All published articles of this journal are available on ScienceDirect.

Pain Management Interventions for Drug-addicted Patients Admitted in Intensive Care Units: An Integrative Review
Abstract
Background:
Pain management interventions among critically ill drug-addicted patients admitted to ICUs are still the major challenge faced by healthcare practitioners.
Objective:
Therefore, this study aimed to identify and appraise the pain management approaches of patients with drug addiction (substance use disorder) admitted in ICUs.
Methods:
An integrative review of the literature was performed; narrative data synthesis was used for data extraction. The search was performed using scientific databases, including Google Scholar, PubMed, Scopus, Web of Science, Ovid Medline and EMBASE from January 2000 to September 2019. All studies that assessed pain management interventions for drug-addicted patients (substance use disorder) admitted in ICUs were included in the review.
Results:
Initially, four studies were included in this review. All these studies were Randomized Controlled Trials. The settings were intensive care units in the United States and Iran. The evidence identified from all studies included administration of intravenous paracetamol and midazolam, implementation of Buprenorphine-Naloxone therapy, adjuvant therapy and proper utilization of nursing sedation and pain management interventions for addicted patients admitted in ICUs.
Conclusion:
Management of pain in drug-addicted patients admitted in ICUs is relevant to healthcare practitioners, especially critical care nurses, as these patients’ subpopulation is at risk of underestimation of pain levels and not getting appropriate treatment.
1. BACKGROUND AND RATIONALE
Drug addiction (substance use disorder) is caused by the frequent use of an addictive substance or harmful use of psychoactive substances such as alcohol, marijuana, hallucinogens, and opioids [1, 2].
The use of these substances and drugs has several aftermaths on health; these are often chronic and persistent. The effects of drug abuse on health may include a damaged immune system, cardiac diseases including heart attacks, heart valves disease and heart muscle disease especially the injection drug use. Furthermore, other consequences of drug abuse include nausea, abdominal pain leading to anorexia and weight loss, increased strain on the liver which causes the risk of liver damage or liver failure, seizures, stroke, altered mental illness, brain damage, lung dysfunction, impaired memory and decision making. Worldwide effects in the human include enlargement of breast tissue in male, fever, and the most severe health consequence of drug addiction or abuse is death [1].
Pain management in the intensive care unit among the addicted patients is more significant than ensuring human care because failure in managing pain of this vulnerable population will lead to catastrophic consequences. For example, inadequate pain management of addicted patients will cause relapse to addiction due to re-exposure because most of the patients are being exposed to drugs and other substances before admitted to critical care units. Subsequently, this will lead to prolonged mechanical ventilation, delirium, depressed immunity, and increased length of stay in ICU, decreased level of consciousness, infections, and hemodynamic instability. Hence more attention and effective use of analgesia are required for these individuals in order to achieve the desired results and prevent further addictions [3, 4].
Furthermore, the knowledge and skills of ICU nurses toward pain management interventions in addicted patients are highly needed in order to ensure that patients are free from pain regardless of their previous history of substance abuse. The following are the nurses’ roles in managing pain of the addicted patient admitted in ICU; to perform a comprehensive assessment regarding pain of the patients, to apply evidence-based pain management intervention, to maintain the patient’s safety, to reduce ambiguity and contradiction between patient and staff, to promote clear communication between all team members, including the patient and family, especially regarding goals and plan of care, to follow the relevant pharmacologic principles, to be aware of tolerance issues and to consider multidisciplinary consultation including mental health, social work, pharmaceutical and spiritual care [5].
