All published articles of this journal are available on ScienceDirect.

Nursing Communication as a Tool for Patient Satisfaction. A Single Hospital Survey
Authors Info & Affiliations
Abstract
Background:
Communication is an essential tool for health promotion. Effective healthcare communication has great therapeutic value.
Objective:
The aim of the study is to assess the degree of patient satisfaction related to nursing communication in the various stages of hospital stay.
Methods:
Patients admitted to General University Hospital in medical and surgical department were subjected to this survey using a questionnaire, structured in four sections (acceptance, hospital stay, discharge, pain and new drugs management). Chi-square and multivariate logistic regression models were used to test the association between the outcome of interest defined as the satisfaction of nursing communication and the independent variables.
Results:
One thousand three hundred seventy questionnaires were administered. In acceptance, among patients satisfied with nursing skills related to explaining the department's functioning, most were satisfied with nursing communication (972 vs 87 p <0.005). Also during the hospital stay, among patients satisfied with nursing Skills and Manner relating to communication most were significantly satisfied with the nursing communication (849 vs 74 p <0.005 and 987 vs 55 p <0.001). At the discharge, the number of patients satisfied with nursing communication was greater among patients who considered the length of hospital stay adequate (1020 vs 65 p <0.001). Data are confirmed by the multiple logistic regression analysis.
Conclusion:
Our study shows how nursing communication is the key to establishing a good therapeutic care relationship and how it can be associated with patient satisfaction in various phases of hospital stay.
1. INTRODUCTION
1.1. Background
Care, compassion and effective communication are three essential elements of nursing care and the basis of skills that meet the standards of care [1]
Each nurse must show compassion and empathy towards the people he is called to assist. Nurse's empathy consists of interpreting the patient's needs through the use of numerous tools, including communication [2].
Communication is a pivotal skill of health professionals requiring awareness and practice [1]. It also has a remarkable possibility of influencing behavior and attitudes of the patients [3]. Even in distress, when nurses communicate effectively and actively listen, each one reports a positive experience.
In 2014, U.S. Joint Commission identified miscommunica-tion as the main cause of serious and unforeseen injuries to the patient and established improving effectiveness of communica-tion as the main goal [4]. Due to lack of completeness or different codes (for example, different spoken languages), a communication defect occurs when the issuer's signals do not reach the recipient comprehensively, can become difficult for the use of a short and fast or a too technical and over-abundant language. When the conversation no longer relies on the meaning of words but respects the rules of conversation and courtesy, it tends to become a conversation without communication.
Caregivers without equal attention to the individual in a holistic sense can determine incorrect behavior; Communica-tion, therefore, impacts the patient-nurse relationship, which should be based on intrinsic values such as trust, responsibility and support [5]. In this setting, communicative competence becomes a professional skill and changes attitude towards patients in a two-way process in which a message is sent, must be correctly received and understood [6].
When this occurs, patients gain confidence, feel respected and involved in the treatment process. They, also, can express feelings, improving therapeutic adherence and treatment outcomes [3, 6].
There are three types of communication: "verbal" "non-verbal" and "paraverbal" [7]. "Verbal" communication uses the "spoken word" channel; "non-verbal" is linked to emotions, from the face-to-face encounter with one's fellows and through the emotional state is manifested. Finally "paraverbal" consists of the use of the voice referring to the timbre, tone and pauses and volume. Without one of these components, communication becomes difficult to understand and cannot be understood by the patients [6].
Therefore, a verbal, non-verbal and para-verbal type of global communication approach, focused on the patient, is a powerful tool of the care system. Patients want to build a trusting relationship with the caregivers through communica-tion in order to switch from an object to the main leading actor [8]. Previous studies show how the communicative relationship with the patient has a strong impact in terms of satisfaction. On the contrary, a difficult communication results in greater dissatisfaction for the patients [6, 9, 10].
