All published articles of this journal are available on ScienceDirect.

The Impact of Islamic-Based Disaster Response Competencies Program on Nurses: A Computer-based Training Randomized Controlled Trial
Abstract
Introduction:
Disasters have a significant impact on physical, psychological, psychosocial, and spiritual conditions. Indonesia, a predominately Muslim country, is a country of high vulnerability and risk for disasters. The nurses are frontliners and care providers need sufficient competencies in handling the survivors in health service centers. Local government regulations in the Aceh Province required Islamic-based health services.
Objective:
The study aims to identify the effectiveness of the Islamic-based disaster response competencies on nurses at the Banda Aceh Hospitals.
Methods:
A randomized controlled trial with a pre- and post-tests with a control group design was used in this study. The population was all nurses at three hospitals in four wards: emergency department, intensive care, medical, and surgical wards. The samples were selected using cluster random sampling and assigned into three groups: evidence = 50, Islamic = 49, and control = 48. Data were analyzed using parametric and non-parametric tests.
Results:
The results showed a significant increase in nurses’ knowledge, skills, and attitudes of disaster response in the evidence and Islamic groups with the mean and SD of the Islamic group in post-test 1 and 2 (knowledge = 15.9±2.9 and 15.8±2.9, skills = 19.0±1.4 and 18.9±1.4, attitude = 108.1±6.9 and 108.2±6.9) were higher than the evidence group (knowledge = 15.6±2.7 and 15.5±2.7, skills = 18.7±1.5 and 18.8±1.5, attitudes = 107.5±7.4 and 107.4±7.3) and the control group (knowledge=13.8±4.0 and 13.9±4.0, skills = 17.9±1.9 and 17.9±1.9, attitude = 104.5±8.8 and 104.6±8.8), respectively.
Conclusion:
The results indicate the Islamic group is more effective in increasing the disaster response competencies of nurses. This finding suggests the importance of developing regulations including policies, guidelines, emergency and disaster training, and public health services to support the implementation of an appropriate Islamic-based disaster nursing responses for hospitals in the Aceh Province and other regions with the implementation of Islamic law. Request number ANZCTR 378930
1. INTRODUCTION
Indonesia is one of the high-risk countries for natural disasters because of its location at the confluence of the three major plates of the world; the Indo-Australia, Eurasia, and the Pacific [1]. Disasters, led by natural, non-natural, and human factors, threaten the population in the region by causing casualty, environmental damage, property loss, and psychological impact [2]. Although the incidence and frequency of disasters have increased in the last few decades and resulted in many casualties, therefore, disaster management is not well managed [3-5]. The adequacy of disaster preparedness and response should be the main priority, especially in high-risk areas of disasters, by increasing the responsiveness of health workers, including nurses in hospitals and community settings.
As a public health services center, hospitals play an urgent role when a disaster occurs. Disaster response in hospitals to manage the survivors is an important indicator in disaster management. Hospitals must prepare the necessary resources, especially equipment, ward/department, medical personnel, and nurses, through adequate emergency preparedness and hospital disaster plans. In case the hospital is destroyed by the disaster; a field hospital is required to handle the survivors [6]. Nurses are the frontline workers who have the main role in the disaster response. Thus, adequate disaster response competencies are needed, including knowledge, skills, and attitudes regarding services for disaster survivors through education and training programs [3]. The competencies and roles of nurses in both the preparedness and disaster response phases are inadequate in caring for disaster survivors. The previous study reported that 88% of the population affected was still dissatisfied with the skills shown by nurses and physicians in caring for disaster survivors [7, 8].
Disasters negatively impact the exposed communities, such as physical, psychological, psychosocial, and spiritual problems. Nurses’ competencies in handling these problems have been described in some literature [9, 10]. However, Islamic-based interventions to address these problems have not been reported. The implementation of Islamic law is based on the holy book of the Quran and hadith, which are used as guidelines in Islamic-based health service interventions. Efforts to support Islamic-based nurses’ competencies are strongly supported by implementing Islamic law in public services, including hospitals. Aceh is a province in Indonesia where 98.19% of the population is Muslim. The implementation of Islamic law in Aceh has been carried out since 2000 [11].
This study adopts a conceptual framework about emergency preparedness competency dimensions and disaster nursing competencies, and all-hazard disaster core competencies for acute care medical professionals consist of handling physical, psychological, and psychosocial problems [10, 12]. Also, spiritual competencies contained in spiritual care and nursing; a nurse contribution and practice must consider human diversity (culture, belief, and values) [9], and the conceptual framework for Islamic-based competencies about the standard of service for sharia hospitals [13], based on Islamic law (the Holy Quran and hadith) and need asssement to care for the survivors, that found four themes: (1) the perception of disaster in an Islamic perspective consisted of: disaster as a destiny from God, a test of faith, and a warning from God, (2) the skills and attitudes of nurses in disaster response are sincerity, caring, empathy, and patience, (3) the role of nurses in disaster response is by integrating Islamic values in patient care: prayer, dzikir (remembrance), shalawat, (salutation to Prophet Mohammad PBUH (Peace Be Upon Him), reciting Al-Quran, and endeavors, and motivating patient through surah Nabawiyah (the story of the prophets), and (4) nurses’ competencies barriers in disaster response.
