All published articles of this journal are available on ScienceDirect.

Association between Food Intake and Overweight in Children Assisted by Primary Care
Authors Info & Affiliations
Abstract
Background:
The child feed in the first two years of life is of fundamental importance for a healthy growth and development.
Aims:
To verify the association between food consumption indicators and overweight in children under the age of two, followed up by primary care health professionals.
Methods:
A cross-sectional study was conducted on 232 children assisted by primary care. A structured questionnaire was used with questions on sociodemographic data of mothers or guardians and food intake and anthropometric data of children. The analysis of the association between excess weight and food intake indicators was performed using the Pearson’s chi-square test (χ2) and Fisher’s exact test (f ˂ 5).
Results:
Regarding food intake in children under 6 months of age, 35.1% of the children were exclusively breastfed. Among children at the age of 6 to 23 months: 66.3% were on continued breastfeeding; 16.7% consumed adequate foods at the age of 6 to 8 months; 90.4% consumed foods that belonged to the six food groups; 76.3% consumed food at the minimum frequency and with adequate consistency; 88.9% consumed iron-rich and vitamin A-rich foods, and 59.3% consumed ultra-processed foods. Regarding nutritional status, 24.5% of the children were overweight.
Conclusion:
There was no statistically significant association between overweight and food consumption indicators among the surveyed children. However, exclusive breastfeeding was below the recommended level, a low percentage of the introduction of complementary foods at the appropriate age and high consumption of ultra-processed foods reveal the need to improve the assistance provided by primary care to this group.
1. INTRODUCTION
Child feeding in the first 2 years of life is of fundamental importance for healthy growth and development. The World Health Organization (WHO) recommends exclusive breastfeeding (EBF) until the sixth month of life. After this period, new foods known as complementary foods must be introduced. Breastfeeding relates in several ways to the sustainable development goals since it promotes a better start in life for children, regardless of whether they are born in a high or low-income country or whether their family is rich or poor. Thus, breastfeeding collaborates with the Sustainable Development Goal (SDG) 1 (End of poverty). As for SDG 2 (Zero Hunger), EBF during the first six months helps to prevent hunger, malnutrition, and obesity by ensuring all the nutrients and calories necessary for the baby’s growth and development [1, 2].
One of the most recurrent problems in the imbalance of infant feeding is overweight. Besides the hereditary component, excessive intake of high-calorie foods and low physical activity contribute to overweight. Children with these conditions are at higher risk of developing diseases such as arterial hypertension, stroke, and metabolic syndrome [3].
In Brazil, child health care has undergone changes with scientific advances, the incorporation of technologies and the adoption of care models. The Family Health Strategy (FHS) has consolidated itself as the main strategy for child health surveillance, in the context of primary care, with emphasis on the adoption of instruments for monitoring the child's growth and development, as well as encouraging breastfeeding, maternal health, immunization, and attention to diseases prevalent in childhood [4, 5].
Under this focus, this study aimed to verify the association between food consumption indicators and overweight in children under the age of two, followed up by primary care health professionals. In this perspective, as the study made it possible to make a nutritional diagnosis of this group and establish its association with food intake, the results can contribute to the elaboration of strategies aimed at improving the health of the assisted children.
2. METHODS
This is a cross-sectional study targeting children aged between 0 to 23 months and 29 days accompanied by the Family Health Strategy (FHS), in Basic Health Units (BHUs), in the capital city of the Northeast of Brazil. The FHS is the strategy of action and intervention of the primary health care model in Brazil, responsible for monitoring families in all age groups. It has a minimal team made up of medical professionals, nurses, nursing technicians, and community health agents. In the specific case of children, the target audience of this study, care is provided by the doctor and nurse at the BHUs, located in the neighborhoods in which they live, according to the minimum schedule of consultations recommended by the Brazilian Ministry of Health (MS) [6].
According to data from the Live Birth Information System (SINASC), 13,535 children were born in the year 2017 [4]. The sample calculation was made using the formula n = [(Zα/2)2 x p x q]/E2 [5], applying a sampling error of 5% and a confidence level of 95%. The final sample consisted of 232 children. Data were collected from March to April 2019.