2. MATERIALS AND METHODS
2.1. Study Cohort
In this survey, consecutive patients admitted to a University General Hospital, from July 2018 to June 2019, were enrolled. Patients under the age of 18 years, with cognitive disorders, unable to write and read in Italian, admitted to intensive care and cardiac intensive care were excluded from enrollment. Data on age, gender, level of education, marital status, Body Mass Index (BMI) and reason for hospitalization were recorded. All enrolled patients completed an anonymous questionnaire delivered at the time of acceptance and collected at the time of discharge in special boxes placed near the information desk at the entrance to the wards.
2.2. Questionnaire Development
The questionnaire was constructed by a group of experts, made up of two experienced nurses, an epidemiologist, and members of the hospital management staff. For the collection of data, a two-part questionnaire was used: the first was dedicated to the collection of the socio-demographic characteristics of the sample examined, the second was composed of 40 items structured in four sections: reception (1-8); hospitalization (9-25), treatment of pain and administration of new drugs (26-33) and discharge (34-40) in which the answers are predefined through a Likert scale, to express a quality judgment on 5 levels: excellent, good, discreet, sufficient, insufficient.
The patient’s satisfaction with the behavior of healthcare personnel at the reception was regrouped to construct a binary variable, either "yes" or "no". The "yes" group consisted of patients who rated "yes" to the question "5- Did you immediately get all the attention you need from the healthcare staff?". Whereas the "no" group consisted of patients who rated "no" to the questions.
The patient’s satisfaction with the skill of healthcare personnel at the acceptance was regrouped to construct a binary variable, either "yes" or "no". The "yes" group consisted of patients who rated "yes" to the questions about N.1("having received information on the operation of the department at hospital admission") and N.7("satisfaction of information received from health personnel"), whereas the "no" group consisted of patients who rated "no" to one or both of these two questions.
The patient’s satisfaction with the behavior of healthcare personnel during hospitalization was regrouped to construct a binary variable ("Was the behavior of healthcare personnel during hospitalization satisfactory?"), either "yes" or "no". The "yes" group consisted of patients who rated "yes" to all the following questions N.10 ("were the nurses patient?"), N.14 ("did the nurses try to understand your situation?"), N.15 (" during visiting hours, nurses allow me and my family privacy and time to be together"), N.16 ("were available to meet the needs of the family during and outside visiting hours"), and who rated "often" and "always" to the questions, N.20 (" during hospitalization, how many nurses have treated you with courtesy and respect") and N.21 (" during hospitalization, how many nurses have listened you carefully".) Whereas the "no" group consisted of patients who rated "no" to at least one of the previous questions .
The patient’s satisfaction with the skill of healthcare personnel during hospitalization was regrouped to construct a binary variable, either "yes" or "no". The "yes" group consisted of patients who rated "yes" to all the following questions N.12 ("nurses worked together with continuity between shifts"), N.13 (" nurses provided personalized care to meet my needs"), N.17 (" nurses encourage family members and explain how to help the patient (nutrition, hygiene, moral support)", N.18 (" nurses support me psychologically in stressful moments (unpleasant procedures, medical visits)"; and who rated "often" and "always" to the questions N.22 ("during admission, how many nurses have given explanations (using understandable terms)" and N.23 ("during hospitalization, after pressing the call button, how many times she was helped as soon as she needed them").
The patient’s satisfaction with the behavior of healthcare personnel throughout the hospital stay was regrouped to construct a binary variable, either "yes" or "no". The "yes" group consisted of patients who rated "yes" to the question (" during hospitalization, doctors, nurses or other hospital staff members spoke to you if by chance you might need help as soon as you left the hospital"), whereas the "no" group consisted of patients who rated to the same question.
The patient’s satisfaction with the skill of healthcare personnel throughout the hospital stay was regrouped to construct a binary variable, either "yes" or "no". The "yes" group consisted of patients who rated "yes" to the question N.34 ("during hospitalization you received written information about the symptoms or health problems to watch out for after being discharged from the hospital"), whereas the "no" group consisted of patients who rated "no" to the same question.