The religiosity, Islamic values, beliefs, and also the regulation of local government to implement Islamic-based health care services are reinforcement to support for this study. This research was conducted to assess the impact of an Islamic-based disaster intervention program on nurses’ competencies of disaster response in dealing with survivors’ psychological, psychosocial, and spiritual problems.
2. METHODS
2.1. Study Design
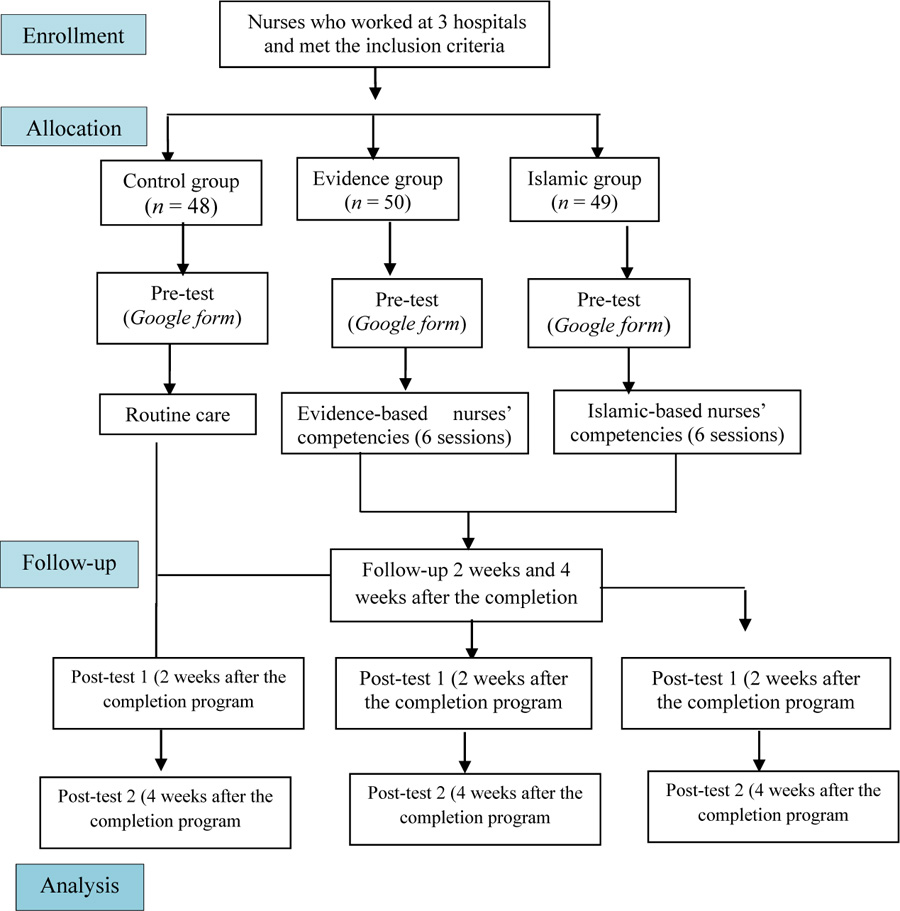
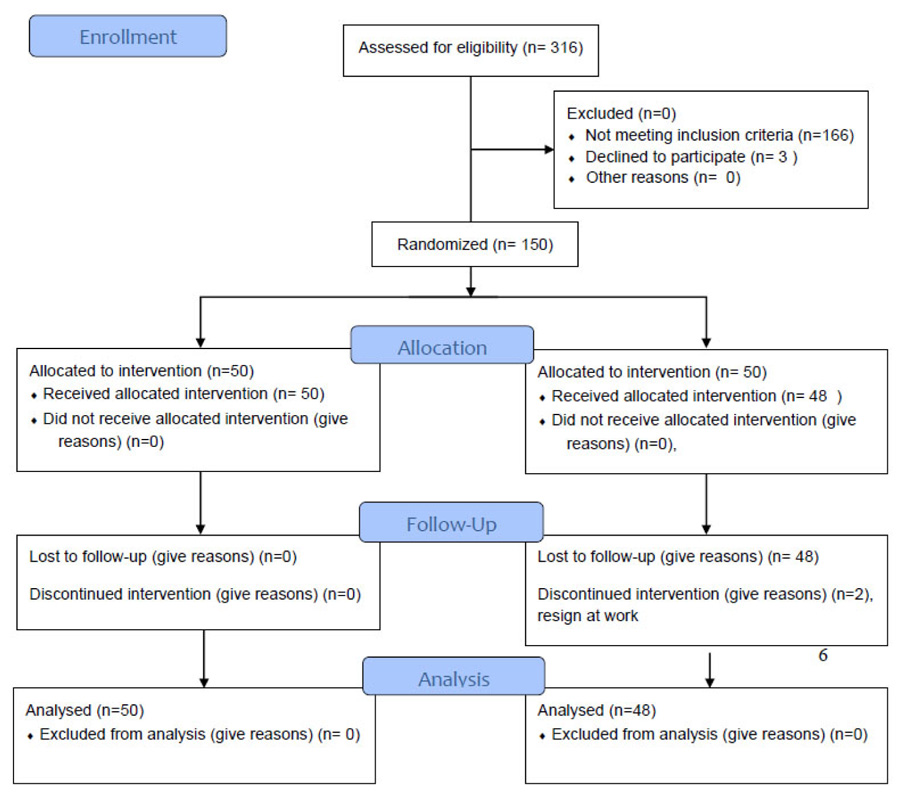
A quantitative study with a randomized controlled trial (RCT) with a pre-test and post-test control group design was conducted in this study consisted of three groups; evidence, Islamic, and control groups. Evidence group was an intervention group using disaster response competencies based on the International Council of Nurses and other studies. Islamic group was an intervention group according to the standard of service for sharia hospitals (Islamic law) and needed asssement by focus group discussion; meanwhile, the control group did not provide intervention, but only routine care. The RCT intervention program of this study is as follow (Figs. 1a and 1b).
