All published articles of this journal are available on ScienceDirect.

Self-Leadership Practices of Nurse Educators at South African Nursing Education Institutions
Abstract
Background:
Self-leadership has emerged as a leadership style that could be used to achieve successful performance for individuals and organisations, including higher education institutions. It is, however, not known how nurse educators perceive their self-leadership practices.
Objective:
To describe the self-leadership practices of nurse educators at nursing education institutions.
Methods:
This article reports the quantitative phase of a broader exploratory, descriptive, sequential mixed-method design study conducted with conveniently selected nurse educators (n=265) in two provinces in South Africa. Data were collected using a self-administered questionnaire.
Results:
Constructs found to be valid for self-leadership practices were autonomy-supportive environment, continuing professional development, role modelling, and shared leadership. Respondents perceived themselves to be engaged in self-leadership practices. The Cronbach alpha coefficient indicated the internal consistency of the constructs.
Conclusion:
Educational institutions should create environments that support autonomy and role modelling to facilitate the engagement of nurse educators in self-leadership practices.
1. INTRODUCTION
South Africa is undergoing transformative legislative reforms that require nursing education to be positioned in the higher education band which will influence the training of nurses in the country [1, 2]. As subject and clinical experts, role models, mentors, project managers, and leaders in their communities, nurse educators will play a vital leadership role in the implementation of these reforms. Besides being influential in training and producing nurses, nurse educators also need to be visible leaders who influence and drive policy reforms and engage in professional forums, research, and scholarship [3, 4]. Thus, there is a call for a new way of leadership in nursing education institutions that ensures organisational success during these reforms whilst simultaneously contributing to the improvement of the functioning of the country’s health systems [5, 6]. Self-leadership has emerged as a leadership style that could be used to achieve successful performance for the individual and the organisation [7, 8]. Goldsby and colleagues challenge managers in nursing to practice self-leadership to enhance their own performance as well as improve their workplaces by utilising skills such as self-awareness, positive self-talk, and visualisation [9]. The difference between the self-leadership of managers in a clinical setting and that of nurse educators the pedagogical setting in which nurse educators find themselves; they are the first ones to respond to the expectation of disseminating knowledge to students [10].
Nurse educators that utilise self-leadership are driven by motivation and demonstrate self-influence to direct themselves towards achieving optimum performance [11, 12].
However, some authors have noted that there are nurse educators whose behaviours do not resemble the self-leadership attributes: they resist new changes in nursing education, detest innovations and no longer have the motivation to teach; while some go to class unprepared, and some victimise and harass students and their colleagues verbally and emotionally [13-15]. These unfortunate behaviours by nurse educators do not only lead to poor working relations with their colleagues but can also lead to students leaving the course or the nursing profession altogether [16].
Based on the background above, the following research question arose:
What are the self-leadership practices of nurse educators in nursing education institutions?
The study aimed to respond to this question by describing how nurse educators perceive their self-leadership practices at nursing education institutions. It drew on Manz’s theoretical framework on self-leadership, namely the Expanded theory of self-influence processes in organisations [17]. This theoretical framework provides a comprehensive listing and review of the various self-leadership strategies from which most literature on self-leadership is based [18].
The practice of self-leadership is described as engagement of the self in a variety of activities that are not only targeted at motivating the self but also as an act of deliberately improving the environment to such an extent that it influences other team members to become motivated and committed to their work [19].
The concept of self-leadership is based on the assumptions of the social-cognition theory as well as theories of self-control, self-regulation, and self-management, which focus predominately on behavioural strategies [18]. Self-leadership strategies, which include behavioural and mental techniques, are designed to positively influence individual effectiveness. These strategies are divided into three categories: behaviour-focused strategies, natural reward strategies, and constructive thought pattern strategies [8]. Behaviour-focused strategies improve an individual’s self-awareness where individuals take a conscious decision to monitor their own behaviour and are aimed at nurturing behavioural management [20, 21]. Natural reward strategies are about an individual’s search and promotion of pleasant experiences during goal-striving activities [21, 22]. Constructive thought pattern strategies facilitate the generation of habitual thinking that positively influence the performance of an individual [21, 22].
Some literature has identified the following as self-leadership practices of educators in mainstream education: self-reflection, self-goal setting, self-control, self-development, role modelling, and collaboration [23-27]. However, owing to the dearth of specific literature on nurse educator self-leadership, there was a need for exploration of self-leadership practices by nurse educators themselves to get a comprehensive understanding of the concept, how it is practiced [28], and how it can be facilitated [21, 29].