After presenting to each patient a letter with the description of the project to ensure maximum information on the purposes of the study, a signature was obtained for the consent to complete the questionnaire.
2.3. Statistical Methods
Firstly, descriptive statistics, including frequencies, means, and standard deviations, summarized demographics, beliefs and perception about the hospital stay was performed. Secondly, chi-square was used to test the association between the outcome of interest defined as the satisfaction of nursing communication (OUTCOME I) and the independent variables. All independent variables with a p-value less or equal than 0.25 were considered eligible for inclusion into the multivariate regression analysis. Thirdly, multivariate logistic regression models have been built to investigate independent characteristics associated with the outcome of interest: " Satisfaction with nursing communication. The following independent variables were included in the Model: gender (male=1; female=2); age (20-30 years=1; 31-50 years=2; over 50 years=3); nationality (Italian=0 and foreigner=1); education level (compulsory education=0; university education=1 ;); type of hospital ward (surgical ward=1 and medical ward =2); type of disease (medical=1 and surgical =2); ease in identifying the role of the healthcare staff on the basis of the color of the uniform worn (yes=1 and no=0); place where the medical history was collected (doctor’s office room=1; nurses’ room=2; patient’s room=3); satisfaction with the behavior of healthcare personnel at the reception (yes=1 and no=0); satisfaction with the hospitality in the medical department (yes=1 and no=0); satisfaction for the reception in the medical department (yes=1 and no=0); evaluation of the management of the department (good=1 and bad=0); information provided by health personnel on how to become independent (yes=1 and no=0); psychological support provided by the healthcare personnel (yes=1 and no=0); satisfaction with the behavior of health personnel during hospitalization (yes=1 and no=0); satisfaction with the skill of health personnel during hospitalization (yes=1 and no=0); need for help from the healthcare staff to go to the bathroom (yes=1 and no=0); frequency with which the patient asked the healthcare staff for help to go to the bathroom (high=1 and low=0); pain felt during hospitalization (yes=1 and no=0); intake of new drugs during hospitalization (yes=1 and no=0); satisfaction with the behavior of healthcare personnel throughout the hospital stay (yes=1 and no=0); satisfaction with the skill of healthcare personnel throughout the hospital stay (yes=1 and no=0); satisfaction with the length of hospital stay (yes=1 and no=0); change in health following hospitalization (yes=1 and no=0); likelihood to recommend the hospital (yes=1 and no=0).
A stepwise procedure was applied to obtain the final models with p values for the variable inclusion and exclusion of 0.2 and 0.4, respectively. The results of the logistic regression analysis are expressed as odds ratios (OR) and their 95% confidence intervals (CIs). A two-tailed p-value of less than 0.05 was considered significant for all analyses. The data obtained from the questionnaire were analyzed using Stata software version 14.
3. RESULTS
3.1. Study Population
One thousand three hundred seventy questionnaires were administered and 1162 replies were received with a response rate of 84%. As shown in Table 1, of 1162 patients analyzed, 705 (61%) were male, with a mean age of 55 ± 12 years, and a BMI of 26 ± 2 (Kg/m2). Most, 1138 (97%), were Italian, about half (56%) had a high school diploma, only 181 (16%) had a degree. 642 patients (55%) were hospitalized in medical and 520 (45%) in surgical departments. 798 patients (68%) were treated for the medical disease and 364 patients (32%) for surgical, respectively.