Orsini et al. (2017) from US found that 3 – 14% of ICU admissions were related to substance use disorder (SUD) or addiction. The most common substance identified in urine or serum toxicology screen was Opioids 33%, Marijuana 16%, Benzodiazepines 18%, Methadone 22% and Cocaine 24% [6]. This statistics shows that drug-addicted patients or patients with substance-use related disorders have a higher rate of admission to intensive care units. Therefore, healthcare practitioners need to be aware of pain management approaches to attend this vulnerable population in order to avoid pain underestimation and undertreatment [7]. Pain and addiction are interconnected because most of the patients especially those with chronic pains who are treated with opioids for a prolonged period get addicted, although most of the patients experience addiction due to previous exposure to opioids use. Hence this causes analgesic drugs to become unresponsive and creates a major challenge in the treatment of pain of addicted patients [8].
Empirical evidence highlights that effective utilization of pain management approaches among drug-addicted (substance use disorder) patients in ICUs is still a challenge following nurses’ underutilization of the interventions. For example, most of the ICUs use Opioids for pain management regardless of the patient’s past history, but the use of these drugs for a long time and a higher dose can cause exacerbations to addicted patients. The healthcare practitioners including physicians and nurses are confronted with a serious management challenge and they must use the standard guidelines in order to provide adequate pain relief to this vulnerable population [9, 10]. To clear the gap in practice, this study aimed at assessing the pain management approaches employed by critical care nurses for managing pain among drug-addicted (substance use disorder) patients admitted in ICUs. It is expected that the article will create a foundation that will be useful to identify the evidence-based nursing interventions which will be applied for pain management among drug-addicted (substance use disorder) patients in different ICUs.
1.1. Aim of this Review
The aim of this integrative review is to identify and appraise the pain management interventions of patients with drug addiction (substance use disorder) admitted in ICUs in order to improve the critical care nurses’ knowledge and performance.
1.2. Objectives
(1) To identify the existing literature that clearly facilitates the evidence-based pain management interventions towards drug-addicted (substance use disorder) patients in ICUs.
(2) To appraise the pain management interventions that do not cause addiction exacerbations to drug-addicted (substance use disorder) patients in ICUs.
2. MATERIALS AND METHODS
3. PICO
PICO technique was applied in this integrative review as the evidence-based approach to provide a clear answer regarding the patients’ clinical problem. PICO frame comprises of four types of clinical information which includes; firstly the patient or population to be studied, secondly the intervention to be applied in the study, thirdly the comparison criteria of the study (if appropriate), and fourthly the outcome which needs to be accomplished or improved [11]. Henceforth the PICO developed for this integrative review is shown in Table 1 below.
3.1. Population
The population in this study included adult patients with drug addiction (substance use disorder) admitted in ICUs regardless of their gender. The area of interest was pain management approaches towards drug-addicted (substance use disorder) patients.
3.2. Intervention
The intervention in this study was to identify and appraise the evidence-based interventions that will lead to achieve optimal pain relief among drug-addicted patients in ICUs.
3.3. Outcomes
What was measured in this study is the achievement of effective pain management interventions towards drug-addicted patients.
3.4. Review Question
In adult patients with drug addiction (substance use disorder) admitted in ICUs, what are the effective interventions for pain management?