2. MATERIALS AND METHODS
2.1. Design, Setting, and Sample
This study employed an exploratory, descriptive, sequential mixed-method design, which had three phases. Phase 1 consisted of two subphases: subphase 1 entailed conducting an integrative literature review to explore and describe the concept of self-leadership of nurse educators and subphase 2 entailed conducting semi-structured focus group interviews with nurse educators from a selected group. Phase 3 entailed the development and validation of guidelines to facilitate self-leadership in nurse educators. This article reports on phase 2, which focused on obtaining information about the self-leadership practices of nurse educators through structured questionnaires.
The population was nurse educators teaching in purposively selected private nursing schools, public nursing colleges, and universities in the Gauteng and KwaZulu-Natal provinces in South Africa. The nursing education institutions in the two provinces consistently had high outputs of registered nurses and midwives for the years 2009-2018.
Convenience sampling was used to recruit nurse educators appointed on a full-time basis at the remaining nursing education institutions in the two provinces, who were not included in the qualitative phase of the study. Participation was voluntary and anonymous, and no incentives were offered. The total number of possible respondents was 443, of whom 265 (59.8%) responded.
2.2. Questionnaire Development and Data Collection
A questionnaire was compiled based on the themes that emerged from phase 1 (subphase 1 and subphase 2) and the literature to determine the self-leadership practices of nurse educators in nursing education institutions. This data collection approach is typically that of a sequential mixed-methods study because one set of data would be building on the other [30]. The questionnaire comprised four sections: Section A was designed to elicit the biographical information of nurse educators who participated in the study; Section B comprised questions that attempted to ascertain the nurse educators’ understanding of the concept of self-leadership and its constructs; Section C comprised questions that attempted to determine the self-leadership practices of nurse educators; Section D comprised questions that attempted to ascertain how motivation could influence self-leadership. Some of the questions were further explored by asking open-ended questions to obtain richer information. The questionnaire used a seven-point Likert scale with the responses ranging from strongly disagree (1) to strongly agree (7). This article focuses on findings based on data collected in Sections A and C of the questionnaire. The hand-delivered structured questionnaires were distributed and collected by the researcher between 2018-2019. Sealed and lockable boxes were used to collect the questionnaires from the respondents. Each questionnaire was accompanied by an information leaflet that described the purpose of the study and the ethical issues related to the participation in the study.
2.3. Internal and External Validity
Rigour of the study was ensured through validity and reliability. In order to ensure the validity of the instrument, content validity, face validity, and construct validity were measured. Content validity was established through an integrative literature review, discussions, and consultations with the study supervisor to evaluate the relevance of the questions to the subject. Pre-testing of the questionnaire and coding of the question items by a statistician also improved the content validity of the instrument. Face validity was established using the statistician and nurse educators who were not part of the study to review the questionnaire and identify questions that were difficult to interpret and answer.
Construct validity was established by incorporating the theoretical framework and integrative literature review on self-leadership into the questionnaire.
Reliability was enhanced by carefully designing, pre-testing, and checking the questionnaire. Bell and colleagues describe the Cronbach-alpha test as a commonly used test to determine internal reliability [31]. In this study, a Cronbach’s alpha coefficient of 0.6 was used to determine the reliability of the tool. The closer the Cronbach’s alpha is to 1, the higher the internal consistency reliability [31].
3. DATA ANALYSIS
The unprocessed data from the participants (n=265) were coded and entered into a Microsoft (MS) Excel (Windows 2016) spreadsheet and analysed by a statistician, using the descriptive SPSS Version 25 statistical package [32]. Specifically, the statistical techniques used were the exploratory factor analysis for the validity of the constructs and the Cronbach Alpha Coefficient for the reliability of the constructs. The exploratory factor analysis technique is purported to be highly sensitive to the sample size and less stable when estimated from small samples [33]. However, the author, after consultation with the second author and the statistician, was satisfied with the overall number of returned questionnaires (n=265). The interpretation of exploratory factor analysis was based on rotated factor loadings, rotated eigenvalues, and a screentest [33].
Descriptive statistics were used to synthesise and describe data, using parameters such as means, frequencies, and percentage distributions [34]. The data were presented by means of frequencies, tables, and histograms.
The exploratory factor analysis was applied to the responses of the self-leadership activities subscale. The maximum likelihood method was used to extract the factors, followed by a varimax (orthogonal) rotation. The criteria used to determine the number of factors for rotation is discussed in 5.2.
4. RESULTS
4.1. Biographical Data
Table 1 below presents a summary of biographical data of the respondents, namely gender, age, and type of nursing education institution. Where not all respondents responded to items such as age, the authors calculated the frequencies and percentages according to the number of responses. Therefore, missing values were not included but were indicated in the tables.
| Demographic Features | ||
|---|---|---|
| Frequency | Percentage | |
| Gender (n=265), Missing=0 | ||
| Female | 250 | 94 |
| Male | 15 | 6 |
| Total | 265 | 100 |
| Age (n=263), Missing =2 | ||
| 21-30 | 9 | 3.42 |
| 31-40 | 35 | 13.31 |
| 41-50 | 79 | 30.04 |
| 51+ | 140 | 53.23 |
| Total | 263 | 100 |
| Type of Nursing Education Institution (n=265), Missing=0 | ||
| Public Nursing College | 178 | 67 |
| Private Nursing School | 60 | 23 |
| University | 27 | 10 |
| Total | 265 | 100 |
Only 15 (6%) respondents were males. Males are a minority in the nursing profession, which is generally dominated by females according to Smith and colleagues [35]. Thus it was not unexpected that females responded to the questionnaire more frequently than males.
