All published articles of this journal are available on ScienceDirect.

Health-Related Quality of Life and Undergraduate Nursing Students: A Narrative Review
Abstract
Background:
Undergraduate nursing students are vulnerable to stressful university learning environments and poor working conditions in clinical rotations. This can result in students leaving nursing programs or abandoning the profession following graduation. As a result, the health-related quality of life of nursing students is an important indicator to monitor student quality of life adequacy. Preventing premature student nurses' departure from the profession is necessary to reduce the nursing shortage.
Objective:
To describe the body of knowledge about the health-related quality of life for undergraduate nursing students during their qualification process.
Methods:
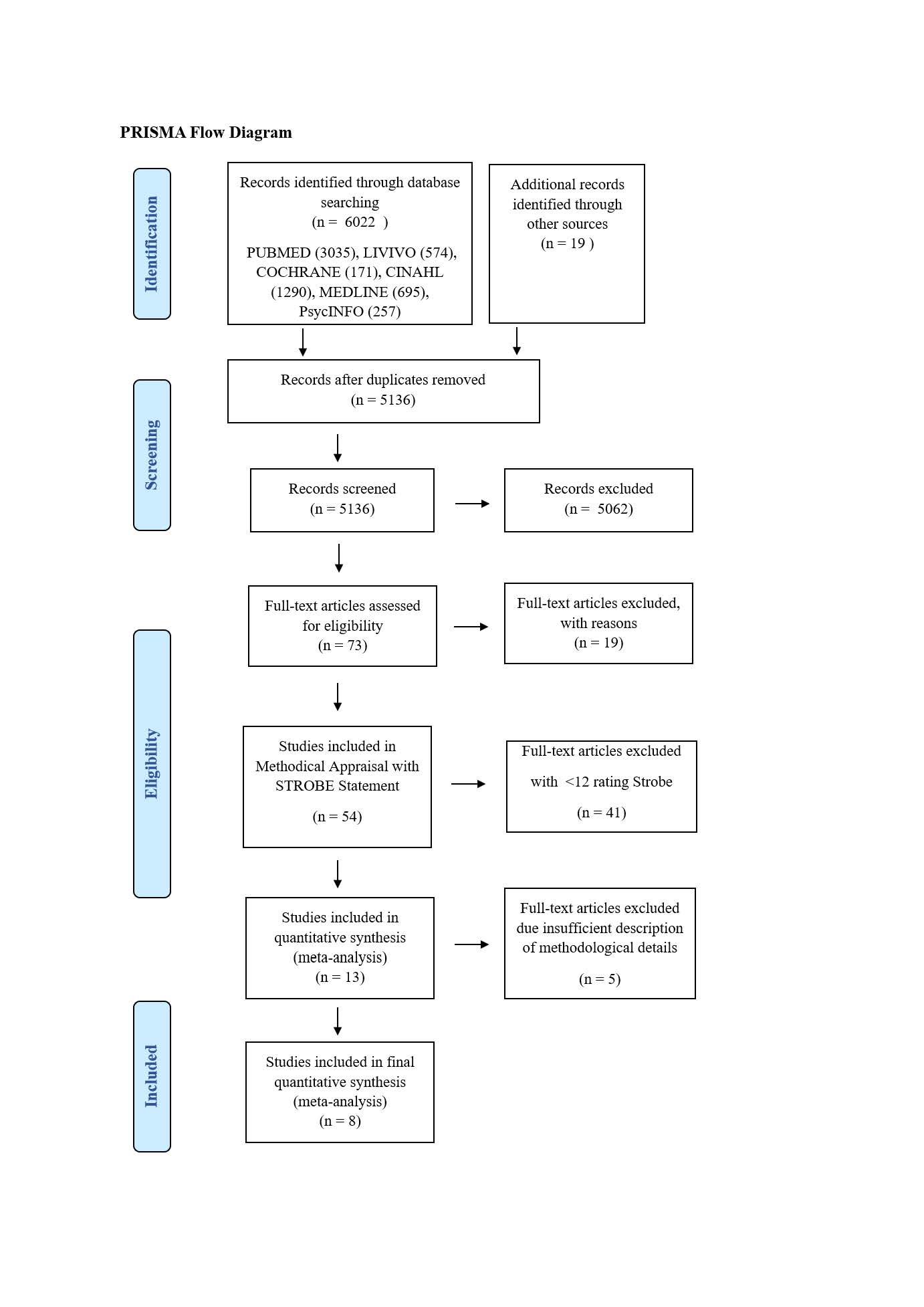
This was a narrative review through a six-database search, including Cochrane, CINAHL, Pubmed, Medline, PsycINFO and Livivio, from between January 1990 and June 2018, with updates in the search followed until November 2019. To assess study quality, the STROBE checklist was used.
