All published articles of this journal are available on ScienceDirect.

Investigation of Contacts for Latent Mycobacterium Tuberculosis Infection: Application Software Development
Authors Info & Affiliations
Abstract
Introduction:
Tuberculosis is a pathology that continues to be worthy of special attention from health professionals and society due to its high prevalence, proving to be a crucial public health problem.
Objectives:
To describe the development of an application for family health strategy professionals’ investigation of tuberculosis contacts for Latent Mycobacterium tuberculosis Infection.
Methods:
This study is applied research on an application software developed according to three of the five phases described by Falkembach for developing digital educational materials, which include analysis and planning, modeling, and implementation.
Results:
The application is dynamic; that is, it guides health professionals through sequenced screens according to professionals’ self-informed answers. This functionality helps them deciding whether to proceed to the treatment of the patient with Latent Mycobacterium tuberculosis Infection or returning to the initial stage of a tuberculosis contact.
The screens of the application follow the flowchart presented in the Ministry of Health’s Manual of recommendations for tuberculosis control in Brazil of 2018.
Conclusion:
The application developed to guide Family Health Strategy professionals regarding Latent Infection by Mycobacterium Tuberculosis can prevent human errors and increase the care quality when assessing tuberculosis contacts.
1. INTRODUCTION
Tuberculosis (TB) is still a significant public health problem, although there is a governmental commitment to surveillance and control strategies for this disease [1-3]. Worldwide, there are approximately 10.4 million new TB cases each year. Some of the regions that are most at risk for this illness are Africa and Asia. India, Indonesia, China, Pakistan, and the Philippines account for 56% of the new cases [4], while the Democratic People’s Republic of Korea, Lesotho, Mozambique, the Philippines, and South Africa has the highest incidence rate, with more than 500 new cases per 100,000 inhabitants [5].
About a quarter of the world’s population has Koch’s bacillus but does not show any signs of active TB [6]. This condition is known as Latent Tuberculosis Infection (LTBI), i.e., a state of the persistent immune response to stimulation by Mycobacterium tuberculosis antigens without evidence of clinically manifested active TB [7]. It is noteworthy that not all individuals infected with Mycobacterium tuberculosis will become ill, that is, developing the active form of the disease; most of them remain in the latent phase, constituting a large reservoir of individuals with LTBI. Most cases that progress to the active disease occur in the first 2 to 5 years after the first infection, but the latency period can extend for many years [7].
In the United States, the estimates for LTBI reactivation account for more than 80% of new TB cases when compared to the rapid progression of recent infection [8, 9]. In Brazil, due to the lack of information, standardization in data collection, and LTBI surveillance in some Brazilian regions, the data gathered on LTBI do not represent the epidemiological panorama [10]. Still, it is important to highlight that Brazil occupies the 20th position in the 30 countries, considered a priority for TB control [11].
Asian countries also lack standardized reports on LTBI and specific data for this infection. Furthermore, most notification systems in Brazil were designed to report active TB. For this reason, they may be inadequate to record cases of LTBI [12]. Therefore, there is active TB screening, but the investigation of contacts has been neglected or below expectations.
The investigation of contacts aims to identify and treat cases of early-stage TB and latent infection. This procedure prevents the disease from developing in contacts and interrupts the TB chain of transmission. Therefore, analysing the interactions between index cases and their contacts can delineate new disease control strategies [13].
The evaluation of contacts’ degree of exposure should be individualized, taking into account the source’s case disease form, patient’s environment, and time of exposure. In addition to cases of contact with active pulmonary TB, people living with HIV and health professionals also require attention in LTBI screening. The former group is at increased risk of developing the disease because of the immune response, and the second is regularly exposed to infected people, which can increase the risk of developing the active disease [10].
In Asian countries, there is a limited number of well-trained professionals on (LBTI investigation), and they considered it difficult to adopt WHO’s updated guidelines for LTBI [14-16]. A study conducted in Nepal found that health professionals' knowledge and general practices regarding TB infection control were not satisfactory [17]. In Brazil, the factors limiting TB control at Primary Health Care (PHC) level include professionals’ frail commitment to control actions, centralized vertical processes of control within PHC, professionals turnover, poor professional training, the need for better articulation between health care units, and weaknesses related to TB control strategies [18, 19].