The age bracket with the lowest number of respondents was that of 21–30 years at nine (3.4%) and the age bracket with the largest number of respondents was that of ages 51 or older, which comprised 140 (53.2%) respondents, which means that more than half of the respondents were older than 51-years. Some authors have observed that nurse academics are becoming redundant, which may impact the country’s ability to educate and produce next generation nurses [36, 37].
As depicted in the table, 178 (67%) of the respondents were teaching at public nursing colleges, 60 (23%) taught at private nursing schools, and 27 (10%) taught at universities.
4.2. Validation of Constructs for the Subscale: Self-Leadership Activities
Exploratory factor analysis was applied to the responses of the self-leadership activities subscale. The maximum likelihood method was used to extract the factors, and this was followed by a varimax (orthogonal) rotation. The following criteria were used to determine the number of factors to be used for rotation: cumulative percentage variance greater than 50%; Eigen value greater than 1; and a significant decline in the scree plot. In interpreting the rotated factor pattern, an item was said to load on a given factor if the factor loading was 0.40 or greater for that factor and less than 0.40 (absolute value) for the other factors in the rotated factor matrix, as depicted in Table 2. The factor loadings that were 0.40 or greater are highlighted in bold.
Five factors exhibited with Eigen values above 1 and 50.9% of cumulative variance. The results of a scree plot also suggested that the five factors were meaningful. Thus, the five factors were retained for rotation. Table 2 below displays the matrix of rotated factor loadings for the subscale: self-leadership activities.
Table 2.
| Item No. | Items | Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 |
|---|---|---|---|---|---|---|
| C70 | It is my belief that nurse educators should be involved in the decision-making processes of the nursing education institution. | 0.83 | 0.06 | 0.10 | 0.15 | 0.04 |
| C71 | In my opinion the nursing education institution should support nurse educators’ innovation and creative behaviours. | 0.73 | 0.07 | 0.18 | 0.33 | 0.02 |
| C67 | Nurse educators have a responsibility to instil professional ethics and values in their students. | 0.72 | 0.13 | 0.18 | -0.0 | 0.17 |
| C68 | Leaders in a nursing education institution should be passionate, inspirational and build self-confidence in nurse educators. | 0.66 | 0.16 | 0.13 | 0.04 | 0.42 |
| C72 | In my opinion nurse educators are change agents who advocate for the transformation of the broader community. | 0.64 | 0.33 | 0.05 | 0.26 | 0.08 |
| C75 | Nursing education institutions should send nurse educators to training programmes that stimulate their self-leadership | 0.58 | 0.07 | 0.20 | 0.39 | -0.1 |
| C69 | The leaders in nursing educations institutions should give nurse educators room for failure and encourage them to take risks. | 0.43 | 0.06 | 0.12 | 0.14 | 0.06 |
| C74 | Rigid bureaucratic leadership systems and autocratic leadership styles prevent nurse educators from engaging in self-leadership activities. | 0.37 | 0.12 | 0.13 | 0.10 | -0.1 |
| C47 | I identify my own learning needs for self-development based on the current and future health and education trends. | 0.14 | 0.62 | 0.29 | 0.24 | -0.0 |
| C48 | I take time to reflect on how my work contributes to the improvement of student performance in the nursing education institution. | 0.04 | 0.58 | 0.15 | 0.07 | 0.00 |
| C46 | In my opinion, it is the responsibility of the individual nurse educator to engage in his or her own professional development. | 0.09 | 0.58 | 0.10 | 0.14 | 0.02 |
| C51 | I take time to reflect on my teaching behaviour and actions with the aim to make positive improvements and meaningful change. | 0.07 | 0.57 | 0.28 | 0.01 | 0.11 |
| C50 | In my opinion, engagement in continuing professional development (CPD) activities that are relevant to my area of work could facilitate my self-leadership. | 0.26 | 0.50 | 0.20 | 0.36 | 0.04 |
| C54 | Nurse educators should take time to research new information and developments in their areas of teaching. | 0.21 | 0.45 | 0.30 | 0.13 | 0.41 |
| C60 | I am a team worker who engages in sharing ideas and resources with fellow nurse educators. | 0.25 | 0.43 | 0.16 | 0.33 | 0.28 |
| C73 | I consider myself as a change agent who advocates for the transformation of the nursing education system. | 0.31 | 0.32 | 0.01 | 0.17 | 0.17 |
| C56 | Nurse educators should endeavour to meet deadlines on their tasks. | 0.18 | 0.24 | 0.60 | 0.13 | 0.08 |