2.2. Participants
The population in this study were nurses working in four wards; (1) emergency department (ED), (2) intensive care (IC), (3) medical ward, and (4) surgical ward. This study applied a medium effect size with a power of 0.08, a confidence level of 95% (α=0.05), and a value of d Cohen = 0.60, so the sample size was 45 respondents [14, 15]. To avoid the attrition rate, the sample size was increased by 10%, generating the total number of respondents were 150 people (50 respondents in each group). The sample selection used random cluster sampling with the following inclusion criteria: a) nurses in the emergency department, intensive care ward, medical ward, and surgical ward, b) working period ≥ two years, c) minimum educational background of Diploma in Nursing, and d) not currently on leave annual/study assignments. The number of final samples in the training program for each group was as follows: the evidence group = 50, Islamic = 49, and control = 48 respondents.
2.3. Randomization
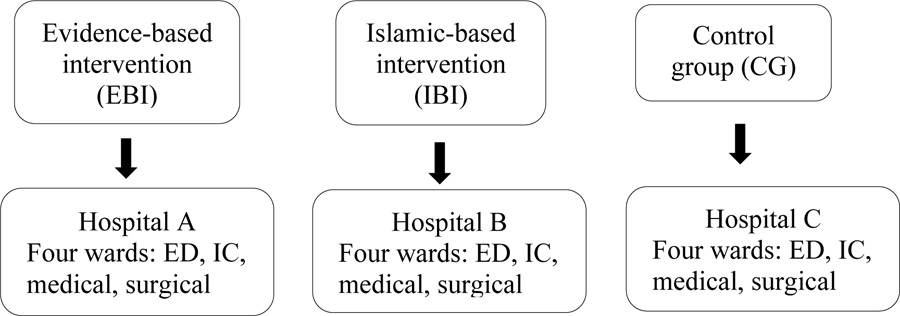
Samples were selected by random cluster sampling in four wards at three hospitals in Banda Aceh. The samples consisted of three groups; Evidence-based intervention/EBI (hospital A), Islamic-based intervention/IBI (hospital B) and control group/CG (hospital C). The sample selection was in accordance with the inclusion criteria by making clusters for each designated ward (Fig. 2).
2.4. Program Development
The program development began with three focus groups with 24 nurses and nine disaster survivors, and three series of face-to-face in-depth interviews with eight policymakers at the hospital and nine members of the Aceh Ulama Consultative Council, Indonesia. Focus group discussions (FGDs) and in-depth interviews aimed to identify and explore the need for nurses’ disaster response competencies in handling psychological, psychosocial, and spiritual problems due to disasters. This development program is useful to support intervention and implementation programs at the nurse training stage.
2.5. Program Intervention and Implementation
2.5.1. The Evidence-based Intervention (Evidence group)
In this group, the intervention focused on the evidence-based intervention for nurses in hospitals using standardized nurses’ competencies in disaster response adopted from International Council of Nurses (ICN) than other literatures, consisting of six sessions with a duration of 60-90 minutes/session. The intervention material consists of knowledge of disaster overview, causes and impacts of disasters, and nurses' competencies in handling psychological, psychosocial, and spiritual problems. Nurses' skills in handling psychological, psychosocial, and spiritual problems in disasters include educational care, emotional care, counseling care, support, advocacy, and referrals. Finally, attitudes in caring for disaster survivors include patient-centered care, open vs. closed questions, and good listening skills. The method of intervention comprised lectures, discussions, demonstrations, active learning through role-play, and storytelling.
2.5.2. The Islamic-based Intervention (Islamic group)
In this group using nurses’ competencies in disaster response adopted from the standard of service for sharia hospitals (Islamic law) and need assesments from FGDs.The intervention focused on the Islamic-Based Disaster Response Competencies for Nurses in Hospital, consisting of six sessions with a duration of 60-90 minutes/session. The intervention materials consisted of 1) the concept of disasters from an Islamic perspective, 2) the impact of disasters and disaster management laws in Indonesia, symptoms of psychological, psychosocial, and spiritual problems related to disasters, 3) Islamic-based disaster response knowledge, skills, and attitudes to nurses in handling psychological, psychosocial, and spiritual problems, 4) the concept of self-consciousness, 5) Islamic-based emotional freedom technique (EFT), 6) ikhtiar (endeavor), doa (prayers), and tawakkal (trusting in God’s plan) in response disaster, and termination and follow-up plans. The intervention method included lectures, discussions, demonstrations, active learning through role-play, and storytelling.