Results:
Eight studies were included in a narrative synthesis. All studies were of cross-sectional design, and none included follow-up procedures. Most of the studies recruited participants from nursing courses and only one study recruited students from a national register. Sample sizes ranged from 110 individuals to 4,033 participants in the register-based study. Common health-related dimensions evaluated included stress, social support, mental health, fatigue, quality of life, and drug abuse. Stress, the most commonly studied dimension, was associated with clinical placements, final exams, and non-prescribed drugs. Social support networks were positively associated with coping abilities and self-esteem.
Conclusion:
There is low-quality evidence of the impact of nursing courses upon student health-related dimensions (stress, self-esteem, health-related behaviors). Nurse educators should be aware of these associations and support routine screening of students and their health-related dimensions. Interventions, such as consultation and study redesign, might increase the level of health-related dimensions. Nursing schools should further collaborate to investigate these associations and tailored interventions to positively affect health-related dimensions in nursing students.
1. INTRODUCTION
Nurses representing more than half of the global health professional workforce (estimated 21 million) [1] are essential for healthcare systems to provide health services to their communities, including emergency services and mental health. Complaints about poor working conditions, mandatory overtime, recruitment and retention problems are common in the nursing community [2]. The result is a global shortfall of approximately 9 million nurses with an expected 8 million vacant nursing positions by 2030 [3, 4]. This deficit is exacerbated, as the elderly population will almost double from 12% to 22% by 2050 [5].
A widely known reason for the nursing deficit is the poor working conditions [7], resulting in a high-stress work environment. The Nurses’ Early Exit Study (NEXT-Study) reported that nurses with lower skill levels were more likely to either change employers or leave the profession [6]. The profession is not considered attractive for higher skill level nurses due to the weekend and shift work, high physical and psychological stress, limited advancement opportunities, and inadequate compensation for the required education, skills, and time [8]. Kahn et al. [9] reported that nearly 50% of the nurses could not provide the necessary professional care to address the needs of their patients. There is a clear conflict between nurse expectations about their professional role and their ability to fulfill this role at work. This incongruency will continue to contribute to increased turnover, particularly with newly graduated nurses [10].
While preparing to enter the nursing profession, university students encounter stressful learning environments and difficult clinical rotations [11]. Upon graduation, the new nurses are also vulnerable to poor clinical experiences, resulting from limited guidance and inadequate support during their clinical qualification [12]. Attempts by institutions to compensate for the shortfall of nursing graduates by increasing the number of training positions need to include reforms to improve the working conditions. The problems that the undergraduate nursing students are confronted with are limited career guidance, heavier workloads associated with increased clinical training throughout their education program, and the prospect of limited opportunities for a satisfying career [12, 13].
The physical and mental health of nursing students is an important area for increased research and more evidence-based interventions. In particular, the evidence basis for the health-related quality of life (HRQOL) of nursing students needs to be further explored. HRQOL is a multi-dimensional concept commonly used to examine the impact of health status on quality of life [14]. The HRQOL is considered a useful indicator for overall health, including the physical and mental health status of individuals [15, 16]. HRQOL is usually assessed via multiple indicators of self-perceived health status and physical and emotional functioning. We aim to describe the body of knowledge about the health-related quality of life for undergraduate nursing students during their qualification process.
2. MATERIALS AND METHODS
This study was a narrative review method designed to summarize the empirical literature about the health-related quality of life of nursing students. The narrative review synthesizes studies to stimulate general debates, illustrate the appraisal of previous studies, describe the current lack of knowledge, and provide rationales for future research [17]. The adopted question for this review was What is the health-related quality of life of undergraduate: nurses during their qualification process? (Table 1).