Children were selected through probabilistic sampling proportional to the number of BHUs in each of the four zones of the city (North, East, South, and Southeast), by means of a simple draw. The municipality has 72 BHUs in the urban area. Thus, each area of the city had at least two BHUs drawn in order to reach the desired number of children. However, when the number of children proportional to the area was not enough, a new BHU was drawn until the minimum sample size of participants was reached. Thus, the research was carried out in 13 BHUs in the urban zone of the municipality.
Children were recruited in the consultation waiting room, where parents or guardians were invited to participate in the study. When they accepted the invitation, they were informed about the objectives and the need to sign the Informed Consent Form (ICF). The researcher read the ICP, answering the doubts presented by those with less schooling degree. It is noteworthy that all participants could sign their names and that the participation in the study occurred only after signing the ICF. All parents or guardians signed the consent form. There were no refusals to participate in the study.
The following inclusion criteria for participation in the study were considered: being a child aged 0 to 23 months and 29 days assisted and monitored by the FHS; being present at the time of the interview, and being monitored by the staff of the BHU. Children born from a twin pregnancy or presenting other progressive pathologies that could interfere with nutritional status, such as Prader Willi and Down syndromes and hypothyroidism, were excluded. The interviews were conducted with the mother or guardian of the child in the facilities of the BHU by the main researcher, in a space indicated by the coordination of the BHU.
The instrument used for data collection consisted of a structured questionnaire with questions about the sociodemographic data of the mothers or guardians and anthropometric data and food intake of the child. The sociodemographic variables surveyed were: sex and age of the child, mother’s age, marital status and schooling, number of family members, monthly income, and social benefits.
The anthropometric variables, weight and height, were collected by the main researcher. Children were weighed, measured, and classified according to the BMI, as recommended by the WHO for children under two years of age, according to the instructions in the manual of the SISVAN (Food and Nutrition Surveillance System) of the Ministry of Health (MOH) [6]. Weight was measured with the subject with bare feet on a digital scale, with a capacity of up to 180 kg and sensitivity of 100 g. Height was obtained using a portable stadiometer, with a capacity of 100 cm and sensitivity of 0.1 cm, both from the Seca brand.
Food consumption was assessed using the form for assessing food consumption markers proposed by the Ministry of Health. This form assesses food consumption for the foods consumed the day before, which eases possible memory biases. It is noteworthy that this form should be used by ESF professionals in the routine of attending children in the UBS [7]. The indicators proposed by the Ministry of Health and used for the purposes of this study are as follows:
- EBF: estimated the proportion of children under 6 months of age who received breast milk exclusively;
- Continued breastfeeding (CBF): defined the proportion of children aged between 6 to 23 months and 29 days who received breast milk;
- Introduction of foods: reflected the proportion of children aged between 6 to 8 months and 29 days who received food at the frequency recommended for their age;
- Minimum food diversity: showed the proportion of children aged between 6 to 23 months and 29 days who received six groups of food (breast milk or milk other than breast milk, porridge with milk or yogurt; fruits, vegetables and greens; plant foods or fruits with an orange color and dark green leaves; meat and eggs; beans; and cereals and tubers);
- Minimum frequency and adequate consistency: assessed the proportion of children aged between 6 to 23 months and 29 days whose frequency and consistency of salt consumption in the lunch and dinner was appropriate for their age;
- Consumption of foods rich in iron and vitamin A reflected the proportion of children aged between 6 to 23 months and 29 days who received foods rich in these minerals;
- Consumption of ultra-processed foods: showed the proportion of children aged between 6 to 23 months and 29 days who consumed at least one food from this group, sweetened drinks, instant noodles, packaged snacks or crackers, cookies, and sweets or candies.
In this study, we used BMI/Age as a parameter to assess nutritional status, as defined by the World Health Organization in 2006, as a reference curve for assessing the nutritional status of children under five [6].
The classification was made according to the z-score: a result greater than or equal to +2 was considered “overweight (overweight + obesity)”, and those less than +2 were classified in the category “without overweight”. The Ministry of Sause adopts the z-score classification in the child growth assessment charts contained in the Child Health Handbook, an instrument used by the FHS to monitor children. The classification of nutritional status was carried out by the main researcher in this study [6] and reviewed by another researcher.