2.6. Program Providers
According to their respective competencies and expertise, four experts were selected: disaster nursing nurse, psychiatric nurse, psychologist, and Islamic scholar. For the evidence-based intervention group, the program providers were a disaster nursing nurse, a psychiatric nurse, and a psychologist. For the Islamic-based intervention group, apart from three other providers, an Islamic scholar was added with an intensive training program on Islamic-based disaster response competencies for nurses to handle psychological, psychosocial, and spiritual problems.
A one-day training of providers was conducted to optimize the implementation of the intervention program and uniform perceptions, goals, achievements, and the expected results on each of these training materials. The training activities consisted of the introduction of the training objectives and programs, materials, methods, media, and evaluation used for the six sessions of the intervention program. All experts and researchers discussed and shared their expertise and experience to be developed as resources used in this training program.
2.7. Ethical Considerations
This study pays attention to ethical principles in nursing research. The respondents involved in this study signed written informed consent to indicate their willingness. This study was approved for ethical considerations by the Ethics Committee of Dr. Zainoel Abidin Banda Aceh Hospital, with number 1171012P dated January 25, 2019.
2.8. Primary Outcomes
The primary outcomes of this study were the nurses’ competencies, including knowledge, skills, and attitude of disaster response to deal with psychological, psychosocial, and spiritual problems, which were measured by a questionnaire. It was adopted from the literature [9, 12, 13, 16] and used for the development of training materials and modules the intervention program.
2.9. Development and Testing of the Instrument
The questionnaire was developed based on the literature review and consisted of four parts: demographic data, knowledge of nurses, skills of nurses, and attitudes of nurses in disaster response. The questionnaire was tested for content validity using the content validity index by three experts in their fields related to research topics: a) an expert nurse in disaster nursing, b) a psychologist, and c) an Islamic scholar from Aceh. The reliability of the instrument was assessed by the Cronbach alpha, which was carried out on 38 nurses at regional hospital Banda Aceh. The results of the reliability test for the nurses’ were knowledge = 0.80, attitude = 0.86, and skills = 0.70.
2.9.1. Demographic Information
Demographic data included age (years), gender, highest educational level, ward, working experience (years), attendance in disaster/emergency training (yes/no, if “yes” the type of training and the year).
2.9.2. Nurses’ Knowledge about Disaster
The nurses’ knowledge of disaster response was measured using 22 multiple-choice items. Each question consisted of five answers, scored “1” for the correct answer and “0” for the wrong answer. The total scores ranged from 0-22, with the high scores describing the high nurses’ knowledge of disaster response.
2.9.3. Nurses’ Skills about Disaster
Nurses' skills of disaster response were measured using 20 dichotomous items. Each statement was scored “1” for the correct answer and “0” for the wrong answer. The total scores ranged from 0-20, with the high scores describing the high nurses’ disaster response skills.
2.9.4. Nurses’ Attitude about Disaster
Nurses’ attitudes of disaster response were measured using 24 items a-5 points Likert scale (1=strongly disagree, 2=disagree, 3=doubtful, 4=agree, and 5=strongly agree). The total value was from 1 to 120, with the high scores describing the high nurses’ attitudes in disaster response.
2.10. Study Procedure
The training program in the intervention group was carried out in six sessions in six weeks with 60-90 minutes/session. It was computer-based training due to the COVID-19 pandemic. The evaluation began with a pre-test, followed by materials provided by the program providers. The post-test was carried out twice. Post-test 1 was carried out two weeks, and post-test 2 four weeks after the completion program. The evaluation was carried out using google form assisted by three research assistants who had no affiliation with the hospitals.
2.11. Statistical Analysis
Descriptive statistics were used for frequency, percentage, mean, and standard deviation. Inferential statistics using for parametric and non-parametric tests. This study used a type 1 error of p<0.05 as the criterion for statistical tests used to determine the effects and interactions of each analysis. Data analysis was conducted using SPSS version 12.0.
3. RESULTS
3.1. Subject Characteristic
Demographic characteristics of respondents consisted of age, gender, highest educational level, religion, working experience, disaster training attendance, and the type of training attended are shown in Table 1.