| C59 | Nurse educators should give timeous feedback to the students on their performance. | 0.29 | 0.16 | 0.53 | 0.26 | 0.01 |
| C57 | Nurse educators should adhere to teaching schedules (timetables). | 0.05 | 0.13 | 0.52 | 0.08 | 0.09 |
| C55 | In my opinion nurse educators should strive to commence their work on time. | 0.11 | 0.23 | 0.52 | 0.04 | 0.11 |
| C58 | Nurse educators should develop lesson plans in their preparations for teaching. | 0.13 | 0.12 | 0.47 | 0.30 | -0.0 |
| C66 | Nurse educators should promote ethical attitudes towards colleagues, students and in society. | 0.25 | 0.29 | 0.42 | 0.33 | 0.11 |
| C52 | In my opinion, nurse educators should regard themselves as co-learners who consider suggestions from students during the teaching and learning process. | 0.29 | 0.28 | 0.31 | 0.12 | 0.30 |
| C49 | I endeavour to be a resourceful role model who embodies the values and image of the nursing profession to my colleagues and students. | 0.09 | 0.03 | 0.10 | 0.07 | 0.05 |
| C65 | It is my opinion that nurse educators should be involved in succession planning to ensure continuity in key leadership positions and retain intellectual and knowledge capital. | 0.27 | 0.15 | 0.10 | 0.64 | 0.12 |
| C61 | In my opinion, collaboration between nurse educators in the nursing education institution should be encouraged. | 0.18 | 0.21 | 0.18 | 0.62 | 0.23 |
| C53 | In my opinion, nurse educators should request feedback on their performance from significant others in the nursing education institution. | 0.20 | 0.18 | 0.22 | 0.42 | 0.02 |
| C64 | It is my opinion that in the absence of designated mentors, nurse educators should be initiative and find resources to read, research and observe colleagues in order to develop the necessary teaching skills. | 0.33 | -0.0 | 0.15 | 0.35 | 0.26 |
| C62 | In my opinion, a nurse educator should assume the leadership role when the supervisor is not available to provide leadership. | 0.07 | 0.10 | 0.09 | 0.28 | 0.08 |
| C63 | In my opinion, the institution should provide new nurse educators with mentors. | 0.02 | 0.05 | 0.11 | 0.31 | 0.58 |
Six items loaded on the first factor labelled “autonomy-supportive environment”; six items loaded on the second factor labelled “continuing professional development”; six items loaded on the third factor labelled “role modelling”; three items loaded on the fourth factor labelled “shared leadership”; and one item loaded on the fifth factor, possibly labelled “mentoring”.
Item C68 that was cross-loaded for factor 1 and factor 5 was not retained for any of the two factors. Although it loaded the highest on factor 1, it did not make logical sense, nor would it make logical sense if retained in factor 5.
Similarly, item C54 which was cross-loaded for factor 1 and factor 5 at 0.45 and 0.40, respectively, was not retained for either of the factors. The fifth factor in this subscale had two items, which were cross-loaded with other factors in the rotated factor matrix and these items were not retained. As a result, there was only one item, C63, which was about the institution providing new nurse educators with mentors, remaining under factor 5. Since factor 5 only had one item, a score could not be calculated.
4.3. Reliability Testing on Self-Leadership Activities
Table 3 below presents the results from the analysis of the questionnaire subscale of self-leadership activities. As depicted in the table, the reliability testing was measured on the items that loaded as follows: six items loaded on the first factor labelled “autonomy-supportive environment”; six items loaded on the second factor labelled “continuing professional development”; six items loaded on the third factor labelled “role modelling”; and three items loaded on the fourth factor labelled “shared leadership”. The Cronbach alpha coefficient of all the factors was greater than 0.6, which means that the items of the constructs were reliable. Thus, the results indicate the internal consistency of the self-leadership activities.
4.4. Determining the Self-Leadership Activities Subscale Composite Scores
The responses on the questionnaire ranged from a 1, strongly disagree, to a 7, strongly agree. The composite construct scores for factors in the subscales were calculated by taking the average of the reliable items that loaded onto that factor. Histograms were used for showing distribution and descriptive statistics. Distribution was considered skew if the skewness value was outside the range of -1 and +1. Where the distribution was skew (skewness outside the range of -1 and +1), the median was used in the interpretation of results.