In the present study, the diagnosed nutritional status of the child was considered an outcome (dependent) variable in two categories: no overweight and overweight. The explanatory variables were the calculated food intake indicators.
Data were tabulated in a Microsoft Office Excel 2016 spreadsheet and analyzed in the statistical package Stata® version 12. Fisher’s exact test was used to study the dependency between the variables. The level for rejection of nullity in the statistical analyses was set at α = 0.05.
The research was authorized by the Research Ethics Committee (CEP) through opinion No. 3,018,809 of November 13, 2018, as recommended by Brazilian laws.
3. RESULTS
A total of 232 children participated in the study. The sociodemographic data are described in Table 1. Of these children, 50.9% were female, and 64.6% were between 6 and 23 months of age. Regarding mothers, 88% were between 20 and 49 years old; 72.4% had a partner; 67.2% had completed high school and a higher education, and 66.8% had families with more than 4 members. Regarding family income, 75.8% had an income of up to 2 minimum wages. It is noteworthy that 30.2% received social benefits from the Federal government (Table 1).
| Variables | n | % |
|---|---|---|
| Child's sex | ||
| Male | 114 | 49.1 |
| Female | 118 | 50.9 |
| Child's age (months) | ||
| < 6 | 97 | 41.8 |
| 6 – 11 | 60 | 25.9 |
| ≥ 12 | 75 | 32.3 |
| Maternal age (years) | ||
| < 20 | 28 | 12.0 |
| 20 to 29 | 99 | 42.7 |
| 30 to 49 | 105 | 45.3 |
| Marital status | ||
| Married | 100 | 43.1 |
| Consensual union | 68 | 29.3 |
| Single | 62 | 26.7 |
| Separated | 2 | 0.9 |
| Number of family members | ||
| 1 to 3 | 77 | 33.2 |
| 4 to 5 | 106 | 45.7 |
| > 5 | 49 | 21.1 |
| Monthly Income (MW: minimum wage) | ||
| < 1 | 75 | 32.3 |
| 1 to 2 | 101 | 43.5 |
| 3 to 4 | 41 | 17.7 |
| 5 to 10 | 15 | 6.5 |
| Other | ||
| Social benefit | ||
| Yes | 70 | 30.2 |
| No | 162 | 69.8 |
| Education | ||
| Not literate | 1 | 0.5 |
| Incomplete primary school | 30 | 12.9 |
| Complete primary school | 14 | 6.0 |
| Incomplete secondary school | 31 | 13.4 |
| Complete secondary school | 97 | 41.8 |
| Incomplete higher education | 19 | 8.2 |
| Complete higher education | 40 | 17.2 |
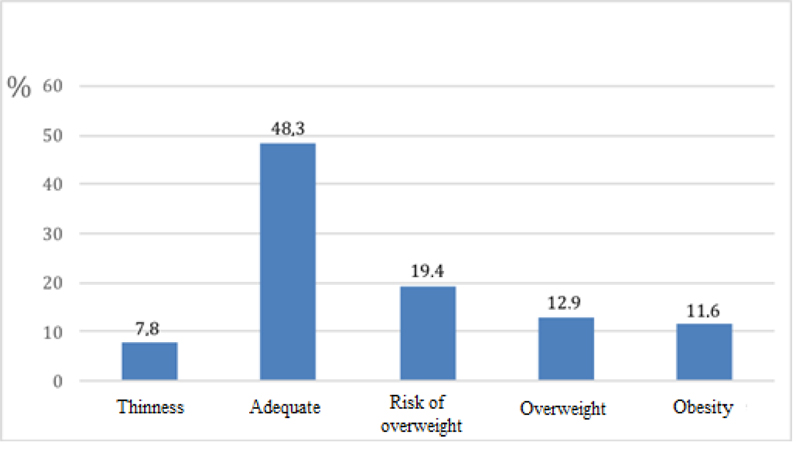
With regard to anthropometric assessment, according to BMI/Age, 24.5% of the children had excess weight, of whom 12.9% were overweight and 11.6% were obese (Fig. 1).