3.5. Search Strategy
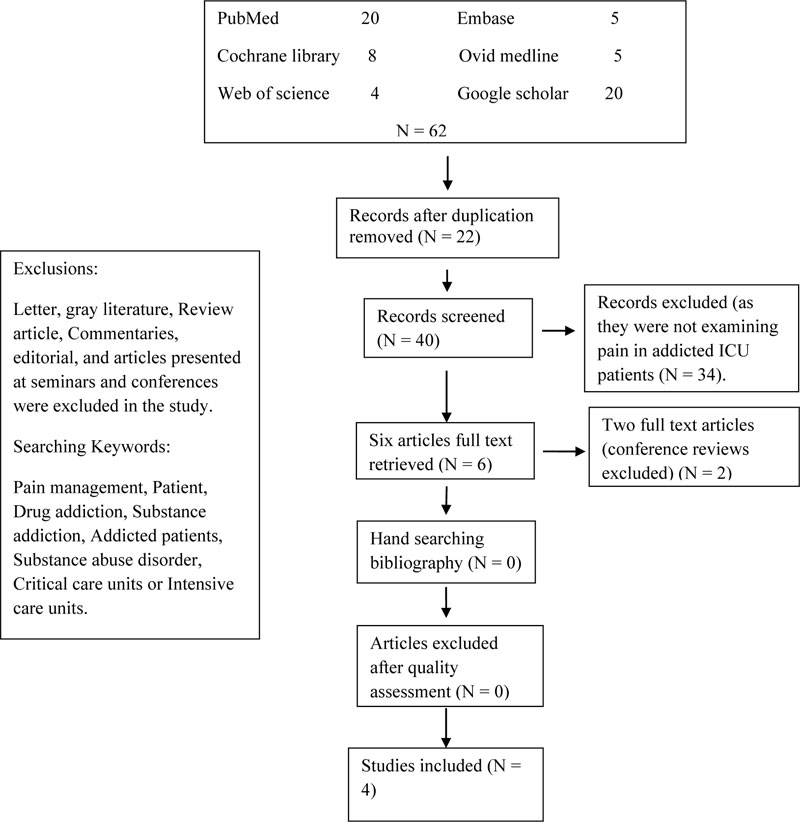
This article integrated all peer-reviewed published papers centered on pain management interventions for drug-addicted patients. The electronic databases that were used for the search of peer-reviewed papers included PubMed, Cochrane Library, Web of Science, Ovid Medline, EMBASE and Google Scholar. The following keywords were used for search in electronic databases as follows; ((“Pain management”) AND (patients)) and (drug addiction)). All search results, including title and abstract, were entered into Endnote-7 software. English articles on pain management with a target group other than addicted patients were excluded. At first, the search outcome was imported into Endnote (n=62). By eliminating duplicate articles, abstracts of 40 studies were screened. In case of any ambiguity in the abstract or the title, the full text of the study was downloaded and reviewed by two authors. Once ambiguity was cleared, the study was then further screened; otherwise, it would be eliminated from the study. Ultimately, according to the inclusion and exclusion criteria, 12 studies remained and were further screened for quality and inclusion in the study.
a. The full text of these studies was assessed with PRISMA. All 12 studies were scored separately by two authors. In case of any disagreement, the points were discussed until the consensus was reached. Finally, 4 original articles were included in the study (Fig 1).
| P | Patient (population or problem) | Adult patients with drug addiction (substance use disorder) admitted in ICUs. |
| I | Intervention | Identifying effective interventions to achieve optimal pain relief |
| O | Outcome (s) | To attain optimal pain management with the utilization of appropriate evidence-based interventions. |
| Evidence level | Description |
|---|---|
| Level 1 – Experimental Designs | Level1.a– Systematic review of Randomized Controlled Trials (RCTs) Level1.b– Systematic review of RCTs and other study designs Level 1.c – RCT Level 1.d – Pseudo-RCTs |
| Author/ Year/ Location | Patient group and age | Study design | Findings | Strengths and weaknesses |
|---|---|---|---|---|
| Rafiei et al. (2013) Iran [12]. | Addicted mechanically ventilated patients aged between 15-45 years. |
Randomization and blinding Double-blind randomized study was implemented. Sample size and attrition 37 Opium addicted critically ill patients, no attrition observed. Drug dosages Morphine 3.5-4.6 mg and midazolam 2.7-4.0 mg Interval time for administration Single dose of morphine and midazolam was administered every 6 hours for 48 hours; it was recorded in mg. |
Patients whose nursing sedation and pain protocols were maintained, they received less dose of morphine and midazolam compared to patients whose protocols were not implemented. |
Strength of the study Patients with a past medical history of kidney, lung, heart and liver were excluded from the study to avoid injury to these organs. Weakness of the study -Study involved only surgical related patients with multiple trauma and subdural hemorrhagic. -Study included a small sample size. |
| Griffin et al., (2016) US [13]. | Patients with opioid use disorder who were ≤ 18 years old. |
Randomization and blinding Double blind randomized study. Sample size and attrition 148 opioid dependent patients, there was no attrition Drug dosages Buprenorphine-naloxone treatment 8-32mg daily. Interval time for administration The medication was administered once per day. |
85% of respondents ever complained of mild pain, 58.1% ever complained to have moderate pain, 29.7% ever complained to have severe pain and 15.5% ever complained to have any pain. |