The composite scores of each of the constructs for subscale self-leadership activities are discussed below:
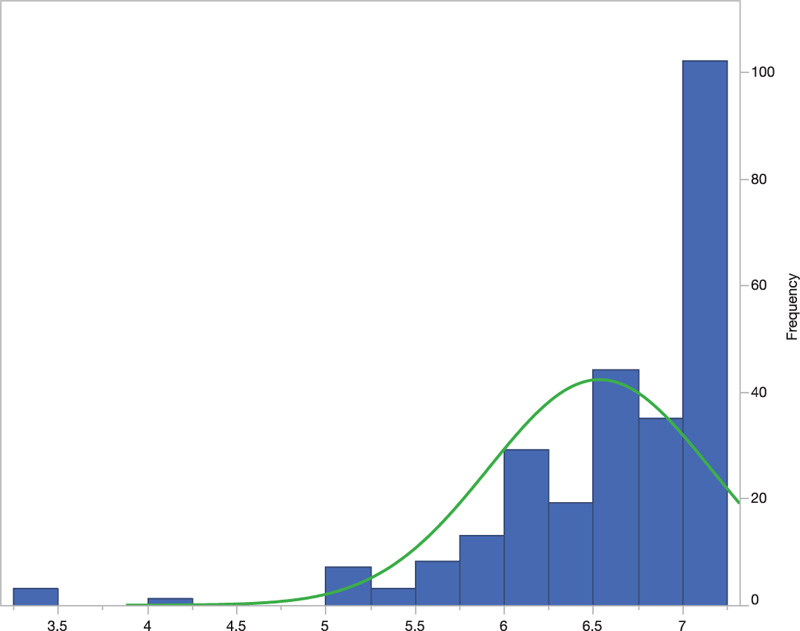
4.4.1. Construct 1: Autonomy-Supportive Environment (Items C67, 69, 70, 71, 72, 75)
The composite construct “autonomy-supportive environment” measured whether nurse educators perceived that the nursing education institution and its management provided an environment that facilitated self-leadership by providing autonomy-related aspects, such as giving nurse educators room for failure and encouraging them to take risks; involving nurse educators in decision-making processes; supporting them in innovative and creative behaviours and empowering nurse educators by sending them to training programmes that stimulate their self-leadership.
Fig. (1) below depicts the distribution of composite scores on the construct “autonomy-supportive environment”. The composite scores for each respondent ranged from 3.3 to 7 (maximum score). The histogram shows a skewed distribution of composite scores to the left (negatively skewed), with a skewness value of -2.28 and a mean of 6.54. Therefore, a median of 6.8 was used for interpretation. The median (6.8) is greater than the mean of 6.54, with a standard deviation of 0.62. This means that the respondents perceived that an autonomy-supportive environment could facilitate self-leadership by strongly agreeing with this construct.
| Subscale | Constructs | Items | Items left out | Cronbach | Reliability |
|---|---|---|---|---|---|
| Self-leadership practices | Autonomy-supportive environment | C67, 69, 70, 71, 72, 75 | None | 0.82 | Good reliability |
| Continuing professional development | C46, 47, 48, 50, 51, 60 | None | 0.78 | Acceptable reliability | |
| Role modelling | C56, 59, 57, 55, 58, 66 | None | 0.75 | Acceptable reliability | |
| Shared leadership | C61, 65, 53 | None | 0.69 | Acceptable reliability |
4.4.2. Construct 2: Continuing Professional Development (Items C46, 47, 48, 50, 51, 60)
The composite construct “continuing professional development” mainly measured whether the nurse educators believed that it was their responsibility to engage in their own professional development and whether they believed that engagement in continuing professional development activities that are relevant to their area of work could facilitate their self-leadership.
Fig. (2) below depicts the distribution of composite scores on the construct “continuing professional development”. The composite scores for each respondent ranged from 2.3 to 7 (maximum score). The histogram shows a skewed distribution of composite scores to the left (negatively skewed) with a skewness value of -1.85 and a mean of 6.36. Therefore, a median of 6.5 was used for interpretation. The median (6.5) is greater than the mean of 6.36, with a standard deviation of 0.659. This means that the respondents perceived that they should engage in continuing professional development because it was an intervention that would motivate them to engage in self-leadership by strongly agreeing with this construct.