The children's food consumption indicators are shown in Table 2. As for the breastfeeding indicators, 35.1% of the children under 6 months were in EBF and 66.3%, aged 6 to 23 months, were in CBF. The introduction of food at the appropriate age, 6 to 8 months of life, occurred in 16.7% of children in this age group. Among children aged between 6 to 23 months, regarding the minimal eating diversity, 90.4% did not consume food from the six recommended food groups, for this phase (breast milk or milk other than breast, porridge with milk or yogurt; fruits, vegetables and fruits; vegetables or colored fruits orange and dark green leaves, meat and eggs, beans, and cereals and tubers); 76.3% consumed food at the minimum frequency and adequate consistency, 88.9% consumed foods rich in iron, as well as vitamin A, and 59.3% used ultra-processed foods (sweetened drinks, instant noodles, snacks) packet or savory cookies, stuffed cookie and sweets or treats) (Table 2).
| Variables | N | % |
|---|---|---|
| <6 months | ||
| Exclusive breastfeeding (n = 97) | ||
| Yes | 34 | 35.1 |
| No | 63 | 64.9 |
| 6 to 8 months | ||
| Food introduction (n = 24) | ||
| Yes | 4 | 16.7 |
| No | 20 | 83.3 |
| 6 to 23 months | ||
| Continued breastfeeding (n = 135) | ||
| Yes | 90 | 66.7 |
| No | 45 | 33.3 |
| Minimum food diversity (n = 135) | ||
| Yes | 13 | 9.6 |
| No | 122 | 90.4 |
| Minimum frequency and adequate consistency (n = 135) | ||
| Yes | 103 | 76.3 |
| No | 32 | 23.7 |
| Intake of iron-rich foods (n = 135) | ||
| Yes | 120 | 88.9 |
| No | 15 | 11.1 |
| Intake of vitamin A-rich foods (n = 135) | ||
| Yes | 120 | 88.9 |
| No | 15 | 11.1 |
| Intake of ultra-processed foods (n = 135) | ||
| Yes | 80 | 59.3 |
| No | 55 | 40.7 |
As for the association between food intake and excess weight, as shown in Table 3, there was no statistically significant association between overweight and food consumption indicators in children under two. Although there are no differences in food consumption indicators between groups (overweight and not overweight), the low proportion of children in EBF under the age of six months and the high proportion of consumption of ultra-processed foods is emphasized.
| Variables | Overweight | p-value | |||
|---|---|---|---|---|---|
| No | Yes | ||||
| n | % | n | % | ||
| Exclusive breastfeeding (n = 97) | |||||
| Yes | 29 | 35.4 | 5 | 53.0 | 0.565 |
| No | 53 | 64.6 | 10 | 66.6 | |
| Continued breastfeeding (n = 135) | |||||
| Yes | 62 | 66.7 | 28 | 66.7 | 0.575 |
| No | 31 | 33.3 | 14 | 33.3 | |
| Food introduction (n = 24) | |||||
| Yes | 11 | 73.3 | 9 | 100.0 | 0.259 |
| No | 4 | 26.7 | - | - | |
| Minimum food diversity (n = 135) | |||||
| Yes | 85 | 24.7 | 37 | 88.1 | 0.376 |
| No | 8 | 75.3 | 5 | 11.9 | |
| Minimum frequency and adequate consistency (n = 135) | |||||
| Yes | 23 | 24.7 | 9 | 21.4 | 0.427 |
| No | 70 | 75.3 | 33 | 78.6 | |
| Intake of iron-rich food (n = 135) | |||||
| Yes | 12 | 11.3 | 2 | 8.3 | 0.501 |
| No | 94 | 88.7 | 22 | 91.7 | |
| Intake of vitamin A-rich foods (n = 135) | |||||
| Yes | 10 | 10.8 | 5 | 11.9 | 0.527 |
| No | 83 | 89.2 | 37 | 88.1 | |
| Intake of ultra-processed foods (n = 135) | |||||
| Yes | 38 | 40.9 | 17 | 40.5 | 0.560 |
| No | 55 | 59.1 | 25 | 59.5 | |
Fisher’s exact test
4. DISCUSSION
The results found in the present study allowed an analysis of the food intake of children under 2 years of age, accompanied by the FHS and its association with excess weight data found. A similar profile between the two sexes was found in terms of sociodemographic characteristics, which is in line with a published study [8] about the sociodemographic and obstetric profile of women in groups that encourage breastfeeding in a poor community, with children up to six months old, in which 50.31% of the babies were female, thus, similar to the present study.