| Characteristics |
Evidence (n = 50) |
Islamic (n = 49) |
Control (n = 48) |
P-value |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | ||
|
Age (Year); (M±SD) |
33.9±5.6) | 32.5±3.4 | 29.0±3.9 | 0.406 |
|
Gender: Male Female |
7 (14) 43 (86) |
16 (32.7) 33 (67.3) |
11 (23) 37 (77) |
0.000 |
|
Highest Educational Level Diploma Bachelor |
33 (66) 17 (34) |
29 (59.2) 20 (40.8) |
34 (70.8) 14 (29.2) |
0.077 |
|
Working Experience (Year) (M±SD) |
2.4 ±2.8 | 7.4±3.4 | 2.7±1.5 | 0.770 |
|
Disaster Training Attendance: Yes No |
11 (22) 39 (78) |
14 (28.6) 35 (71.4) |
13 (27.1) 35 (72.9) |
0.278 |
|
Types of Disaster Training Attended: Basic Life Support Basic Trauma Cardiac Life Support Light Fire Extinguisher (LFE) Disaster Management (drill) |
8 (16) 10 (20) 11 (24) 6 (12) |
10 (20.4) 11 (22.4) 9 (18.3) 4 (8.1) |
8 (16.6) 12 (25) 12 (25) 4 (8.3) |
0.592 |
| Outcomes |
Evidence (n = 50) |
Control (n = 48) |
P-value |
Islamic (n = 49) |
Control (n = 48) |
P-value |
Evidence (n = 50) |
Islamic (n = 49) |
P- value |
||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MR | SR | MR | SR | - | MR | SR | MR | SR | - | MR | SR | MR | SR | - | |
| Knowledge Pre-test Post-test 1 Post-test 2 |
49.98 56.45 55.80 |
2499.0 2822.5 2790.0 |
49.00 42.26 42.94 |
2352.0 2028.5 2061.0 |
0.864 0.013 0.024 |
49.96 56.16 55.93 |
2448.0 2752.0 2740.5 |
48.02 41.69 41.93 |
2305.0 2001.0 2012.5 |
0.733 0.011 0.013 |
49.08 49.00 48.47 |
2454 2450 2423 |
49.94 49.00 48.47 |
2397 2401 2427.5 |
0.881 0.857 0.711 |
| Skills Pre-test Post-test 1 Post-test 2 |
50.08 58.48 57.84 |
2504.0 2924.0 2892.0 |
48.90 40.15 40.81 |
2347.0 1927.0 1959.0 |
0.833 0.001 0.002 |
50.20 58.39 57.21 |
2460.0 2861.0 2803.5 |
47.77 39.43 40.61 |
2293.0 1892.0 1949.5 |
0.663 0.001 0.003 |
48.65 48.66 49.64 |
2432.5 2433 2468.5 |
50.39 50.38 49.64 |
2418.5 2418 23.82 |
0.757 0.741 0.960 |
| Attitude Pre-test Post-test 1 Post-test 2 |
49.97 55.60 55.25 |
2498.5 2780.0 2762.5 |
49.01 43.15 43.51 |
2352.5 2071.0 2088.5 |
0.867 0.030 0.041 |
49.58 55.16 55.01 |
2429.5 2703.0 2695.5 |
48.41 42.71 42.86 |
2323.5 2050.0 2057.0 |
0.837 0.029 0.033 |
49.61 49.12 49.05 |
2480.5 2456 2452.5 |
49.39 49.90 49.64 |
2370.5 2395 2398.5 |
0.969 0.892 0.873 |
Table 1 shows the mean of age and standard deviation (SD) in the evidence-based group = 33.9 ± 5.6, Islamic-based = 32.5 ± 3.4, and the control = 29.0 ± 3.9. The respondents in three groups were mainly females (evidence= 86%, Islamic= 67.3%, control = 77%). Concerning the respondents' religion, 100% is Islam, while the educational level in the three groups was dominated by Diploma (evidence = 66%, Islami = 59.2%, and control = 70.8%). For the working experience, the highest mean and SD = 7.4 ± 3.4 was found in the Islamic group, and the lowest was in the evidence group, with the mean and SD = 2.4 ± 2.8. Disaster training attendance was dominated by the Islamic group (28.6%), and the disaster training attended was mainly control group, namely basic trauma cardiac life support and LFE, by 25%, respectively. There were no differences between the three groups based on their demographic characteristics.
3.2. Effect of the Interventions on Knowledge
The analysis results of three mean scores in the evidence, Islamic, and control groups were conducted using the Kruskal-Wallis test in the pre-test, post-test 1, post-test 2 to assess the difference of disaster response knowledge are shown in Table 3. The results of the study showed significant differences of knowledge in post-test 1 (p-value = 0.014) and post-test 2 (p-value = 0.023) between the evidence, Islamic, and control groups. The statistical results indicate a significant effect on knowledge of disaster response in the post-test 1 and post-test 2 in the evidence and Islamic groups.
Effects of the intervention programs on nurses’ knowledge of disaster response are shown in Table 2. For the nurses’ knowledge, there was no significant difference in the pre-test between the evidence and control groups (p-value = 0.864) and between the Islamic and control groups (p-value = 0.733). However, after the intervention program, significant differences in post-test 1 were indicated in the knowledge of disaster response between the evidence and control groups (p-value = 0.013) and between Islamic and control groups at post-test 1 (p-value = 0.011). The results indicated the difference in nurses’ knowledge of the disaster response in both the evidence and Islamic groups compared to the control group in pre-test and post-test 1.
3.3. Effect of the Interventions on Skills
In the analysis, results of three mean scores in the pre-test, post-test 1, post-test 2 in the evidence, Islamic, and control groups using the Kruskal-Wallis test are shown in Table 3. It shows significant differences in the mean rank of skills in the evidence, Islamic, and control groups in the post-test 1 (p-value = 0.001) and post-test 2 (p-value = 0.002). These results concluded a significant effect of disaster response skills on nurses in the post-test 1 and post-test 2 in the evidence, Islamic, and control groups.
Effects of the intervention programs on disaster response skills among nurses are presented in Table 2. For the nurses’ skills, there was no significant difference of pre-test between the evidence and control groups (p-value = 0.833) and between the Islamic group and control (p-value = 0.66). After the intervention program, a significant difference was found in effect on disaster response skills between the evidence and control groups (p-value = 0.001) and between the Islamic and control groups (p-value = 0.001). The results indicate a significant difference in disaster response skills among nurses in both the evidence and Islamic groups compared to the control group in post-test 1.