2.1. Search Strategy
Six electronic databases, including PUBMED, COCHRANE, CINAHL, MEDLINE and PsycINFO and LIVIVIVO, were searched between January 1990 and June 2018. In addition, hand searches were performed to collect grey literature and further references using the snowball method. Search strategies were guided by a systematic approach to the research questions. Minor adoptions were used to address the different designs of databases (Table 2).
| Sample | Nurse students |
| Phenomenon of Interest | Health status during studies |
| Design | Questionnaire, survey, or observational study |
| Evaluation | Health-related quality of life |
| Research type | Quantitative |
| Nursing student or nursing school OR nursing school OR nursing apprenticeship OR nursing education | AND | Health-related behaviors or health-related quality of life or quality of life OR HRQL OR health status OR health behavior OR burden OR emotional stress OR emotional stress |
| Reference |
| Chen C-J, Chen Y-C, Sung H-C, Hsieh T-C, Lee M-S, Chang C-Y. (2015) The prevalence and related factors of depressive symptoms among junior college nursing students: a cross-sectional study [51] Reason: Unclear exposure measurment of depression symptoms (no use of valid instrument). |
| Fabbris JL, Mesquita AC, Caldeira S, Carvalho AMP, Carvalho EC (2017) Anxiety and Spiritual Well-Being in Nursing Students: A Cross-Sectional Study [52] Reason: Missing description of recruiting procedure and response rate (selection bias). |
| Grobecker PA. (2016) A sense of belonging and perceived stress among baccalaureate nursing students in clinical placements [53] Reason: Missing presentation of essential study variables (reporting bias). |
| Polat Ü, Özen Ş, Kahraman BB, Bostanoğlu H. (2016) Factors Affecting Health-Promoting Behaviors in Nursing Students at a University in Turkey [54]. Reason: Unclear exposure measurement of depression symptoms (no use of valid instrument). Selective presentation of associations of variables (reporting bias). |
| Tuomi J, Aimala AM, Žvanut B. (2016) Nursing students' well-being using the job-demand-control model: A longitudinal study [55] Reason: No information about the characteristics of the study sample (reporting bias). |
2.2. Inclusion Criteria
We included studies on full-time education programs in the field of nursing, specifically registered nurse programs. English was defined as the publication language, access to the abstract and full-text was mandatory for inclusion. The review examined literature that had been peer-reviewed.
2.3. Data Processing
The search was completed in June 2018, and the results were processed using Endnote (Version: X8). All duplicates were removed electronically. All titles and abstracts were screened according to the inclusion criteria. For a valid screening process, a double screening method was used for 10% of the articles (n = 514); the articles were randomized (Software: ResearchRandomizer) prior to the screening. Interrater reliability, measured with Cohens Kappa, was 0.78, which was appropriate according to methodological standards [18].
From the 136 record abstracts screened, 72 were potentially relevant to the research question. Reasons for exclusion were noted and inconsistencies between the author groups were discussed until consensus. A hand search with reference lists from the selected papers provided no additional studies. After a full-text review, 54 studies were left for critical appraisal. The literature identification process is summarized in Fig. (1).
2.4. Treatment of the Results
The full-text articles were subjected to a critical appraisal using the “STROBE statement—checklist of items in reports of observational studies” [19]. This checklist contains 22 items in the following five categories: 1) title and abstract (1 item), 2) introduction (2 items), 3) methods (9 items), 4) results (5 items), 5) discussion (4 items), and other information (1 item).
Each article was assessed with the checklist. Rating options for each of the 22 items were either one (sufficient = requirement of STROBE checklist item is fulfilled) or zero (not sufficient = requirement of STROBE checklist item is not fulfilled). With one point maximum given for each item, one study could reach a maximum of 22 points. The cut-off threshold was set at 11 points; studies with 12 or more points meeting the inclusion criteria were included in the final selection. The cut-off was defined by consensus (Table 3).