Family income is one of the key factors for the proper development of children. It was observed in this study that most families received up to two minimum wages and a minority had social assistance. These are factors that can influence the adequate development of children because low socioeconomic level can reflect negatively on breastfeeding [8].
A study with 77 children aged between 7 to 36 months in the city of Matinha-PR analyzed, among other factors, the relationship between family income and adequate development of children, demonstrating the negative impacts of poverty and precarious socioeconomic factors in the first years of life [9].
As for maternal age, marital status, and schooling, it was observed that most mothers in the present study were aged over 20 years, had complete high school or higher education, and were married or in a stable relationship, which could be important factors for the prevalence of breastfeeding during the recommended time. However, the prevalence of EBF was below the recommended WHO standards in this study, in particular. According to a study, mothers who have the greatest chance of breastfeeding are those who are over the age of 20, have a high school or higher education, and are married [10].
With respect to the results of EBF in children under 6 months of age found in the present study, a small percentage was observed. Studies carried out in other municipalities with children assisted by the FHS also showed low indicators of EBF among children under six months of age. For example, the study carried out in the municipality of São José do Piauí found 17.86% of EBF [11], another carried out in Guarapuava-PR found 36% of EBF [12], and a survey conducted in Ribeirão das Neves-MG found 30% of EBF in children under six months of age [13].
Regarding the indicator “Introduction of food” at the recommended age, the results found in the present study showed a low percentage. However, it is important to note that the number of children assessed at the age of 6 to 8 months was small when compared to the study population and may not reflect reality. Given the importance of adequate and timely complementary foods for the health of children under two years of age, the promotion of healthy complementary foods, in a timely manner, has become a priority in the agenda of public food and health policies, prioritizing the first two years of life, and recognizing them as a crucial period in the child’s growth and development [14].
The introduction of adequate complementary feeding in a timely manner is a challenging issue for health professionals in the context of Primary Health Care. The WHO advocates EBF until the 6th month of life; after this period, new foods should be introduced because breast milk no longer provides all the nutrients necessary for the healthy growth of the child [2].
The values found in the indicator “Minimum food diversity” are a reason for concern because they presented low percentages, indicating that the feeding of these children is not as recommended by the WHO [2]. Similar values were found in a study with 2,477 children aged between 6 to 36 months conducted by the National Survey of Demography and Health in Brazil (2006/2007) to assess the quality and diversity of the diet. In this study, it was observed that only 20% of Brazilian children consumed four or more food groups, indicating that, in general, the children’s diet is monotonous and this can contribute to the worsening of the main nutritional problems existing in the country [15].
Complementary food should consist of healthy foods, with acceptable cost and prepared based on items and culinary ingredients consumed by the family. Foods with a high degree of processing, industrialization, excess salt, sugars, and additives, and artificial preservatives should not be offered to children in the first years of life [16]. In this study, in particular, the high percentage of consumption of ultra-processed foods is an indicator that deserves to be highlighted; more than half of the children older than 6 months had consumed some ultra-processed foods the day before the survey. It is noteworthy that the use of an indicator referring to the previous day may not reflect the consumption of this type of food.
The National Health Survey of 2013 corroborates the findings of the present study with respect to high consumption of processed and ultra-processed products by children under 24 months of age. Consumption rates of 60.8% of cookies, crackers, and cakes and 32.3% that of soft drinks and artificial juices were observed [7]. In another study carried out in the city of São Paulo, the introduction of these foods in children under 12 months of age had alarming prevalence values: foods such as instant noodles were consumed at a percentage of 70.6%, salty snacks at 65.9%, sausages at 54.7%, chocolate at 67.1%, ice cream at 36.9%, and cookies at 68.7% [17].