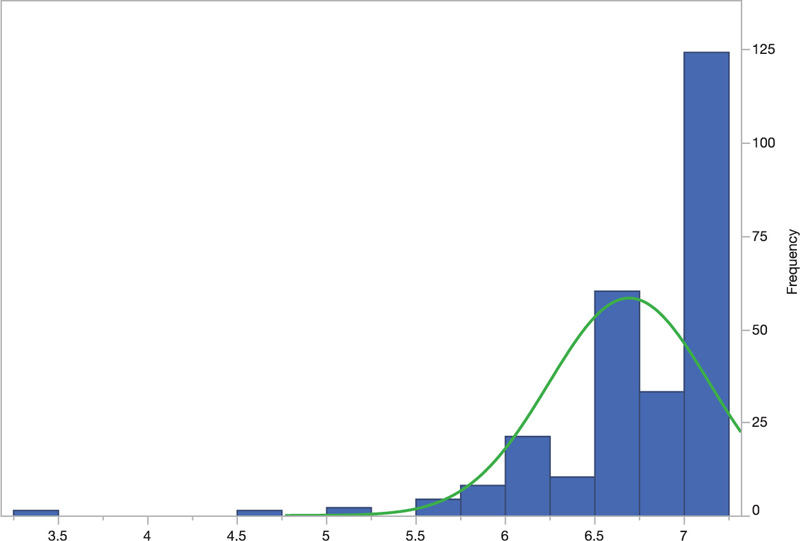
4.4.3. Construct 3: Role Modelling (Items C56, 59, 57, 55, 58, and 66)
The composite construct “role modelling” measured the nurse educators’ perceptions of aspects perceived as promoting role modelling to students and colleagues. The aspects related were meeting deadlines on tasks, giving timeous feedback to the students, adhering to teaching schedules (timetables), commencing with work on time, developing lesson plans in their preparations for teaching, and promoting ethical attitudes towards colleagues, students, and society.
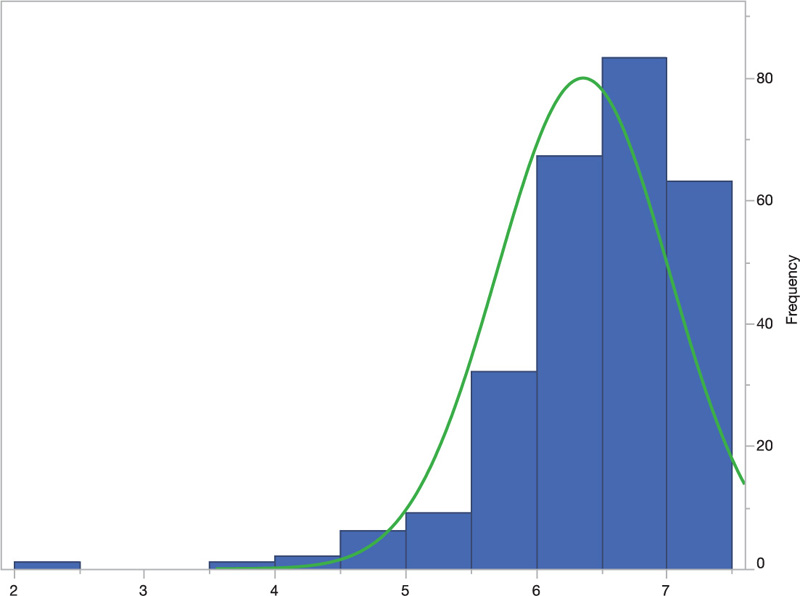
Fig. (3) below depicts the distribution of composite scores on the construct “role modelling”. The composite scores for each respondent ranged from 3.3 to 7 (maximum score). The histogram shows a skewed distribution of composite scores to the left (negatively skewed) with a skewness value of -2.79 and a mean of 6.7. Therefore, a median of 6.8 was used for interpretation. The median (6.8) is greater than the mean of 6.7, with a standard deviation of 0.452. This means that the respondents perceived that role modelling in the nursing education institution facilitated self-leadership by strongly agreeing with this construct.
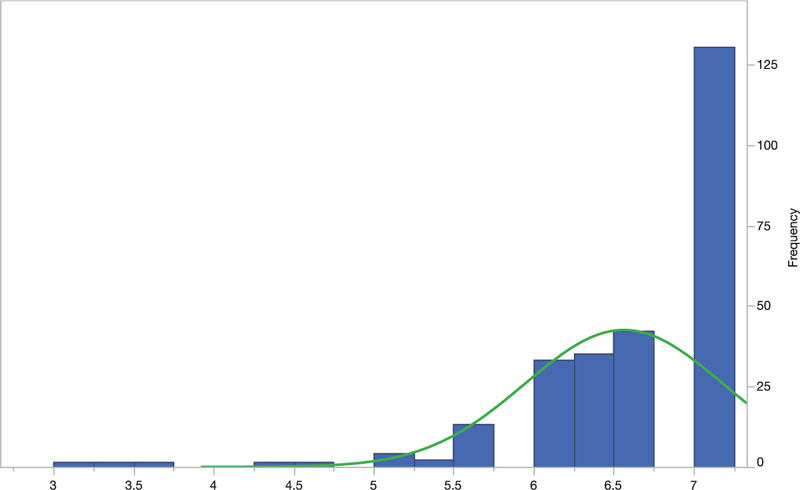
4.4.4. Construct 4: Shared Leadership (Items C61, 65, 53)
The composite construct “shared leadership” measured the nurse educators’ perspectives as to whether shared leadership through collaboration, succession planning, and feedback on performance could facilitate self-leadership. Fig. (4) below depicts the distribution of composite scores on the construct “shared leadership”. The composite scores for each respondent ranged from 3 to 7 (maximum score). The histogram shows a skewed distribution of composite scores to the left (negatively skewed) with a skewness value of -2.34 and a mean of 6.56. Therefore, a median of 6.6 was used for interpretation. The median (6.6) is greater than the mean of 6.56, with a standard deviation of 0.619. This means the respondents perceived that self-leadership could be facilitated through shared leadership in the nursing education institutions by strongly agreeing with this construct.