2.5. Data Analysis
Due to the methodological diversity of the included studies, a descriptive synthesis was deemed the most appropriate analytical method [20]. The results are presented in categories. A table was prepared with a summary of findings, (Tables 4 and 5).
| Single-center Studies | ||||
|---|---|---|---|---|
| Reference & Study Design | Sample Size, Characteristics | Data Collection | Analysis | Results |
| Gibbons et al. (2011), Stress, coping and satisfaction in nursing students [25] Descriptive, cross-sectional: United Kingdom |
Nursing students invited by the lead researcher from all nursing specialties in the final year of programme in one institution n=171 |
Index of Sources of Stress in Nursing (ISSN) Generalized Self-Efficacy Scale General Health Questionnaire (GHQ, 12-item version) Marlowe-Crowne Social Desirability (10-item version), Brief COPE |
Hierarchical multiple regression analyses Variables with the lowest Beta values were removed until R2, with the greatest amount of variance determined |
Descriptive: --- Hierarchical multiple regression: The model explained 47.9% of the variance in GHQ scores. As avoidance coping increased, so did GHQ scores. As support, self-efficacy, dispositional control and the interaction variable – ‘learning and teaching hassles and self-efficacy’– increased, scores on GHQ decreased. Summary: Self-efficacy, dispositional control and support were important predictors, and avoidance coping was the strongest predictor of adverse well-being. Promoting support and self-efficacy are likely to have immediate benefits for student well-being. |
| Hamaideh et al. (2016); Nursing students’ perceived stress and coping behaviors in clinical training in Saudi Arabia [23] Descriptive, cross-sectional: Saudi Arabia |
Nursing students doing clinical training invited by the researcher n = 110 |
The Perceived Stress Scale (PSS) The Coping Behavior Inventory (CBI) Demographics |
Descriptive statistics Multiple linear regression analyses to determine variables that predict the perceived stress and coping behaviors |
Descriptive: Common type of stress was from assignments and workload (mean = 1.82, SD=0.89), followed by the stress from teachers and nursing staff (mean=1.51, SD=0.85); lowest levels of stress were recorded due to the lack of professional knowledge and skills, and due to taking care of patients, the highest stressful events were due to nature and quality of clinical practice (mean = 2.07, SD = 1.35) and worrying about bad grades (mean=2.06, SD=1.48). Common coping behaviors utilized by students were problem-solving (mean=2.64, SD=1.00), followed by staying optimistic (mean=2.19, SD=0.91) Multiple linear regression: Ways of choosing nursing and presence of relatives in nursing showed statistically significant effects; variables accounted for 12.4% of the total variance of the perceived stress (adjusted R2); the second analysis revealed stress related to peers, daily life, and mothers’ educational level together accounted for 13.5% of the total variance of coping behaviors (adjusted R2). Summary: There were significant differences in coping behaviors concerning the presence of relatives in nursing, living status and mothers’ educational level. A significant difference in perceived stress was found for students concerning their way of choosing nursing. |
| Rella et al. (2009); When does nursing burnout begin? An investigation of the fatigue experience of Australian nursing students [28] Descriptive, cross-sectional: Australia |
First, second and third-year BN students invited via e-mail in large Australian university nursing School n=431 |
Occupational fatigue exhaustion recovery scale (OFER) Nottingham health profile (NHP) Work demands Questionnaire Demographics |
Descriptive statistics Hierarchical multiple linear regression to determine factors predicting fatigue and recovery, emotional health and sleep quality |
Descriptive: 38% (n = 160) participants indicated to consider abandoning the course before completion, 35% (n = 150) indicated that fatigue was a very significant/complete reason for considering quitting, 45% (n = 192) participants reported that the programs equipped them very poor to cope with nursing strains. Multiple linear regression: Percentage of variance all the dependent variables (fatigue, recovery, emotional health and sleep) ranged from 36% (Fatigue) to 23% (recovery); NHP emotional health emerged as the major predictor in all the equations. Summary: Nurse training places students under significant psychosocial stress. To prevent fatigue from progressing in nursing programs, adequate mentoring and guidance may be used. |
