the researcher.
2.8.2. Second Session
Meaning of urogenital infection and risk factors and causes of urogenital infection were explained and discussed.
2.8.3. Third Session
The subjects were acquainted with the symptoms of urogenital infection and treatment regimen of urogenital infections.
2.8.4. Fourth Session
Preventive measures of urogenital infection and women's practices related to prevention of urogenital infection were taught to the participants.
2.8.5. Fifth Session
By the end of every session, the participants,’ names were written down. The sessions ended after responding to their questions. The educational slides, papers, and charts were presented to the participants for practice and learning.
2.8.6. Evaluation Phase
Three assessments were performed to conduct the study. First was done before implementation of the educational program (using the study tools). The second time was done after the implementation of the educational program and the third time after three months. An interview among the respondents by the researcher was done to assess the follow-up phase by using the same tool or by using the telephone.
2.8.7. Statistical Analysis
Data collected from the studied sample were revised, coded, and entered using PC. Computerized data entry and statistical analysis were fulfilled using the Statistical Package for Social Sciences (SPSS), version 23. Data were presented using descriptive statistics in the form of frequencies and percentages. Analysis of variance (ANOVA) was utilized to determine whether the means of three or more groups are different. Correlation coefficients are used to measure how strong a relationship is between two variables. It was noted slightly significant if p-value was < 0.05, highly significant if p-value was < 0.01 and not significant if p-value > was 0.05.
3. DISCUSSION
Urogenital infections, as an important health element are associated with the risk of many problems among women. So, the support training program is an effective factor in reducing such problems [14]. The current study aimed to evaluate the effect of urogenital infection educational programs on women's knowledge and practices.
| Items | Pre | Post | Follow up | A nova test | P-value |
|---|---|---|---|---|---|
|
Correct N (%) |
Correct N (%) |
Correct N (%) |
|||
| Meaning of urogenital infection | 5 (10) | 41 (82) | 36 (72) | 9.141 | <0.01** |
| Symptoms of urogenital infection | 4 (8) | 38 (76) | 36 (72) | 7.685 | <0.01** |
| Causes of urogenital infection | 7 (14) | 43 (86) | 41 (82) | 10.243 | <0.01** |
| Complications of urogenital infection | 2 (4) | 37 (74) | 38 (76) | 9.055 | <0.01** |
| Risk factors of urogenital infection | 6 (12) | 44 (88) | 42 (84) | 8.738 | <0.01** |
| Preventive measures related to urogenital infection | 5 (10) | 45 (90) | 44 (88) | 10.016 | <0.01** |
| Ways of treatment | 2 (4) | 42 (84) | 40 (80 | 9.071 | <0.01** |
| Items | Pre | Post | Follow up | ANOVA test | P-value |
|---|---|---|---|---|---|
|
Done N (%) |
Done N (%) |
Done N (%) |
|||
| Washing hand before and after bathing | 25 (50) | 50(100) | 50(100) | 9.102 | <0.01** |
| Cleanliness genital area after each toilet | 45 (90) | 50(100) | 50(100) | 3.014 | <0.05* |
| dryness of genital area after cleanliness | 12 (24) | 48 (96) | 47(94) | 10.117 | <0.01** |
| Wearing cotton under wear | 14 (28) | 46 (92) | 94 (98) | 11.684 | <0.01** |
| Wearing loose under wear | 20 (40) | 47 (94) | 46 (92) | 9.938 | <0.01** |
| Continuous changing of underwear | 12 (24) | 48 (96) | 49 (98) | 10.205 | <0.01** |
| washing underwear clothes by hot water | 30 (60) | 50 (100) | 50 (100) | 9.056 | <0.01** |
| Exposing clothes to sun rays | 3 (6) | 40 (80) | 42 (84) | 8.878 | <0.01** |
| drink plenty of water daily | 17 (34) | 45 (90) | 47 (94) | 12.302 | <0.01** |
| Empty the bladder frequently when full | 20 (40) | 46 (92) | 48 (96) | 10.888 | <0.01** |
| Clean the perineum from front to back after elimination | 25 (50) | 50 (100) | 50 (100) | 9.764 | <0.01** |
According to the characteristics of the women under investigation, results show that the mean age was (40±2), almost all of them were from rural areas, and more than one-third of them had a university education. Likewise, it is noteworthy that about three-quarters of the women suffered from chronic diseases and less than half of them have BMI ranging between 19 to 25. These results are aligned with a study conducted in Turkey [15] entitled “Prevalence of urinary incontinence in Turkish women, risk factors, and effect on activities of daily living”, conducted in Turkey, which found out that the mean age of the women-respondents was (40±2.11) and more than half of them suffered from chronic disease. This was in contrast with the findings of the study [16, 17] about urinary incontinence and its association with functional physical and cognitive health among female nursing home residents in Switzerland which found out that the mean age of the women was (35±3.6) and more than one-third of them do not have any partner or spouse. As with the life style domains, the present study revealed that mean of the preventive domain was 59.4±5.9, 11.9±2.7 for the exercise domain, 48.12±7.1 for the nutrition domain, 14.3±3.7 for the stress management domain, and 24.1±5.5 for the social relation domain. Overall, the mean for total lifestyle was 157.82±18.7. These results coincide with the study in Iran [14] about the determinants of a healthy lifestyle and its related factors among elderly people. It can be noted that the mean score of prevention domain was 62.53±3.84, stress management was 16.94±2.33 and social relation was 21.62±5.02. Also, the current study agreed with another study [18] and reported that the mean score of the exercise domain was 12.48±3.5, prevention domain was 60.95±4.93 and nutrition domain was 37.33±4.49 and total lifestyle was 152.5±16.25.