3.4. Effect of the Interventions on Attitude
The results of the mean score in the pre-test, post-test 1, post-test 2 in the evidence, Islamic, and control groups are shown in Table 3. There were significant differences in disaster response attitudes in the evidence, Islamic and control groups on the post-test 1 (p-value = 0.042) and post-test 2 (p-value = 0.050) at α = 0.05. These results indicate a significant effect on nurses’ attitude of disaster response in the post-test 1 and post-test 2 in the evidence, Islamic, and control groups.
Effects of the interventions on disaster response attitude among nurses are shown in Table 2. Concerning the nurses’ attitudes for disaster response, there was no significant difference in the pre-test between the evidence and control groups (p-value = 0.867) and between the Islamic group with control (p-value = 0.837). After the intervention program, it showed a significant difference in the effect of disaster response attitudes between the evidence and control groups (p-value = 0.001) and between Islamic and control groups (p= 0.001). The results concluded a significant difference in disaster response attitudes among nurses in both the evidence and Islamic groups compared to the control group in post-test 1.
Table 3 shows a significant difference in the nurses’ knowledge of disaster response on post-test 1, with M ± SD (15.6 ± 2.7), and post-test 2 (15.5 ± 2.7), higher than the pre-test (13.9 ± 3.9). The skills of nurses in the disaster response in the post-test 1 (18.9 ± 1.5) and post-test 2 (18.8 ± 1.5) were higher than the pre-test (17.9 ± 1.9), and the nurses’ attitude in disasters response on the post-test 1 (107.5 ± 7.4) and post-test 2 (107.4 ± 7.3) were also higher than the pre-test (104.7 ± 8.6). The comparison is shown in Table 4 below.
| Outcomes | Evidence (n = 50) | Islamic (n = 49) | Control (n = 48) |
|---|---|---|---|
| M±SD | M± SD | M± SD | |
| Knowledge | - | - | - |
| Pre-test | 13.9±3.9 | 13.9±4.0 | 13.7±4.0 |
| Posttest 1 | 15.6±2.7 | 15.9±2.9 | 13.8±4.0 |
| Posttest 2 | 15.5±2.7 | 15.8±2.9 | 13.8±4.0 |
| Skills | - | - | - |
| Pre-test | 17.9±1.9 | 17.9±1.9 | 17.7±1.9 |
| Posttest 1 | 18.7±1.5 | 19.0±1.4 | 17.8±2.0 |
| Posttest 2 | 18.8±1.5 | 18.9±1.4 | 17.9±1.9 |
| Attitude | - | - | - |
| Pre-test | 104.7±8.6 | 104.7±8.7 | 103.8±8.8 |
| Posttest 1 | 107.5±7.4 | 108.1±7.0 | 104.5±8.8 |
| Posttest 2 | 107.4±7.3 | 108.2±6.9 | 104.6±8.8 |
| Variables | Outcomes | Groups | MR | X2 | P-value |
|---|---|---|---|---|---|
| Knowledge | Pre-test | Evidence | 73.96 | 0.12 | 0.94 |
| Islamic | 75.49 | ||||
| Control | 72.52 | ||||
| Post-test 1 | Evidence | 80.55 | 8.49 | 0.01 | |
| Islamic | 81.57 | ||||
| Control | 59.45 | ||||
| Post-test 2 | Evidence | 79.35 | 7.54 | 0.02 | |
| Islamic | 81.90 | ||||
| Control | 60.36 | ||||
| Skills | Pre-test | Evidence | 73.90 | 0.20 | 0.91 |
| Islamic | 75.90 | ||||
| Control | 72.17 | ||||
| Post-test 1 | Evidence | 82.40 | 15.61 | 0.001 | |
| Islamic | 83.98 | ||||
| Control | 55.06 | ||||
| Post-test 2 | Evidence | 82.45 | 12.60 | 0.002 | |
| Islamic | 82.10 | ||||
| Control | 56.93 | ||||
| Attitude | Pre-test | Evidence | 74.32 | 0.05 | 0.98 |
| Islamic | 74.73 | ||||
| Control | 72.92 | ||||
| Post-test 1 | Evidence | 79.65 | 6.32 | 0.04 | |
| Islamic | 80.62 | ||||
| Control | 61.35 | ||||
| Post-test 2 | Evidence | 79.19 | 5.83 | 0.05 | |
| Islamic | 80.58 | ||||
| Control | 61.88 |
4. DISCUSSION
Disasters have a significant impact on physical, psychological, psychosocial and spiritual conditions. Sufficient competencies of nurses, as the frontliner workers in disaster response are needed in caring for survivors [17]. This intervention program was carried out for six sessions [18-20] in both intervention groups (Islamic and evidence) for 60-90 minutes/session for every week period and a control group. There were two follow-ups: post-test 1, carried out two weeks after the intervention program, and post-test 2, conducted one month after completion program [21].