These are worrying numbers when it comes to complementary food, regarding the processed foods given to children under two years of age. These findings raise the question of whether mothers are properly instructed about the introduction of complementary feeding and whether they are aware that the high consumption of foods not recommended for the age of the children can contribute to the creation of unhealthy eating habits in adulthood [13].
Regarding the prevalence of overweight, a high percentage was observed, corroborating other studies. In a survey carried out with children living in private households in the urban areas of 100 small, medium and large municipalities across the 5 geopolitical regions of Brazil, an overall prevalence of 13.1% of overweight was found in children under 24 months of age in urban populations in Brazil [18]. This is considered a contemporary, multifactorial public health problem. Besides resulting in excessive accumulation of fat in the body, overweight can be linked to the appearance of diseases [19].
Another study carried out in the five regions of Brazil investigating the nutritional status of children under two years of age found an average prevalence of 15.9% of overweight [20]. In a cohort study in Canada with 1,996 children in which the demographic and obstetric characteristics of this population were analyzed, 34.2% of the children under 5 months of age were overweight [21], similar to the present study, which indicates that this is likely a problem at the international level.
As a consequence, overweight children are prone to developing several health problems, such as psychosocial disorders, several metabolic and hemodynamic anomalies, which are cardiovascular risk factors, including arterial hypertension, dyslipidemia, decreased glucose tolerance, resistance to insulin and type 2 diabetes mellitus, skeletal changes, and orthopedic complications, in addition to respiratory disorders and sleep disorders [22-24].
In the present study, there was no association between overweight and the food consumption indicators analyzed among children. Few studies with this theme were found in children aged between 3 to 6 years (preschool age). An example is the study carried out in municipal daycare centers in the city of Teresina, which found a strong correlation (r> 0.7) between the occurrence of overweight and the consumption of foods such as bread; cookies, cakes, sweet pies, dairy products, chocolate, and sausages [25].
Another study carried out with preschoolers in a city in northeastern Brazil found an association between overweight and lower fruit consumption; however, other variables related to higher maternal education, higher family income, maternal overweight, presence of catch-up growth, and sedentary behavior were also associated, showing that, despite the important role of food consumption in the occurrence of overweight in children, other variables also contribute to this problem. The authors denote the need to recognize this problem as multicausal to guide public policies aimed at this age group with the objective of preventing this nutritional problem [26].
In Brazil, despite continuous transformations with scientific advances, child health care is developed with the proposal of favoring the approximation between health services and the community through embracing and trusting relationships that favor bonding [27-29]. In primary care, child monitoring and health promotion are closely related to health surveillance and child development, whose actions are capable of reducing situations of vulnerabilities and risks, such as those found in the present study. They favor the early identification and intervention of delayed child development. However, it is important to consider the coexistence of different primary care models in the country, in addition to an increasing number of FHS units, which have different health work processes, with different ways of producing child care [29-31].
A limitation of this study was the use of a data collection instrument that portrays food consumption only of the day prior to the research. In this sense, the inference should be careful since it may not represent the frequent food consumption of the child. However, this questionnaire is easily applicable, and the proposed food consumption indicators allow for analysis, even if preliminary, of the feeding of children under two years of age.
CONCLUSION
The analysis of the association between food consumption indicators and overweight among children under the age of two, accompanied by primary care, showed no statistically significant association. However, exclusive breastfeeding was below the recommended level, along with a low percentage of the introduction of complementary foods at the appropriate age, and high consumption of ultra-processed foods. In view of this, it is necessary to take a close look at the work carried out by primary care professionals since they are fundamentally important to change this reality through encouraging EBF until six months of life and guidance on the introduction of adequate and timely complementary foods in order to improve the health condition of children and promote their adequate growth and development.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The research was authorized by the Research Ethics Committee (CEP) through opinion No. 3,018,809 of November 13, 2018, as recommended by Brazilian laws.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures were followed in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from all participants.
STANDARDS OF REPORTING
STROBE guidelines and methodologies were followed for this study.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