Strength of the study Exclusion of the patients with mental illness from the study. Weakness of the study The study took a long period of 4-12 weeks, hence this can lead to more adverse effects on the patients. |
| Imani et al., (2011) Iran [14] | Orthopedic patients having addiction problems with age between 20 and 50 years. |
Randomization and blinding Single-blind randomized study. Sample size and attrition 90 post-operative male addicted patients, no attrition occurred. Drug dosages Dose of 1st group was 20 mg of morphine sulfate +50 mg of chlorpromazine + 50 mg of promethazine +10 mg of midazolam. Dose of 2nd group was the first group’s regimen plus 150 micrograms of clonidine. Dose for 3rd group was 40 mg of morphine sulfate. A pump with a flow rate of 5 mls/h was chosen Interval time for administration The medication was given after every 12 hours within 2 days. |
Addition of chlorpromazine, promethazine, midazolam and clonidine in morphine infusion relieves pain and increases satisfaction of drug-addicted (substance use disorders) patients. |
Strength The combination of drugs administered to addicted patients managed to relieve pain. Weakness The study did not recruit female patients. |
| Kouchek et al., (2013) Iran [10] | Postoperative patients with mild to moderate pain; the ages were 42.4. |
Randomization and blinding Single blinded randomized prospective study. |
-Intravenous paracetamol may be safe as fentanyl for treating mild to moderate pain. |
Strengths -Pain assessment was done before drug administration. |
| Kouchek et al., (2013) Iran [10] | (+/-16.2) for paracetamol and 41.7 (+/-15.4) for fentanyl. |
Sample size and attrition 40 post-operative ICU patients, no attrition. Drug dosage 1st group received intravenous paracetamol 1gm in 100 ml of normal saline and 2nd group received intravenous fentanyl 25 mcg. Interval time and administration. Intravenous Paracetamol was administered after every 15min for 6 hours and intravenous fentanyl 25mcg was given 3 hours for 48 hours. |
-Also intravenous paracetamol may reduce the doses of narcotics in postoperative patients. | -Laboratory investigation to protect the liver was done. Weakness The scale used for pain assessment was not suitable for ICU patients (Visual Analogue Scale). |
3.6. Data Extraction and Analysis
Two independent authors extracted data on study design and year of publication of all articles published in peer review journals in English from 2010 to 2019, their sample size and findings. The reasons for the exclusion of articles have been explained above. One study was performed by a nurse [12]. We used Joanna Briggs (JBI, 2017) appraisal tool to appraise the articles. JBI’s critical appraisal tools assist in assessing the trustworthiness, relevance and results of published papers. The checklist for analytical case report studies has 8 questions and 13 questions for Randomized Control Trial studies. All studies were reviewed by two authors and if there was found a disagreement, the articles were again reviewed.
3.6.1. Data Items
The information was summarized in data extraction sheets.
3.6.2. Primary Measures
The primary findings in this study were the assessment of pain management among patients admitted in ICUs with a history of drug addiction.
3.6.3. Participants
Drug-addicted (substance use disorder) critically ill patients admitted in intensive care units were included in the study.
3.7. Ethical Consideration
This research was approved by the ethics committee of Tehran University of Medical Sciences (No: 98-3-163-45742).
3.8. Analysis
Data was presented in the form of a narrative. Meta-analysis was not possible due to the heterogeneity of clinical results that was found in small-scale trials included in this integrative review.