| Tada A (2017); The Associations among Psychological Distress, Coping Style, and Health Habits in Japanese Nursing Students: A Cross-Sectional Study [27] Descriptive, cross-sectional: Japan |
Students registered in the Department of Nursing - Hyogo University n=181 |
General Health Questionnaire (GHQ-12) Brief Coping Orientation questionnaire Health Habits Questionnaire Demographics |
Descriptive statistics Multiple linear regression to determine factors associated with psychological distress. |
Descriptive: 61.3% (n=111) had a GHQ-12 score ≥ 4, mean GHQ-12 score of 5.5, three most common coping styles were acceptance, self-distraction and planning; least common coping styles were substance use, religion, and denial. Multiple linear regression: GHQ-12 score was positively associated with “Avoidance coping” (β= 0.39, p < 0.001) and negatively associated with “Active coping” (β= -0.30, p < 0.001), “exercise habit” (β= -0.25, p = 0.001) and “sleeping”(= -0.24, p = 0.002) after controlling for sex, year of study, living with family, and participation in club activities. Summary: Study described the association among psychological distress, coping style, and health behaviors in nursing students. |
| Yıldırım et al. (2017); The relationship between educational stress, stress coping, self-esteem, social support, and health status among nursing students in Turkey: A structural equation modeling approach [26] Descriptive, cross-sectional, Turkey |
Nursing students from Duzce University n = 517 |
Nursing Education Stress Scale (NESS) Coping Behavior Inventory for Nursing Students (CBI) Multidimensional Scale of Perceived Social Support (MSPSS) Rosenberg Self-Esteem Scale (RSES) General Health Questionnaire (GHQ) Demographics |
Descriptive statistics Structural Equation Modeling to demonstrate direct and indirect effects of RSES, NESS, and MSPSS on GHQ. |
Descriptive: RSES – mean: 17.61, SD: 4.55, NESS – mean: 14.77, SD: 4.19, MSPSS – mean: 65.12, SD: 12.22, CBI – mean, 16.54, SD: 4.67, GHQ – mean: 28.15, SD: 8.51 Structural Equation Model: Explanation ratio for GHQ by CBI, NESS, and MSPSS factors was found to be 51.5%. As an independent variable, RSES had a positive significant effect on NESS but negative effects on CBI, MSPSS, and GHQ. Summary: Results indicated that nursing students' stress coping levels were affected by self-esteem and social support; this interaction appears to affect general health status. |
| Multicenter Studies | ||||
| Reference & Study Design | Sample Size, Characteristics | Data Collection | Analysis | Results |
| Boulton et al. (2017) Nursing Students' Perceived Faculty Support, Stress, and Substance Misuse [21] Descriptive, cross- Sectional: USA |
Sample of registered National Student Nurses’ Association (NSNA) members n = 4033 |
Student Nurse Stress Index (SNSI) Personal Drug Use Survey Perceived Faculty Support Scale (PFFS) Demographics |
Descriptive statistics Linear regression: SNSI scores, mean-centered PFSS, and interaction and substance use scores as the outcome variable Logistic regression: SNSI scores, mean-centered PFSS scores, and interaction on the likelihood that participants would excessively drink or use marijuana or illegal drugs |
Descriptive: 1-40+ occasions: Alcohol (< five alcoholic drinks in a row) - 61% (n = 2,481), Marijuana - 18% (n = 723), Nonprescribed drugs - 10% (n = 408), Amphetamines or other stimulant drugs - 8% (n = 323), other illegal drugs - 5% (n = 213) Linear regression: The model was significant, but R2 accounted for less than 1% of the variance in combined substance use scores - with every 10-unit increase in SNSI scores; the combined substance use scores increased by 0.04 units Logistic regression: The model for stimulant use for academic enhancement was significant; R2 accounted for less than 1.6% of the variance, suggesting for every 10-unit increase in PFSS score; students reported a decrease of 0.09 units of stimulant use Summary: Nursing students reported a moderate level of stress and used non-prescribed drugs more frequently as the stress scores increased. Perceived faculty support was inversely related to the use of no prescribed stimulants. |
| Blomberg et al. (2014); Swedish nursing students’ experience of stress during clinical setting characteristics and the organization of the clinical education [24] Descriptive, cross-sectional: Sweden |
Nursing Students in the final term of education at three universities n = 185 |
Numerical rating scale (NRS–10) to rate stress during clinical practice Demographics |