4.5. Comparison of the Constructs: Subscale Self-leadership Activities
Table 4 below depicts a comparison of the minimum and maximum composite construct scores, their average mean, median, and standard deviation for the subscale self-leadership activities.
| Construct | N | Minimum | Maximum | Mean | Median | Std Dev |
|---|---|---|---|---|---|---|
| Autonomy-supportive environment | 264 | 3.0 | 7 | 6.54 | 6.8 | 0.620 |
| Continuing professional development | 264 | 2.3 | 7 | 6.36 | 6.5 | 0.659 |
| Shared leadership | 264 | 3.0 | 7 | 6.56 | 6.6 | 0.619 |
| Role modelling | 264 | 3.3 | 7 | 6.69 | 6.8 | 0.450 |
Table 4. Summary of construct composite scores for subscale self-leadership activities.
The comparison in Table 4 above indicates that the minimum construct score for all the constructs under the subscale self-leadership activities was for “continuing professional development” at 2.3, and the maximum construct score was 7 for all constructs. Both “autonomy-supportive environment” and “role modelling” had the highest median at 6.8, which means that of all the constructs in the subscale self-leadership activities, the respondents had a more positive perception of the constructs, “autonomy-supportive environment” and “role modelling”. The construct with the lowest median in the subscales was “continuing professional development” at 6.5, meaning that this construct was less important for the respondents when compared to the others in this subscale.
4.6. Open-Ended items on Self-Leadership Practices
The questionnaire had open-ended items (items 67; 68; 69) in Section C on self-leadership practices (activities).
The questionnaire had 67, 68, and 69 as follow-up items with open-ended questions that explored certain self-leadership practices (activities) and related aspects. In item 67, the respondents were requested to justify why collaboration between nurse educators at a nursing education institution should be encouraged. Of the 206 that responded, 71 (34%) indicated that collaboration facilitated the sharing of ideas, experiences, and best practices, leading to a change in individuals’ teaching practices. A total of 40 (19%) respondents indicated that collaboration helped improve relations and understanding among nurse educators, thus ensuring that nurse educators worked towards a shared common goal.
In the literature, the management of the educational institution is expected to encourage quality and well-structured and resourced collaboration in teams to improve the teaching performance of the educators, students’ achievements, and ultimately the institution [38]. An academic institution could promote self-leadership by creating a supportive atmosphere conducive to collaborative learning, innovation, and creativity, which may ultimately lead to improved student performance [39]. However, it is the responsibility of the individual nurse educator to proactively seek out and take advantage of available collaborative resources in the institution [38].
With regard to item 68, respondents had to indicate examples of training programmes that stimulate their self-leadership. Of the 150 that responded, 121 (81%) respondents listed training programmes related to their continuing professional development needs for effective curriculum delivery, such as innovative teaching strategies, discipline-specific courses, updates on clinical practice, research, and e-learning. Thirty-two (21%) respondents listed training programmes related to self-awareness and emotional intelligence, such as time management, mentoring, project management, personal development, and self-leadership strategies.
In item 69, the respondents were required to indicate which supervisor leadership styles could enhance the nurse educators’ self-leadership. The respondents indicated their preferences of supervisor leadership styles as follows: democratic: 104 (52%); participative: 45 (23%); transformational: 44 (22%); situational: 18 (9%); and autocratic leadership: 16 (8%). Katewa and Heystek (2019) [40], as well as Kolzow (2014) [41] assert that leaders that enhance the self-leadership of their educators are those that use the democratic and participative leadership styles, since these leadership styles emphasize the inclusion of followers in consultation and decision-making, as well as teamwork, and setting a good leadership example fortheir educators by leading from the front. The leaders’ transformational leadership enhances idea generation, exploratory thinking, creativity, and the innovative ideas of educators [42, 43]. However, autocratic leadership was not the preferred leadership style in literature since this style does not promote that consultation and decision-making resides with the leader; thus, undermining educator motivation and performance [44, 45].