In view of the above, this study describes the development of a mobile application for Family Health Strategy (FHS) professionals to investigate tuberculosis contacts for Latent Tuberculosis Infection. The application is evidence-based and aims at guiding professionals working at the Unified Health System on TB contacts investigation; thus, it contributes to the pillars of LTBI surveillance in Brazil and to meet goal 3.8 of the Sustainable Development Goals (SDGs), which aims at achieving universal health coverage, including financial risk protection, and is complementary and inseparable of the TB control.
The pillars of LTBI surveillance are five: (1) identification of people most likely to have LTBI or at higher risk to the illness; (2) identification of people with LTBI; (3) appropriate treatment and follow-up; (4) notification of people carrying out the LTBI treatment; and (5) follow-up and evaluation of LTBILTBI treatment [11].
2. MATERIALS AND METHODS
2.1. Type of Study
This study is applied research on a mobile technology developed for FHS professionals investigating TB contacts for LTBI. Three of Falkembach’s five phases for developing digital educational materials were followed, i.e., analysis and planning, modeling, and implementation [20].
2.1.1. First Step
For the analysis and planning phase, we carried out the requirements definition, the app conceptual map, the choice of technology, and the content development. In this stage, we chose international and national guidelines on LTBI: Latent TB Infection: Updated and consolidated guidelines for programmatic management [7], Protocol for surveillance of latent tuberculosis infection in Brazil [10], and Manual of recommendations for the control of tuberculosis in Brazil [21].
In addition to following the guidelines, we conducted a descriptive qualitative study with FHS professionals from a Northeastern Brazilian capital to identify the difficulties in screening LTBI. It included physicians and nurses of both genders working in the FHS of the Municipal Health Foundation. Professionals on vacation, medical leave, or maternity leave were excluded.
A semi-structured interview was used for data collection. It included the following questions: How do you evaluate tuberculosis contacts? What does LTBI (Latent Tuberculosis Infection) mean? How is the LTBI diagnosis established? What is the treatment regimen for LTBI?
For selecting the professionals, we carried out a draw between the areas of the city studied, which are east/southeast area, comprising 36 Basic Health Units (BHU); north area, 25 BHU; and the south area; with 27 BHU [22]. The east/southeast was the area selected. Subsequently, we carried out the interview daily, in morning and afternoon shifts.
The results of the qualitative research revealed that health professionals know the definition of LTBI; however, they do take action regarding the identification of LTBI. Concerning the training on the subject, the professionals reported that LTBI was not emphasized, and that they have little knowledge about this infection.
It is noteworthy that the qualitative research followed resolution 466/2012 of the National Health Council, being approved under opinion 2.932.141.
2.1.2. Second Step
Due to the knowledge of the technology required for creating a mobile application, an information technology professional collaborated in the modeling stage. We chose the iOS operating system, as the device available was an iPhone 6s, which belonged to one of the authors. For future tests, this application will be developed for the Android operating system, The framework chosen was Xcode, and the programming language, Swift, both native to iOS, giving more consistency and reliability to the product, as both are specific to this purpose: developing applications for Apple products. This choice also allows future improvements without any concerns about the technology support used. The portability and ease of use of the application also contributed to the choice, since moving to collect the data will be needed.
2.1.3. Third Step
The third phase was the implementation, which was subdivided into two steps. The first comprised a usability study for analyzing how the user would interact with the application. In the second, we analyzed how the treatment of LTBI is carried out according to the flowchart presented in the national guidelines. Then, we proceeded to the creation process using the Xcode Framework, in which we generated all the screens and their layouts. We adopted screens with objective layouts containing only useful information for users, thus, reducing the difficulty of handling the application. There were no specific reasons for choosing the predominantly blue color in the application. The software was named “Orienta TB.”
In the future, evaluation, maintenance, and distribution phases will be carried out. For the testing phase, the application will be evaluated and validated by design professionals [23] and FHS professionals [24]. From the results of these tests, a release version will be published in the iOS app store and Google Play Store, being available for free (Fig. 1).