Descriptive statistics Decision tree analysis, dichotomized NRS scale using the median as cut-off |
Descriptive: Seventy-nine (43%) students had a score above the median (score 6–10) and were considered to have a high level of stress. A maximum value of 10 was scored by four students, and a minimum value of 1, i.e., no stress at all, by 12. The level of stress was reported to be greater in hospital departments, especially where nurses worked in a team and departments overcrowded with patients. Decision tree analysis: Practice in clinical placements in hospital departments was the best predictor of a high level of stress; the absolute risk of stress was reported to be 57% in students with clinical placements compared to 13% in other clinical settings. NCFE (Swedish national final exam) increased the risk of stress to 71% compared to 50% in students working in non-NCFE institutions Summary: The risk of stress in nursing students during their clinical practice differs depending on clinical setting characteristics. Taking a national clinical final examination could present an additional source of stress. |
| Cruz et al. (2018); Quality of life of nursing students from nine countries: A cross-sectional study [22] Descriptive, Cross-sectional: Chile, Egypt, Greece, Hong Kong, India, Kenya, Oman, Saudi Arabia, USA |
Bachelor Students (nursing) Students (1) enrolled in BSN program of participating schools, (2) full-time students, (3) registered in 1st to 4th year of the program, (4) nationality of the country of residence n = 2012 |
Health Organization QOL-BREF (WHOQOL-BREF): self-administered questionnaire Demographics |
Descriptive statistics Multiple linear regression analyses to assess independent relationship between predictor variables and QOL dimensions |
Descriptive: Highest QOL was recorded in the physical health domain (M = 63.77, SD = 14.72), lowest in the social health domain (M = 58.87, SD=21.87), overall perceived QOL of life scores ranged from 3.09 (SD = 0.82; Hong Kong) to 4.30 (SD = 0.71, USA), overall perceived health scores from 2.87 (SD = 0.90; Hong Kong) to 4.17 (SD = 0.66; Greece). Multiple linear regression: Age, country of residence, and monthly family income showed statistically significant multivariate effects; adjusted R2 accounted for 20% of the variance. An increase of one year in the students' age corresponds to 0.02 decrease in overall QOL. Students with monthly family income of > 2000 USD revealed significantly better overall QOL (β = 0.31, 95% CI = 0.23, 0.39, p < 0.001). Summary: Age, country of residence, and monthly family income showed a statistically significant multivariate effect on the aspects of QOL. |
3. RESULTS
A total of 13 studies were included for the narrative review but we had to exclude five further studies due to an insufficient description of methodological details. The final narrative synthesis contains eight studies.
All studies were cross-sectional; no studies were found with follow-up procedures. Most of the studies (87.5%) recruited participants from nursing programs, and only one study [21] recruited students from a national register. All studies except one were limited to individual nations. Those were Australia, Japan, US, United Kingdom, Saudi Arabia, Sweden, and Turkey. The only multinational reference survey [22] included nursing students from the following countries: Chile, Egypt, Greece, Hong Kong, India, Kenya, Oman, Saudi Arabia, and US.
The studies included nursing students undergoing their bachelor’s degree. Sample sizes ranged from a minimum of 110 individuals [23] to a maximum of 4,033 participants [21], with the highest numbers from the register-based sample. Overall, the studies processed in the narrative synthesis included 7,640 participants. All referenced studies were observational and quantitative. The analyzed data were collected for the study purpose, using either electronic or paper-pencil questionnaires (Table 4).
Common health-related dimensions evaluated by the studies were stress [21, 23-26], social support [21, 25, 26], mental health [25-27], fatigue [28], QOL [22] and drug abuse [21]. The number of assessment instruments distributed to the study participants ranged from one [22] to five combined instruments [25, 26], excluding the questionnaires to collect demographic data. Concerning the collection of demographic data, only Gibbons et al. [25] did not outline details about the study sample. To analyze the collected data, studies described the use of statistical logistic and linear regression models.