3.9. Inclusion and exclusion criteria
3.9.1. Inclusion
- Research related to pain management interventions among drug-addicted patients
- Case control studies and Randomized controlled trials
- Research papers in full text and published in English
- Papers published in peer-reviewed journal
3.9.2. Exclusion
- Studies that did not examine pain management interventions in adult patients with drug addiction (substance use disorder) admitted in ICUs.
- Studies that examined pain management in patients admitted in general wards.
- Studies presented at seminars and conferences.
- Studies that did not include intensive care unit settings.
4. RESULTS AND CRITICAL APPRAISAL
Out of 62 studies that were searched on databases, only four (4) studies met the inclusion criteria for the final analysis. Among these four RCTs, three studies were conducted in Iran and one in the United States. These studies reported on the pain management interventions among drug-addicted (substance use disorder) patients admitted in critical care settings. The findings gathered from these four studies were as follows; effective implementation of nursing sedation and pain protocols, utilization of Buprenorphine-naloxone therapy, infusion of morphine, plus clonidine, chlorpromazine, promethazine and midazolam, and administration of intravenous paracetamol. The strengths and weaknesses of each reviewed study have been explained.
4.1. Effective Implementation of Nursing Sedation and Pain Protocols.
Rafiei et al. (2013) revealed that nursing sedation and pain management protocols for opium addicted critically ill patients must be well implemented in an attempt to enhance pain management. This could lead to adequate pain relief among addicted patients, and it also reduces exacerbations. The study demonstrated that the effective implementation of nursing sedation and pain protocols among opium-addicted critically ill admitted in ICU will reduce the accumulation of sedative drugs and antipain medication. Noteworthy, it will minimize and reduce the severity of pain among opium-addicted patients [12].
In this study, Richmond Agitation Sedation Scale (RASS) and Behavioral Pain Scale (BPS) were used to assess the pain and sedation levels in opium-addicted patients hospitalized in ICU. During the admission of patients, the mean score of the RASS was -1.74 +/-1.1 in group 1 where nursing protocols were implemented and it was -1.81+/-1.1 in group 2 where no protocols were applied. But after hospitalization in ICU, the mean score of the RASS was -1.10+/-1.0 in group 1 where nursing protocols were implemented and -1.63+/-1.1 in group 2 where no protocols were applied. Regarding BPS during admission, the mean score in groups 1 and 2 was 7.9+/-1.3 and 8.0+/-1.6, respectively. After hospitalization, the mean score for PBS was 5.8+/-1.6 in group 1 and 6.9+/-2.1 in group 2 [12].
Henceforth, these findings revealed that patients in group 1 where nursing sedation and pain protocols were implemented received a smaller dose of morphine and midazolam compared to group 2 patients where no protocols were applied. The strength of this study was that patients with a past medical history of kidney, lung, heart and liver were excluded from the study to avoid deterioration and further injuries. But one weakness was that this study recruited only surgical related patients and also included a small sample size (n = 37) [12].
4.2. Utilization of Buprenorphine-Naloxone Therapy
Griffin et al. (2016) demonstrated that Buprenorphine-naloxone therapy with counseling in opioids dependent patients produced the desired outcome of optimal pain relief. The study took a period of 12 weeks involving opioids dependent patients. The aim of the study was to investigate the effect of Buprenorphine-naloxone therapy on opioids dependent patients. The dose of 8-32mg of Buprenorphine prescribed by physicians was administered to opioid dependent patients. All heroin dependent patients for more than one month with ≥ 18 years were recruited in the study.
The finding demonstrated that the severity of pain was associated with the increase in the dose of opioids among patients. In addition, the study confirmed that the administration of Buprenorphine-naloxone therapy provide good clinical results with respect to pain relief among opioid addicted patients. The study was conducted among racially homogeneous individuals in United States and found to be effective in relieving pain. They also explained that treating pain in addicted patients is still a challenge among critical care nurses; hence this leads to adverse effects such as chronic pain and delirium in critically ill patients because their pain intensity is underestimated and undertreated [13].