5. DISCUSSION
The article sought to determine the self-leadership practices of nurse educators at nursing education institutions. The evidence showed that the nurse educators perceived self-leadership in their respective institutions. The respondents perceived that an “autonomy-supportive environment” could facilitate self-leadership. This finding is supported by Kör (2016) [46], who found that autonomy supportive environment supports innovativeness, risk-taking, and proactivity in self-leading individuals. Individuals are more autonomously motivated, perform and learn better, and be better adjusted in their engagement in self-leadership when they understand the value and purpose of their jobs, feel ownership and autonomy in carrying them out, and receive clear feedback and support, according to Hagger et al. [47].Academic leaders could create an autonomy-supportive environment that promotes the self-leadership of educators by taking an interest in their views, providing opportunities for choice and participation, encouraging self-initiation, and avoiding the use of external rewards or sanctions as ways to motivate behaviour [48, 49].
The results also showed that engagement in “continuing professional development” was also perceived to be a self-leadership activity that could facilitate self-leadership. Gil et al. found that the institution has a role to play in supporting educators to keep up with the pace of contemporary changes [50]. An institution can develop an individual’s self-leadership attributes by creating a continuous learning environment that encourages staff to try out new ideas, thoughts, and practices [49, 50]. The newly acquired knowledge can then be used to improve student performance. Continuing professional development enhances self-reflection and self-evaluation of the educator and brings a change in attitudes while interacting with students and colleagues [51, 52].
Respondents in this study also perceived that self-leadership could be facilitated through “shared leadership” at the institutions. Jovanović et al. purport that self-leadership and shared leadership complement each other in that to be effective self-leaders who can influence others in teams, and individuals must have self-awareness, should self-reflect to understand their influence on others and develop the ability to self-control, self-regulate, and manage themselves [53]. Davoudi et al. found that shared leadership stimulated knowledge creation among university academics [54]. Stirling (2016) [55] purports that when academic managers encourage shared leadership, the educational institutions become non-threatening environments that support mutual ownership of the educational culture, autonomy, competence, and relatedness. Thus, the educational institution should strive to facilitate self-leadership through the removal of rigid bureaucratic leadership systems and autocratic leadership styles. These ineffective styles should be replaced with supportive leadership styles that would facilitate their self-leadership through involvement in decision-making processes, giving nurse educators the platform to participate and verbalise their views in the institution [56, 57].
“Role-modelling” was perceived to be facilitative to the self-leadership of colleagues and students. According to Ghosh (2021) [39], an organisation can promote individual employees’ self-leadership attributes by systematically exposing them to role modelling. Peers emulate educators who demonstrate expert subject knowledge and pedagogical competence, whose teaching is innovative, engaging, and learner-centred, thus exemplifying relatedness and autonomy [58, 59]. Jack and colleagues found that nurse educators value the credibility, prestige, and trustworthiness of the person being modelled [60]. Such role models are often emulated for their critical thinking, consistency, and integrity in their practice of teaching, academic honesty, flexibility, and respect for students and peers [10].
On the other hand, students value nurse educators who demonstrate a sound clinical knowledge base, have the ability to facilitate effective learning and possess the ability to relate to students on an interpersonal level as role models [60, 61]. Nursing skills are learnt through positive role modelling during both theory and clinical training of students [60, 62]. Thus, nurse educators, including clinical preceptors, should be trained on self-leadership skills and always be mindful that they are being observed by students on an ongoing basis so as not to underestimate the effect their actions and behaviours have on student nurses.
The study has a limitation in that it was conducted in nursing education institutions across two of the nine provinces in South Africa, namely, Gauteng and KwaZulu-Natal. Therefore, the findings of the study cannot be generalised beyond these provinces but could be applied to other institutions in the remaining provinces.
CONCLUSION
The educational institution has a role in facilitating self-leadership practices by nurse educators. Thus, self-leadership practices should not be confined to nurse educators only, but institutions should also strive to improve the self-leadership skills of academic managers. It is recommended that further research be conducted into the following issues that emerge in practicing and facilitating self-leadership in nurse educators: (1) identifying self-leading nurse educators and auditing how their practices improve the performance of student nurses, and (2) further exploration of the concept autonomy-supportive environment, that emerged as a construct, in relation to intrinsic motivation and its effect on nurse educator self-leadership
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This article is derived from a doctoral thesis in health studies. Ethical clearance (REC-012714-039) was sought from the Research and Ethics Committee at the University of South Africa before the study was conducted.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures were followed in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Written informed consent was obtained from all participants when they were enrolled.
STANDARDS OF REPORTING
STROBE guidelines and methodologies were followed for this study.
AVAILABILITY OF DATA AND MATERIALS
The data that support the findings of this study are available from the corresponding author, [V.E.M], on special request.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
FUNDING
None.
ACKNOWLEDGEMENTS
We wish to thank Mr. Hennie Gerber for his assistance with the statistical analysis.