3. RESULTS
The application named “Orienta TB” provides a tool to assist FHS professionals in screening, evaluating, and treating active TB contacts. It is considered a hard technology, as software is being produced.
After compiling the documents published by the Ministry of Health on the investigation of TB contacts, we designed and organized the textual content of each screen to guide FHS professionals on evaluating the contacts.
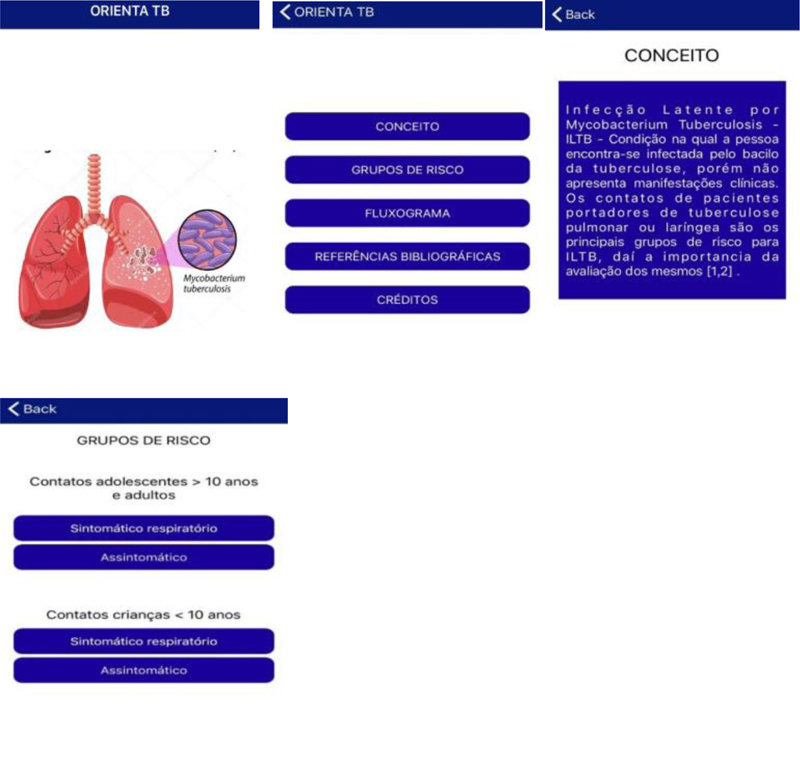
We produced 25 screens that integrated the elements to guide the evaluation of TB contacts in PHC. The first screen presents the application “Orienta TB.” The second screen summarizes the content that the professional can access, such as the concept of LTBI, risk groups, flowcharts for the screening and assistance of TB contacts in specific situations, bibliographic references, and the credits of the application. The third screen describes the concept of LTBI, and the fourth initiate the assessment of TB contacts by risk groups (adults and adolescents contacts > 10 years old; children contacts< 10 years old).
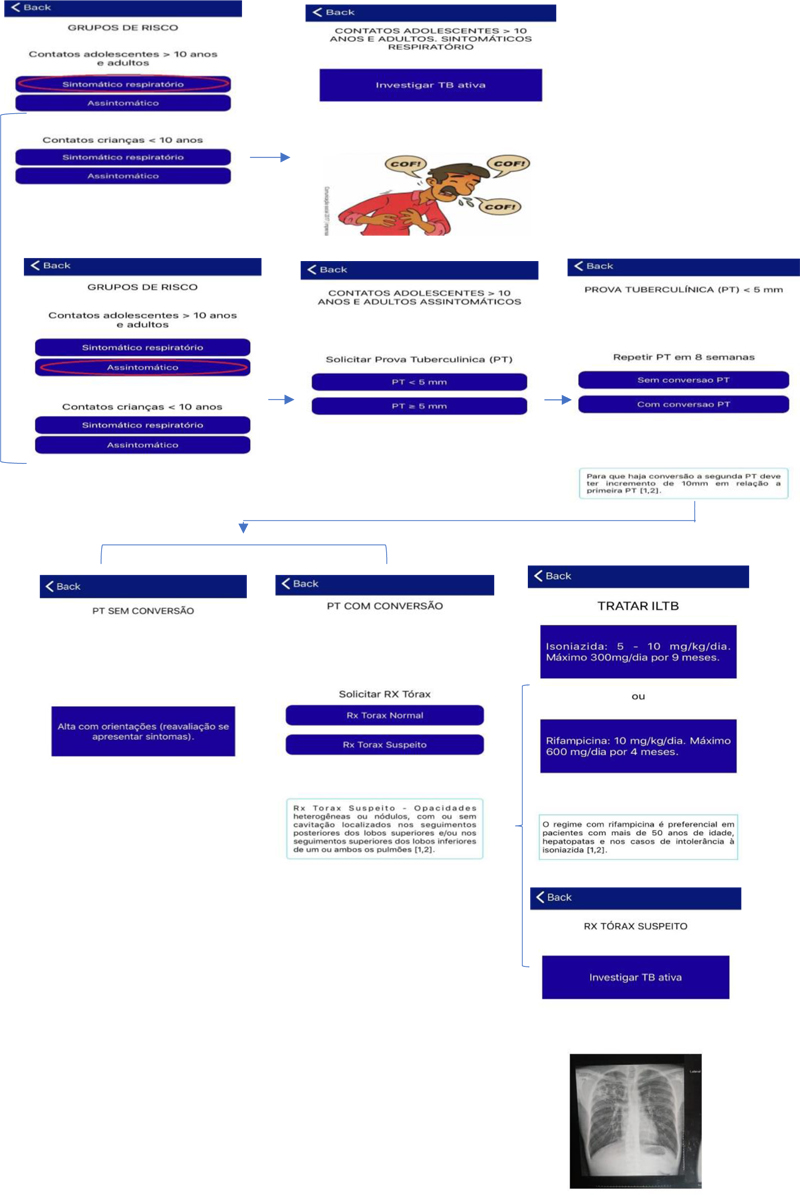
The investigation starts after the health professionals select the risk group. From the fifth to the 13th screen, they have access to the guidelines related to the first risk group: adults and adolescents contacts > 10 years old (Fig. 2).
If the option “respiratory symptomatic” is selected the software path will follow to “investigating active TB”. As the main objective of the appl is examining TB contacts for LTBI and not investigating active TB, after selecting this option, the guiding path is finished (Fig. 2).