| N(1162) | |
|---|---|
| Characteristics | |
| Age (years) | 55 ±12 |
| Gender n male (%) | 705 (61) |
| BMI (Kg/m2) | 26±2 |
| Nationality n (%) | |
| Italians | 1138 (97) |
| Foreigners | 24(3) |
| Education Level n (%) | |
| Primary school | 654 (56) |
| High school | l327 (28) |
| University or above | 181 (16) |
| Hospital Department n (%) | |
| Medical | 642 (55) |
| Surgery | 520 (45) |
| Disease Classifcation n (%) | |
| Medical | 798 (68) |
| Surgery | 364 (32) |
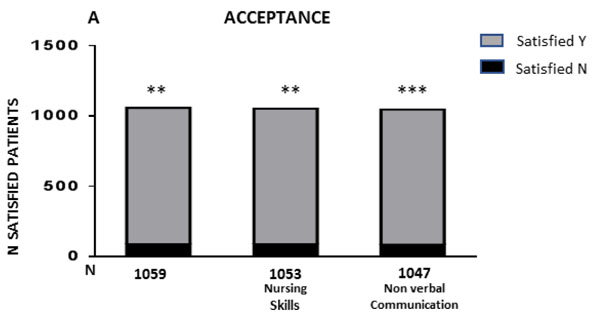
3.2. Acceptance
Most of the patients (1147/1162) (98%) were satisfied with the acceptance methods in each department.
As shown in Fig. (1), in univariate analysis, among patients satisfied with the organization and nursing skills related to explaining the department's functioning, most were satisfied with nursing communication (972 vs 87 p <0.005 and 966 vs 87 p <0.005) respectively. Furthermore, in the field of non-verbal communication, the majority of patients who had considered it easy to recognize caregivers by the color of the uniform, were satisfied with nursing communication (965 vs 82 p <0.001). No significant differences have been highlighted regarding the location and the rapidity of the attention given by the caregivers related to the satisfaction of nursing communication.
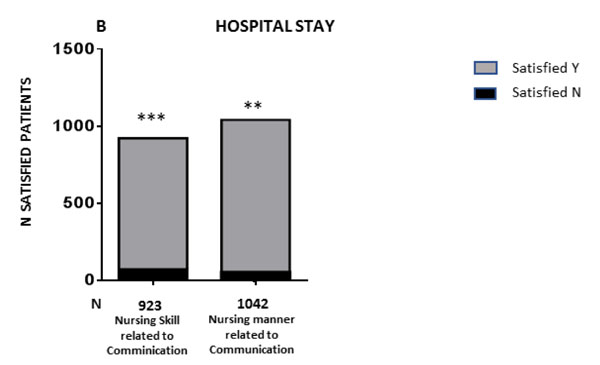
3.3. Hospital Stay
One thousand one hundred and fifty-three (99%) patients were satisfied with the health care received during the hospital stay. Also at this stage of hospitalization, among patients satisfied with nursing Skills and manner relating to communication most were significantly satisfied with the nursing communication. (849 vs 74 p <0.05 and 987 vs 55 p <0.001). Fig. (2).
(***= p <0.001).
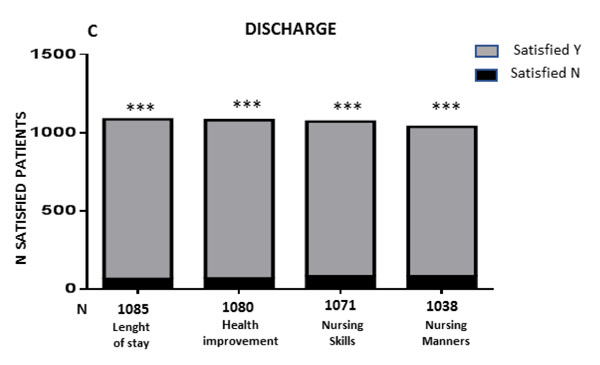
3.4. Discharge
90% of patients 1057/1162 were satisfied with the information received at the discharge. As shown in Fig. (3), number of patients satisfied with the nursing communication was significantly greater among patients who considered the length of hospital stay adequate (1020 vs 65 p <0.001), among those who believed that their health conditions had improved (1012 vs 68 p <0.001) among those who were satisfied with the nursing skills related to the explanation on discharge (988 vs 83 p <0.001) and, finally, among those who were satisfied with the nursing manner at discharge phase (955 vs 83 p 0.001).
3.5. Management of Pain and its Treatment
Eight hundred thirty-eight patients (72%) reported pain during their stay. As shown in Fig. (4), in the subgroup that reported pain, among patients satisfied with management and methods of explanation received most were satisfied with nursing communication, (723 vs 58 p <0.001 and 690 vs 66 p <0.001) respectively.