The most commonly analyzed health-related association with nursing students, stress, was triggered by individual and environmental conditions. In a large study (n = 4,033) from the United States, Boulton et al. [21] reported moderate levels of stress with no relationship between stress and abuse of non-prescribed substances. Blomberg and Hamaideh et al. [24, 23] reported that stress levels of nursing students were linked to the clinical setting (hospital vs. community-based setting, n = 185) and the way students choose their program (self vs. others, n = 110). In Turkey, Yildirim et al. [26] described a relationship between higher stress levels and lower levels of self-esteem.
Followed by the perception of stress, some researchers analyzed the impact of social support in nursing education. Boulton et al. [21] described that a negatively perceived faculty support was related to increased use of non-prescribed stimulants in nursing students. In Saudi Arabia, Hamaideh et al. [23] found the student coping capacity was negatively associated with fewer family members present during their education (R2 = 13.5). Yildirim et al. [26] reported that the general health status was moderated by perceived social support and the level of self-esteem.
In addition to studying social support and stress levels, Gibbons et al. [25] analyzed the psychological wellbeing of nursing students. The presence of coping avoidance was negatively associated with psychological wellbeing in nursing students. Tada [27] reported similar findings from Japan, adding that there was a positive relationship between psychological wellbeing and active coping techniques, including exercise and better sleeping habits. Finally, Rella et al. [28] described that Australian (n=431) nursing students were under significant psychosocial stress, with some students suffering from fatigue (Table 5).
In their ten-country study, Cruz et al. [22] found that QOL scores were correlated to the resident country, student age, and monthly family income. Increased age was negatively associated with QOL, while monthly family income above the US $2,000 was associated with higher overall QOL (β = 0.31, p < 0.001). Students overall scored lowest in the social health domain (WHOQOL: 58.87) and highest in the physical health domain (WHOQOL: 63.77). Across countries, the highest QOL scores were recorded in the United States (WHOQOL: 4.30), while Hong Kong had the lowest scores (WHOQOL: 3.09). Each additional year of age corresponded with a decrease of 0.02 points in the overall QOL score.
4. DISCUSSION
We aimed to describe the health status of undergraduate nurses during their qualification process and the effects of a nursing education program on perceived health-related indicators. We unexpectedly found a low amount of studies that reach a good and unbiased understanding of the health of nursing students, especially considering the proximity to research resources at nursing schools. From our perspective, studies should be easily implementable that could also include longitudinal designs to describe potential predictors about health-related dimensions of nursing education programs. The studies described were primarily stress related to the clinical experience in nursing students as moderate to high. Work stress has been significantly associated with cardio-metabolic risks and mortality [29]. Kivimäki et al. [29] analyzed data of 102,633 individuals; the risk of job strains was greater than hypertension, high total cholesterol concentration, obesity, physical inactivity, and high alcohol consumption. Varying by the study design and cohort, the stress level in nursing students was linked with the clinical environment, the way of selecting nursing education programs [23, 24], and self-esteem [26]. Ruotsalainen et al. [30] collected evidence on interventions to prevent occupational stress in healthcare workers. Cognitive-behavioral training, mental and physical relaxation, and changing work schedules were common interventions to reduce stress in healthcare work environments.
In line with the European and American Heart Association guidelines, psychosocial stress is a potential barrier to healthy lifestyles, especially for people with pre-existing conditions. Nursing students should thus be guided to screen systematically for stress and supported with methods of stress reduction. This could include interventions like consultation, job redesign and reductions in working hours [29]. The resulting stress-reduction of the nurses might increase the likelihood of clinical integration of similar methods and techniques (i.e. consultation, mindfulness-based stress reduction interventions), which could be especially relevant for vulnerable groups, such as people with stroke or cancer [30].