When choosing asymptomatic” patient, the Tuberculin Test (TT) will be requested. Regarding the TT results, the appl presents two possibilities, TT < 5mm or TT ≥ 5 mm. If the TT results are below 5 mm, the recommendation is to repeat the test in eight weeks. After this period, with the new results, the professionals have two options to choose, “without TT conversion” and “with TT conversion” (Fig. 2).
After the test analysis, if there is “TT without conversion,” the app will recommend discharging the patients and guiding them on the signs and symptoms of TB and the need to return to the health unit if there is contact with individuals presenting active TB.
The application clarifies that, for the presence of conversion, the second TT test must have an increase of 10mm compared to the first. For example: first, the patient presented 3mm TT, after eight weeks, the second result was 13mm TT; thus, there was conversion. In this case, the health professionals are directed to request a chest X-ray. From this examination, there are two possibilities “normal chest X-ray” and “suspected chest X-ray” (Fig. 2).
If the RX is normal, the professional can initiate the treatment for LTBI Isoniazid or rifampicin are the drugs that can be administered. The drug indicated as the main treatment in the app is isoniazid, with a recommended dosage of 5-10 mg/kg/day for nine months, considering a maximum of 300 mg/day. However, treatment with rifampicin is preferred in patients aged over 50 years old, with hepatopathy, or isoniazid intolerance. The recommended dosage of rifampicin is10mg/kg/day for four months, with a maximum of 600mg/day.
As clarified in the software, the chest X-ray is considered suspect if it presents heterogeneous opacities or nodules, with or without cavitation located in the upper lobe posterior segment or in the lower lobe superior segment of one or both lungs). For this case, the application will advise the investigation of active TB (Fig. 2).