3.6. Multiple Logistic Regression Analysis
As shown in Table 2, "Satisfaction with nursing communication defined as outcome in the logistic regression model was negatively associated with "Ease in identifying the role of the healthcare staff on the basis of the color of the uniform worn" (OR 0.31 (95% CI 1,57-6,99), p <0.001) and, as expected, "Satisfaction with the nursing skills relating to communication during hospital stay" (OR 0.33 (95% CI 0,16- 0,67), p <0.001), as well as the intake of new drugs (OR 0.46 [95% CI 0,22- 0,97], p <0.004).

| Log-likelihood=-218.41, Chi-square=268.21, p<0.000, N of obs=1162 | |||
|---|---|---|---|
| OR* | 95% CI | P value | |
| Age 20-30 years 31-50 years Over 50 years |
1,00* 3,68 2,54 |
1,13-11,98 0,88-7,32 |
0,03 0,08 |
| Nationality Italian Foreigner |
1,00* 0,273 |
0,68-1,18 | 0,08 |
| Education level Compulsory education University education |
1,00* 1,50 |
0,69-3,25 | 0,30 |
| Type of disease Medical Surgical |
1,00* 1,66 |
0,92-3,01 | 0,09 |
| Ease in identifying the role of the healthcare staff on the basis of the color of the uniform worn Yes No |
1,00* 0,314 |
1,57-6,99 | 0,00 |
| Place where the medical history was collected Consulting room Nurses’ room Patient’s room |
1,00* 0,61 Backward elimination |
0,35-1,07 | 0,09 |
| Satisfaction with the nursing manner at the reception Yes No |
1,00* 0,12 |
0,00-12,29 | 0,37 |
| Was information provided by health personnel on how to become independent? Yes No |
1,00* 0,47 |
0,12-1,81 | 0,27 |
| Was the nursing relating to communication during hospitalization satisfactory? Yes No |
1,00* 18,73 |
9,74-36,05 | 0,00 |
| Satisfaction with nursing skill relating to communication during hospitalization Yes No |
1,00* 0,33 |
0,16-0,67 | 0,00 |
| Was help from the healthcare staff needed to go to the bathroom? Yes No |
1,00* 1,64 |
0,31-1,32 | 0,23 |
| Was any pain felt during hospitalization? (Domanda26) Yes No |
1,00* 0,53 |
0,26-1,11 | 0,09 |
| Were any new drugs taken during hospitalization? Yes No |
1,00* 0,46 |
0,22-0,97 | 0,04 |
| Satisfaction with the nursing skill related to explanation on discharge Yes No |
1,00* 2,20 |
1,04-4,69 | 0,04 |
| Was the length of hospital stay satisfactory? Yes No |
1,00* 14,21 |
6,11-33,07 | 0,00 |
| Was there a change in health following hospitalization? Yes No |
1,00* 4,20 |
1,72-10,24 | 0,00 |
| Likelihood to recommend the hospital to friends and/or relatives Yes No |
1,00* 2,34 |
0,96-5,74 | 0,06 |
Moreover, a significant association with the outcome was found with age, since the patients 31- 50 years were more satisfied compared to younger patients (OR 3.68(95% CI 1,13- 11,98), p <0.05), and with patients who believed that their health condition had improved N.37(OR 4.20(95% CI 1,72- 10,24), p <0.001). As expected, satisfaction of nursing communication were more likely among patients satisfied with the manner of health personnel relating to communication during hospitalization (OR 18.73 (95% CI 9,74- 36,05), p <0.001), with the nursing skill related to the explanation on discharge (OR 2.20(95% CI 1,04- 4,69), p <0.05) and with the length of hospital stay (OR 14.21(95% CI 6,11- 33,07), p <0.001. The gender of the patient and the type of hospital ward were removed from the logistic regression model, as well as the satisfaction with the healthcare personnel’s skill at reception and with their behavior throughout the hospital stay, the hospitality and the management of the medical department. Other variables that were eliminated from the model were the "Frequency with which the patient asked the healthcare staff for help to go to the bathroom", the "Did the healthcare personnel provide psychological support?"