The strength of this study was that the patients with mental illness were excluded from the study to avoid further exacerbations or deterioration of their condition, while the weakness was that the study’s duration was a long period of 4-12 weeks hence this could lead to more adverse effects in the patients.
4.3. Administration of Clonidine, Chlorpromazine, Promethazine and Midazolam to Morphine infusion
Noteworthy, the study by Imani et al. (2011) evaluated the analgesic effects of adding chlorpromazine, clonidine, promethazine and midazolam in morphine infusion. This study recruited post-operative orthopedic patients with drug addiction disorders. The patients involved in this study were 90 addicted patients. These patients were distributed into three groups. Group 1 received 20mg of morphine sulfate + 50mg of promethazine+10mg of midazolam. Group 2 received the same dose as group 1 + 150mg of clonidine. Group 3 received only 40mg of morphine [14].
The study demonstrated that pain management among addicted patients had been difficult as these patients possessed another health issue apart from having pain. The study findings showed that instead of increasing the morphine dose, it is better to add promethazine, clonidine, chlorpromazine and midazolam in the morphine infusion. This is due to the strength of this analgesics cocktail that most addicted patients were more satisfied with the analgesic effect of these medications on optimal pain relief [14].
The strength of this study was that the combination of these analgesics drugs including clonidine, chlorpromazine, promethazine, midazolam and morphine showed a good response to pain relief and increased satisfaction of addicted patients. However, the weakness was that the study did not recruit female patients.
4.4. Utilization of Intravenous Paracetamol
Finally, Kouchek et al. (2013) evaluated the intravenous paracetamol therapeutic effect and its adverse reactions in contrast to fentanyl among ICU patients with mild to moderate pain. The Visual Analogue Scale (VAS) was used for pain assessment before the administration of analgesics. In 1st group, intravenous paracetamol 1gm was given every 6 hours for 48 hours, while in the 2ndgroup, intravenously fentanyl 25μg was given every 3 hours for 48 hours. The participants included were managed for any adverse effects involving the central nervous system and liver. The clients’ age, sex and pain level were coordinated in both the groups [10].
During the first 24 hours, the pain score was 2.60 (+/-1.2) and 2.40 (+/-1.5). After 48 hours, the pain score was 2.25 (+/-0.96) and 2.05 (+/-1.1) in paracetamol and fentanyl groups, independently. Henceforth, the results demonstrated that the therapeutic effects of intravenous paracetamol and fentanyl on pain relief were the same. The study revealed that the administration of intravenous paracetamol is safer and effective for treating mild to moderate pain among opioid addicted patients as it minimizes and reduces the dependence of opioids administration in ICUs. Subsequently, the study emphasizes the use of midazolam for sedating patients in order to decrease the use of opioids to achieve sedative effects [10].
The strength of this study was that the severity of patients’ pain was diagnosed and scored before drug administration. In addition, laboratory investigation was done to protect the liver from injury as frequent paracetamol use leads to liver failure. Regarding the weakness, the scale used for pain assessment was not suitable for diagnosing pain in ICU patients (Visual Analogue Scale). Instead, the tools like behavioral pain scale (BPS) and critical care pain observation tool (CPOT) could have been used [15].
5. DISCUSSION
Unluckily in this integrative review, it was not possible to conduct a meta-analysis due to clinical heterogeneity that arose. As for meta-analysis to be conducted, clinical interventions, outcomes and respondents that are similar in nature are required. In this integrative review, although most of the clinical interventions and outcomes tried to achieve the same results for identifying effective approaches towards pain relief among drug-addicted (substance use disorder) patients in ICUs, but still at the end, the nature of these interventions was different (shown in Table 3). Henceforth, a narrative analysis was conducted in order to identify the evidence-based nursing interventions that could be used to manage pain among drug-addicted (substance use disorder) patients in ICUs [16].