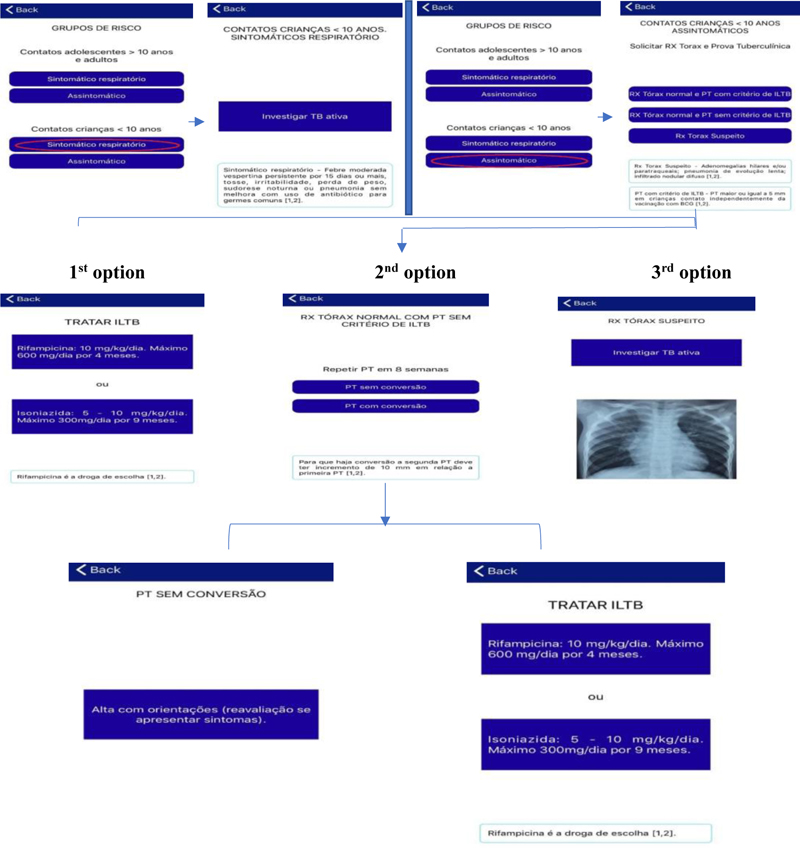
Regarding the risk group of children under ten years old who are contacts of patients with active TB, the professionals can also choose the options “respiratory symptomatic” or “asymptomatic.” When clicking on the first option, the orientation is to investigate for active TB. The app presents an explanation that a symptomatic patient is the one who has persistent moderate afternoon fever for 15 days or more, cough, irritability, weight loss, night sweats, or pneumonia that does not improve with the use of antibiotics for common germs (Fig. 3).
When selecting the option “asymptomatic”, the orientation will be to request the chest X-ray and TT. Having the results, the health professional can choose three options normal chest X-ray and TT with LTBI criterion, normal chest X-ray and TT without LTBI criterion, and suspected chest X-ray (Fig. 3).
For helping the professionals, there are also brief definitions of a suspected chest X-ray (hilar or paratracheal adenomegaly; slow evolution pneumonia; diffuse nodular infiltrates) and TT with LTBI criterion (TT greater than or equal to 5mm in children contacts regardless of BCG vaccination) (Fig. 3).
If, for the case under investigation, the option is “normal chest X-ray and TT with LTBI criterion”, the application suggests following the treatment for LTBI with isoniazid or rifampicin, as mentioned earlier. However, in this risk group, the recommended drug is rifampicin, and the dosage is 10mg/kg/day for four months, considering a maximum of 600 mg/day. If the professional chooses isoniazid, the dosage is 5-10mg/kg/day for nine months, with a maximum of 300mg/day.
If the patient’s test results indicate “normal chest X-ray and TT without LTBI criterion”, the professionals will be requested to repeat the TT in eight weeks. When the patient returns, the procedure is to check whether there was TT conversion. If there is no conversion, the application will recommend discharging this patient, explaining the signs and symptoms of TB and the need to seek the health unit if they are contacts of individuals with active TB.
If the test results present “TT with conversion”, health professionals are advised to treat the patient for LTBI. The treatment will be the same as described for the option “normal chest X-ray and TT with LTBI criterion” (Fig. 3).
The third option for the children risk group is “suspected chest X-ray,” in this occurrence, the procedure is investigating for active TB (Fig. 3).