4. DISCUSSION
Effective skills, interpersonal techniques and appropriate use of verbal and non-verbal communication are essential for providing adequate nursing care [11]. Our results, showed how nursing communication is significantly correlated to the satisfaction on the information received on the functioning of the department at the admission, on nursing skills and manner related to communication during hospitalization, on pain management, on the intake of new drugs, on information received at discharge, respectively. Furthermore, in the linear regression model, a significant association is shown with the age category between 31 and 50 years (OR 3.68 [95% CI 1.13-11.98], p <0.05), probably due to the number of patients belonging to this age group compared to the number of patients belonging to the younger class. However, we have not been able to highlight this data in previous studies. Moreover, in the linear model, all patients satisfied with the communication were those who considered the hospital stay useful and those who considered the information given by the nursing staff during hospitalization and at the time of discharge to be clear. Finally, importantly, they were satisfied with the length of hospital stay (OR 14.21 [95% CI 6.11 - 33.07], p <0.001. No significant correlation was found between satisfaction for nursing communication, sex, level of school education and physical environment. This data differs from a similar and recent institution based cross-sectional study. Fite et al, using a linear regression model, have shown that educational status, language difference, education difference and perceived patient view score were significant predictors of therapeutic communication implementation [12].
Similar to our data, a recent systematic review conducted with umbrella methodology confirms through quantitative and qualitative analysis of 12 systematic reviews that communication is the basis for the creation of a good trust relationship between patient and nurses for the definition of comfort, sense of respect and co-involvement in the management of the disease in order to improve care and treatment [2]. Although other evidence shows that most nurses working in general hospitals do not consider communication as a key element of clinical care [13, 14]
According to previous studies [15-18], as part of non-verbal communication, the ease of recognition of the operator from the color of the uniform is significantly correlated to satisfaction of the nursing communication.
Glowacki [19] in 2015, highlights how adequate nursing pain management during hospitalization improves patient satisfaction. In our study group, 72% of patients reported pain. Most of those satisfied with the management and the explanations about pain management were significantly satisfied with the nursing communication (723 vs 58 p <0.001 and 690 vs 66 p <0.001).
Our study, in a quantitative manner, highlights how dialogue performs a therapeutic and supportive function aimed to satisfy patients' needs, develop self-management during hospitalization.
In a global assessment, during the entire hospital stay, patients interviewed correlated satisfaction with the communication skills of nursing care rather than technical skills.
Finally, in our study nurses' point of view and degree of knowledge of specific communication skills implemented in the relationship established with the patients were not evaluated. Of note, finally, the results of the literature research show that communication is considered a fundamental parameter in determining the quality of the hospital structure [17].
CONCLUSION
Our quantitative data highlight the importance of communication as a tool to improve patient care. Only "the provision of a nursing technique" without adequate communication, is offered. Enabling health care professionals’ communication skills may promote a patient-centred approach to communication, allowing their involvement in communication throughout the hospital in identifying the better diagnostic and therapeutic approach, also in the management of pain. Quantitative data of this single-center survey, obtained with adequate statistical methodology, can be the starting point for the design of further intervention studies to improve nursing management protocols for hospitalized patients.
ETHICAL APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Institutional Review Board (no. 2018 08-018) University Medical Hospital "Mater Domini", Catanzaro, Italy.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Written informed consent was obtained from all the participants prior to publication.
AVAILABILITY OF DATA AND MATERIALS
The data Supporting the finding of the article is available in the paper archive of university Hospital Mater Domini "88100" Catanzaro, Italy.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
We are grateful to the patients who participated in this study. R Spagnnuolo has contributed to the design, analysis, and preparation of the study results. F Licata and A Barilaro have contributed to the analysis of results.