5.1. Levels of Evidence
The hierarchy of evidence is a foundation key of evidence-based practice, especially when looking for effective interventions towards clinical problems. In this integrative review, we only included RCTs as they are considered to be the highest on the hierarchy of evidence to answer intervention questions. In addition, we assessed the hierarchy of evidence using the Joanna Briggs Institute (JBI) criteria in order to find the scientific studies to be included in our integrative review which was found to be located on Level 1 as shown in Table 2 [17].
5.2. Clinical Effectiveness
Due to clinical heterogeneity of the findings and weaknesses as mentioned in Table 3, and the smallest sample sizes recruited in RCTs, this integrative review was insufficient to meet the criteria of being used as a reference for the effective approaches to pain management among critically ill addicted patients admitted in ICUs [18]. Even though the four (4) RCTs included in this review demonstrated the highest hierarchies of evidence according to JBI critical appraisal tools [19], but still this integrative review cannot be considered as the gold standard approach to be implemented by health practitioners in clinical practice.
5.3. Risk of Bias
All randomized controlled trials included in this integrative review reported adequate information required for assessment. These were concealment of allocation to treatment groups, analysis of the participant groups and the blinding fashion. However, two clinical trials applied double-blinded and the other two studies used single-blinded studies. In double-blinded studies, both participants and experimenters were not aware of the treatment allocation but in single-blinded studies, only participants were not aware of the treatment allocation. All these principles were applied to avoid allocation biases that can arise between researchers and participants [19].
There was no selection bias in the RCTs recruited in this integrative review due to the effective concealment of allocation that was implemented. Allocation concealment was implemented when the participants entered the trial (during recruitment) in all RCTs that were included in this review. Furthermore, RCTs were included in this review because it is the gold-standard design that is used to appraise effective therapeutic interventions but also it has the highest quality of evidence (Level 1b) as shown in the criteria used for selection of studies based on the level of evidence (Table 2) above [18, 19].
All of the studies included in this review provided the takeaway lesson; the age of the respondents who were recruited and the inclusion and exclusion criteria were mentioned. Some of the interventions that were reported as evidence-based in improving the pain management of drug-addicted (substance use disorder) patients included effective implementation of the nursing sedation and pain protocols, implementation of Buprenorphine-naloxone therapy, administration of morphine in combination with other drugs including chlorpromazine, clonidine, promethazine and midazolam, and utilization of intravenous paracetamol.
5.4. Limitations of the Integrative Review
This integrative review included resources that were published in peer-reviewed journals from 2010 to 2019. Therefore, gray materials, review articles, commentaries, editorials and articles presented at seminars and conferences were wasted and not included in the review.
Also, this integrative review was faced with a scarcity of published and unpublished resources or relevant papers that address the pain management approaches towards addicted patients in ICUs. Most of the studies focused on pain management in drug-addicted (substance use disorder) patients without classifying their clinical settings. Hence there was found inadequacy of effective pain management approaches to be added in this integrative review.
Finally, the studies included in this review involved a small sample size, hence this factor limited generalization to other clinical settings. However, the findings produced were rich in information on pain management approaches to drug-addicted patients admitted in ICUs. This limitation is similar to that of the study by Kukull and Ganguli [20].
CONCLUSION AND RECOMMENDATIONS
Pain management among drug-addicted (substance use disorder) critically ill patients in ICU is relevant to healthcare practitioners because this group of patients is more vulnerable to suboptimal pain management. This is partly attributed to the notion that administering opioid analgesics to this patient population often leads to harmful effects.
Interventions for optimal pain management in this patient population include adjunct therapy and creating awareness among physicians and ICU nurses regarding different terminologies used in drug abuse like Dependence, Tolerance and Addiction. This helps in equipping healthcare providers in ICUs with knowledge on pain management in the context of substance abuse while minimizing misdiagnosis in this patient population. Well-designed studies are needed to assess the effective pain management interventions among drug-addicted (substance use disorder) patients admitted in ICUs.
CONSENT FOR PUBLICATION
Not applicable.
STANDARDS OF REPORTING
PRISMA guidelines and methodology were followed.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