Disaster response knowledge is obtained from formal, non-formal, informal education through education and training programs [22]. The study results showed the knowledge of disaster response significantly increased between the pre-test and post-test 1 and pre-test and post-test 2 in the evidence group. This program showed a significant impact on increasing nurses' knowledge in disaster response in handling psychological, psychosocial, and spiritual problems. To achieve the learning objectives in each session, the evidence group prepared several learning media such as 2 modules for nurses, power points, case scenarios, videos for each session, and quizzes at the end of each session. The preparation of learning materials was very helpful for respondents in mastering the training ourcomes. This is supported by the opinion mentioned that hardcopy and softcopy attachments of training materials could be provided to increase understanding and achieve learning outcomes [23]. On the other hand, recorded video and audio links for participants' Whatapps group were also provided. This provides an opportunity for respondents experiencing technical problems, such as internet signals and environmental factors.
The existence of this recorded material could help achieve the learning outcomes for the session. The computer-based training (CBT) could provide a significant benefit in pandemic conditions. Various methods could be used through CBT, and internet-based training (IBT), such as teaching, simulation exercises, role-play, skills practice, watching videos, and case discussions can be combined [24]. This is also supported by web-based training, which is part of the health education/promotion program and is reported to be effective in modifying health behavior, increasing knowledge and self-confidence [25, 26].
The study results reported no significant difference of knowledge between post-test 1 and post-test 2 (p-value = 0.102, α = 0.05) in the evidence group. This indicates that the information provided from this training has a constant impact on the evidence group. Furthermore, knowledge, attitudes, and skills are important elements in disaster management to ensure communities’ disasters preparedness [27]. The results of this study also supported the fact that the training program is feasible and effective in increasing the knowledge of nurses related to disaster response [19].
In this study, the statistical tests for nurses’ knowledge of disaster response in the Islamic group indicated a significant difference between the pre-test and post-test 1 (p-value = 0.000), pre-test and post-test 2 (p-value = 0.000) (p<0.05). However, there was no a significant difference between post-test 1 and post-test 2 (p-value = 0.157) (p<0.05). The statistical test reported that nurses’ knowledge of disaster response in the Islamic group with a mean rank pre-test = 75.49, post-test 1 = 81.57, and post-test 2 = 81.90 were higher than the evidence group with the mean rank pre-test = 73.96, post-test 1 = 80.55, and post-test 2 = 79.35, respectively. This interpreted that the Islamic group was significantly more effective in increasing nurses’ knowledge in disaster response than the evidence group.
The training program materials for the Islamic group consisted of disaster perceptions in an Islamic perspective, the roles and functions of Islamic-based nurses, knowledge of disaster response through Islamic-based values, Islamic attitudes in facing disaster, the principles of Islamic-based communication skills, Islamic-based method to overcome psycho-socio-spiritual problems due to disasters, actions that are blessed by Allah in serving patients, and perspective of sick from Islamic views. The training material has increased the respondents' knowledge because it is relevant and applicable to the values, religiosity, norms, and beliefs (100% Muslim). Besides, the results of this study are supported by socio-demographic of respondents, such as age with mean ± SD (32.49 ± 3.38), bachelor education (40.8%), working experience with mean ± SD (7.44 ± 3.37), and disaster training attended (28.6%). Relevant training program materials also support it with the competencies needed in caring for patients with psychological, psychosocial, and spiritual problems due to disasters or other health problems.
Disaster response skills are critical competencies for nurses as the frontline workers in disaster response [28]. In the intervention program to increase the skills of nurses in disaster response in the evidence group, the interventions used disaster response skills adopted from several literature [9, 10, 29]. Disaster response skills include communication skills, such as patient center communication, open versus closed questions, and good listening skills, educational care skills, emotional care, counseling care and skills to provide support as well as the ability to involve families engagement to the deal with patient problems. In the evidence group, it was found that there were significant differences in disaster response skills among nurses in the pre-test, post-test 1 and post-test 2.
Although it has not been supported by the Islamic-based standard operating procedures (SOPs) documents in these hospitals, the IBT-based training method is considered effective in improving the nurses’ skills due to the interesting materials and techniques provided, effective learning media, attractive and communicative videos, and case scenarios that increase the nurse's critical thinking and practical skills in analyzing cases related to the skills required by nurses. Therefore, this training has had a significant impact on improving the skills of nurses in disaster response. This is also supported by the simulation method training, which helps trainees understand the actual situation at hand. While, the skill materials in the evidence group consist of the assessment of psychological responses, fulfillment of emotional needs, communication techniques with patients, listening techniques, maladaptive responses, psychosocial care, family engagement, and handling of spiritual problems due to disasters [30]. Respondents were also provided with videos and case scenarios to achieve skills in dealing with patient problems. This case scenario guides respondents in analyzing, internalizing, and demonstrating the skills of nurses in overcoming the problems. This is supported by nurses’ skills needed in dealing with psychological problems such as patient center communication, open versus closed questions, and good listening skills [31]. At the end of each session, a quiz was also provided to ask for feedback on the mastery of the materials training delivered. This is in line with a study that explained that evaluation of computer-assisted resilience training is carried out through role-play, demonstrations and quizzes to provide feedback relevant to the individual context [24]. Furthermore, several training methods, such as case studies, workshops, tutorials, group discussions, role-plays, demonstrations, and lectures, are used in training programs [19].
Furthermore, intervention for Islamic group was adopted from the Holy Book of the Quran and the hadith of the prophet Mohammad PBUH (Peace Be Upon Him) as a way of life for Moslem society. The Qur'an is a way of life, as a revelation from God to deliver relationships with God and humans. While the hadith is all the words, deeds, provisions, and approvals of the Prophet Mohammad PBUH as the basis of Islamic law. The implementation of Islamic-based nurses’ competencies in response to the disaster was developed from both the Qur'an and the hadith.