In our review, Cruz et al. [22] described the quality of life of nursing students between various countries, summarizing that the highest quality of life of nursing students was found in the US, and the lowest rates in Hong Kong (China) and Chile. The effect of societies and regional influences upon individuals' quality of life will remain a topic of study for many years. One such study, the OECD Better Life Index survey, has been collecting data since 2011 [31]. The survey [describes levels of satisfaction between 35 countries in dimensions like housing, income, and clinical environment. The survey shows the US performing above the worldwide average, considering income, health status, jobs and environmental quality for the general population. The regions with the lowest rates in these categories are South Africa and Mexico, whereas China and Egypt are not part of the OECD Better Life Index, and thus not comparable with the nursing student sample of Cruz et al.; Chile’s performance is outlined in the OECD ranking [32]. When asked, Chileans gave satisfaction of life a 6.5 grade of a 10-grade maximum, which is in line with the OECD average. In contrast, Cruz et al. [22] described the quality of life in nursing students living in Chile as the second-lowest, followed by Hong Kong. This difference among nursing students remains unclear and is likely related to methods of data collection and sample size.
The relation between macroeconomic indicators, like gross domestic product (GDP) and income inequality, and the health-related outcomes has been described before [33]. However, differences between the work and education environments should be further reduced. Our review collected evidence about the high level of health-related quality of life in countries, such as the US. Countries with lower rates might learn from the education qualification procedures in the US. This would prevent nurses from job-related burdens or even leaving their profession due to low health status.
4.1. Quality of Evidence
The quality of the evidence was low with only cross-sectional studies, although some studies provided information from a large sample [21, 22, 26]. Furthermore, most studies collected data from a single institution, implying issues with interpreting the data in the light of dominant cluster effects due to the institutional characteristics (e.g., teachers, concepts, and infrastructure). In some cases, articles did not report data about the institutional characteristics [23, 25, 27, 28], which negatively impacted the significance, comparability and usefulness of the results in different contexts. Minimal information was presented on institution characteristics or rankings of the schools, including key numbers, such as teacher-student ratios. We also found a lack of information describing student opinions about factors influencing their satisfaction with the program conditions. Studies predominantly collected data through psychometric assessments, including stress, anxiety, coping, and social dimensions. To support a more practical approach, psychometric assessments should be complemented by known health-related burdens and students’ opinions about them. This could be aspects like work shifts, conflicts with colleagues, and financial issues. Due to the absence of such connections in these studies, the practical implications for students are limited.
4.2. Limitations
Despite an extensive and inclusive search strategy, relevant studies may have been excluded due to decisions related to the methods. To minimize the risk of missing data, six large databases were searched, and 5,136 articles were screened for relevant content. The broad search strategy was intentional to cover the relevant literature. Due to a large number of publications and similar study designs, relevant publications may be underrepresented.
The main weakness of this narrative review was the subjectivity in study selection [17]. To reduce this risk of bias, the literature search and quality assessment strategy were transparent and fully reported. However, the cut-off point for the STROBE checklist was a subjective threshold [19]. A different cut-off point for the STROBE checklist might have resulted in the proper exclusion of the five studies with an insufficient description of methods during the selection process. Therefore, tools with predefined measures and scores would likely increase the methodological quality of this review.
CONCLUSION
This review of the current evidence about the health status of undergraduate nurses and the effects of a nursing education program on perceived health-related indicators revealed minor associations of the health status with stress and clinical setting, the stress level and self-esteem, health-related behaviors, and the way in which students selected a career in nursing. Nurse educators should be aware of these associations and support routine screening of students and their health status. Interventions, such as consultation and study redesign might increase the level of health in nursing students. It is vital that nursing schools further collaborate to investigate such associations and tailor interventions to positively affect health-related dimensions (stress, self-esteem, health-related behaviors) in nursing students.
AUTHORS' CONTRIBUTIONS
Markus Wübbeler: Conceptualization, methodology, formal analysis, writing - original draft, supervision. Sebastian Geis: Methodology, formal analysis, data curation, writing – review & editing. Björn Teigelake: Formal analysis, writing – review & editing. Sabine Schoening: Conceptualization, formal analysis.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIAL
The data supporting the findings of the article is available in the Zenedo at https://zenodo.org/ record/5550005#.YVxD4H1CSUk, reference number md5:b1bad38102e500a7489d2f412593015b.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.
SUPPLEMENTARY MATERIAL
Supplementary material is available on the publishers web site along with the published article.