Regarding other paths, users can follow in the app, the second screen leads to the flowchart, bibliographic references, and credits. In the flowchart item, there are two flowcharts representing the guidelines mentioned above for the two risk groups for LTBI. The item bibliographic references show two updated references of the Ministry of Health: Handbook of recommendations for tuberculosis control in Brazil, of 2011 and 2018.The credits present the professionals who created and developed the application.
4. DISCUSSION
In recent years, mobile apps have gained importance in healthcare. Health-oriented Information and Communication Technologies (ICTs) have a variety of tools that favor the construction and organization of data and information, providing storage, processing, real-time and remote access, and sharing of the data among the health agents involved in this scenario and between patients and these professionals [25-27].
The number of mobile apps available in healthcare has increased dramatically. There is a vast and diverse number of apps, by October 2017, approximately 325,000 mobile health apps were available in major app stores [28]. These applications present tools that allow well-being management, encouraging and monitoring behavioral change, health data collection, disease management, self-diagnosis, medicine reminders, and rehabilitation schedule management [29, 30].
The literature available on health-oriented apps and their outcomes shows that this software, if well designed, can empower patients, improve medication adherence, and reduce the cost of health care [31-33]. One of the advantages of mobile applications is that they can be updated regularly, ensuring that information is based on current evidence and is easily accessible [34].
Regarding mobile devices focused on TB prevention and treatment, a literature review conducted in three mobile app stores in the United States (iTunes App Store, Google Play Store, and Amazon Appstore) and the gray literature showed that the majority of applications were focused on health professionals and provided access to a comprehensive compilation of information or tools designed to support them in monitoring, detecting, and documenting home visits to TB patients. Applications covered in the gray literature also target frontline health professionals in case documentation, contact screening, or patient management [35].
According to the review, there is a lack of applications specifically designed for patients to provide treatment support and care management or promote their involvement in treatment. The ones focused on patients as end-users offered information about the TB disease, transmission, symptoms, diagnoses, and treatment. It is noteworthy that few TB-related apps have been the subject of formal research regarding implementation and evaluation; some had few guidelines or even misinformed patients about appropriate TB treatment options. Other problems found were lack of support and difficulties with functionality, there were apps that no longer worked or that required logins and passwords [35].
Concerning applications to help screening contacts, the review mentioned found only one in the gray literature, and it did not have a specific name [35]. A poster described it as an application designed to digitize and automate contact screening documentation in Botswana, Africa [36].
In 2016, an evaluation of this application was published. It was analyzed the time for completing the screening of TB contacts and the quality of data collected comparing two methods, the app and paper forms, which is the one usually used. The evidence showed that this software eliminates the need for paper forms, writing, manual data input on a database, and manual production of summarized reports. According to the authors, few works in the literature address mobile health apps for screening TB contacts, and they were the first to compare these two methods of investigation [37].
Few reports on health applications about tracking TB contacts were found in the literature. Therefore, there is an opportunity for developing such software to assist in screening these cases and optimize the daily practice of FHS professionals.
In this sense, more objective and specific applications are needed, considering a real scenario for construction and implementation and users’ evaluation.
The limitations of the study are related to the steps that have not yet been carried out (testing phases, implementation, analysis of FHS professionals, and indexing in app stores). These phases are essential to ensure the applicability of the software and its effectiveness in the intended work process.
CONCLUSION
This study developed the mobile application “Orienta TB”, which guides FHS professionals in investigating TBcontacts for LTBI. It presents interactive and dynamic screens that help the professionals to make the correct approach, based on updated guidelines, the screening and evaluation of the TB contact, and the patient’s treatment for LTBI. This application can prevent human errors and increase the quality of care in investigating TB contacts for LTBI.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Comitê de Ética em Pesquisa (CEP) do Centro Universitário UNINOVAFAPI under opinion 2.932.141.
HUMAN AND ANIMAL RIGHTS
The fundamental ethical and scientific requirements for research involving human beings were met, according to Resolution 466/12 of the Brazilian National Health Council.
CONSENT FOR PUBLICATION
All participants signed the term of consent.
AVAILABILITY OF DATA AND MATERIALS
The authors confirm that the data supporting the findings of this study are available in the article.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