In the Islamic group, relevant training materials for nurses’ skills consisted of an assessment of disaster victims' behavioral responses, emotional needs, Islamic-based effective communication techniques (qaulan sadida, qaulan baligha, qaulan ma'rufa, qaulan karima, qaulan layina, and qaulan maysura), Islamic-based adaptive behavior, application of Islamic values in dealing with patients' problems (prayers, dzikir (remember of God), and reciting Quran), assessment of psychosocial problems, Islamic-based emotional freedom technique, the prohibition of despair in Islam, and the principle of endeavor, prayers, and tawakkal (resignation) in Islam as an obligation for every Moslim. These materials were adopted from several previous studies and the results of the need assessment in the previous supporting qualitative studies.
The results of this training support the hospital policies for Islamic-based services in accordance with the Republic of Indonesia Law No.11, 2006 concerning the implementation of Islamic law. However, the SOPs for nursing intervention, especially for handling Islamic-based psychological, psychosocial, and spiritual problems are not available. The results of this study in the Islamic group indicate that the intervention program improves the disaster response skills of nurses in the hospitals. These results are supported by the materials that are applicable to Islamic values, relevant to nursing practices, feasible and achievable in overcoming the patients’ problems. Family engagement in patients care and effective communication techniques (qaulan baligha), and listening skills are recommended in Islam as part of noble deeds blessed by Allah.
The results of this study related to nurses’ disaster response attitudes consisted of assessment behavior, acceptance, and support for several positive attitudes shown in dealing with disaster survivors. In the evidence group, the increase in the disaster response attitude is supported by several factors, including the age of the respondents (mean = 33.9 years) with high learning motivation, training media, methods of delivering the materials with a two-way and attractive approach, and an underlying attitude in caring for the patients (caring and empathy).This study results are supported that caring is the center of nursing practice based on the values of kindness, care, compassion for oneself and others, and respect for the client's spiritual beliefs [32].
This study showed that the training program activities had changed nurses' positive attitudes in disaster response. This is supported that the positive attitude of nurses in disaster response includes listening skills to patient responses, asking closed and open questions, showing acceptance and being ready to serve patients, being a good listener on adaptive and maladaptive responses, and involving patients and families in intervention or dealing with the problems [10]. Nurses are required to have caring behavior and empathy for patients. However, the emphasis on training in the Islamic group is sincerity and calm, most importantly to create caring and empathy’ attitudes.
There were several attitudes in accordance with Islamic values in caring for disaster survivors, namely: sincerity, caring (ri'ayah), empathy (al 'adhifi), and calm (ithmi'naanun). Of these four attitudes, sincerity is the main positive attitude necessary for forming a caring attitude and empathy for patients’ care. The important points from the aspect of an Islamic-based attitude are listening, involving, accompanying, appreciating, accepting, convincing, and agreeing to the opinion of patients and their families in showing sincerity and caring [33]. This is in line with the teachings of Islam where there are several manners of hearing and speaking that regulate a person to interact with others [34].
The results of the study in the Islamic group, the existence of Islamic values and religiosity of the respondents could be a suggestion in this intervention. Several studies reported that religion and religiosity give meaning and purpose to human life [35], and religion has an element of positive suggestion to affect physiology and psychology well-being [36], reduce anxiety and pain, and improve well-being and recovery [37], the spirit is meaningful in health practice and has an impact on the healing process [38].
CONCLUSION
This study found a significant difference in knowledge, skills, and attitudes of disaster response among nurses between the pre-test and post-test 1. However, there was no significant difference between post-test 1 and 2 in the three groups, indicating that this intervention program showed constant results at the two measurements. The pre-test and post-test of nurses' knowledge, skills, and attitudes were significantly different, with the Islamic group being higher than both the evidence and control groups.The results of this study benefit to support the implementation of an appropriate Islamic-based disaster nursing responses for hospitals in the Aceh Province and other regions with the implementation of Islamic law. The study findings help the hospital policymakers establish an Islamic-based hospital disaster plan, including the policies, guidelines, training for emergencies and disaster plans, developing Islamic-based SOPs in handling psycho-social-spiritual problems due to disasters.
LIMITATIONS
This study was conducted at the peak of the COVID-19 pandemic. Several respondents had contact with COVID-19 patients and were infected. The nurses’ skills slightly decreased in post-test 2, however, remained above the baseline. In addition, all the respondents are Moslim and thus, supporting factors such as religiosity, beliefs and Islamic values of respondents may affect the results of the study. Hence, the findings could not be generalized to other areas with non-Muslim populations.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved for ethical considerations by the Ethics Committee of Dr. Zainoel Abidin Banda Aceh Hospital, with number 1171012P dated January 25, 2019.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures were followed in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
The respondents involved in this study signed written informed consent to indicate their willingness.
STANDARDS OF REPORTING
CONSORT guidelines and methodologies were followed for this study.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Researchers would like to thank all the participants for their willingness to be involved in this study. We also extend our gratitude to all hospital leaders, especially in education and training at the three hospitals in Banda Aceh, for their support. Also, we thank all research assistants for their valuable assistance in completing this study.