As with the distribution of the respondents according to their knowledge about urogenital infection (Table 3) at pre, post and follow up, the current study demonstrated that most of the studied women have unsatisfactory knowledge about urogenital infection at pre-intervention. In contrast, most of them have satisfactory knowledge at post-intervention and the majority of them have satisfactory knowledge at follow up, with highly significant improvement at all items of knowledge between pre, post and follow up an intervention with p-value <0.01. These results explained that the training program was developed based on precision the results of the pre-assessment, and researchers considered the women's needs. This result is supported by a study [19, 20] in Egypt, which found out that the result after three months among the intervention group was significantly higher than the control group (Table 4).
The performance of the study group to prevent urinary tract infection after the implementation of the education program increased from 2.85 ± 0.51 to 3.74 ± 0.29 (out of 4) (p = 0.001). This is similar to the cohort study [21] about “the effect of education on knowledge, attitude, and practices of patients with vaginitis” in rural South Africa and revealed that a significant increase in the mean score of knowledge, attitude, and practices of the patients in the intervention group was after the educational program implementation.
Regarding the distribution of the studied women related to their reported practices about urogenital infection at pre, post and follow up stages, this study revealed that more than three-quarters of studied women have unsatisfactory practices at pre-intervention, while most of them have satisfactory practices at post-intervention. Most of them have manifested satisfactory practices during the follow-up stage with a highly significant improvement in relation to wearing cotton underwear, wearing loose underwear, continuous changing of underwear, washing underwear with hot water, exposing clothes to sun rays, drinking plenty of water daily across the pre, and post phases an intervention with p-value <0.01.
These results can be attributed to accurately implementing the training program, distributing the participants into a small group, using clear, easy, and simple language, giving an opportunity to questions and using explanatory methods such as videos, pictures, and posters. These results are consistent with the study conducted [22] along the same line of topic but involving women with vulvovaginitis in Egypt which reported that the majority of the women have unsatisfactory levels of self-care practices before the educational intervention. However, about three-quarters of them manifested a satisfactory level of self-care practices after the educational intervention, some authors [23, 24] agree with these findings with the study about urinary tract infection performed in Iran and revealed that counseling and phone follow-up were effective in improving level of knowledge, attitude, and performance among women in preventing urinary infection.
The correlation between lifestyle, knowledge, and practice level revealed that there was a highly positive correlation between total lifestyle and knowledge and practice at pre-intervention with a p-value <0.01. Likewise, a high positive correlation exists between knowledge level and their reported practice level at pre-intervention with a p-value <0.01 was revealed. These results were similar to a previously conducted study [21, 25] about knowledge, attitude, and practices of women towards the vaginal discharge and urogenital infection in India who found that there was a high positive correlation between women knowledge and their practice at p-value <0.01.
Table 3 showed that 10% of studied women had correct knowledge about the meaning of urogenital infection pre-intervention, while 82% of them had correct knowledge at the post-test and 72% of them had correct knowledge at follow-up intervention. Also, only 4% of them had correct knowledge related to complications of urogenital infection, at pre-intervention while 88% of them had correct knowledge at the post-intervention and 84% of them had correct knowledge at follow-up assessment. In relation to the ANOVA test, there was highly significant improvement at all items of knowledge between pre, post and follow-up intervention with (p-value <0.01**).
Table 4 demonstrated that 50% of studies reported correct practice about washing hands before and after bathing pre-intervention, while all of them corrected their practice at post and follow-up intervention with p-value <0.01**. Also, 90% of them cleaned genital area after each toilet visit at pre-intervention, while the rest of them cleaned at post-intervention and follow-up stages with p-value <0.05*. In relation to the ANOVA test, there was highly significant improvement at wearing cotton underwear, wearing loose underwear, continuous changing of the underwear, washing underwear clothes by hot water, exposing clothes to sun rays, drink plenty of water daily between pre, post and follow up intervention with (p-value <0.01**).
4. IMPLICATIONS OF THE STUDY
The findings of this study have implications and can guide policymakers at the governmental levels. At the very least, on a national level, it is critical for governments to see health issues or to take note of women's health and well-being. Future studies should consider the factors affecting the prevalence of urogenital infections among women. The recommendations for this study will be discussed under nursing education and nursing research.
CONCLUSION
Study results have revealed significant improvements in women's knowledge and reported practices related to a urogenital infection during the post program intervention phase. Also, there was a positive correlation between total lifestyle and knowledge and practices at pre-intervention, as manifested by p-value of <0.01.
RECOMMENDATIONS
The findings of this current study recommend providing different educational programs regarding knowledge and self-care practices for women with urogenital infection at different women's care settings. Continuous assessment of women's level of knowledge and practices related to urogenital infections are effective in controlling the infection. Replication of this study on a large sample and at different settings is recommended for the generalization of results.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The ethical approval was taken from the medical director and ethical committee of EL Hadaka M.C.H at Fayoum, which granted permission to conduct this study.
HUMAN AND ANIMAL RIGHTS
No animals were used for studies that are base of this research. All the humans used were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from the participants in this study after explaining the purpose of the study and assurance of the subject about the privacy and confidentiality of the obtained data. A summary of the interventions was explained to all respondents who voluntarily agreed to participate in the study.
STANDARDS OF REPORTING
STROBE guidelines and methodologies were followed for this study.
AVAILABILITY OF DATA AND MATERIALS
The data sets used during the current study can be provided from the corresponding author [S.B], upon reasonable request.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflicts of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors gratefully acknowledge the Deanship of the Scientific Research in Fayoum University, Egypt and King Faisal University.

