All published articles of this journal are available on ScienceDirect.

Concept Analysis of Post-operative Recovery after Abdominal Surgery: State of the Science
Abstract
Purpose
This study aimed to analyze the concept of post-operative recovery among patients receiving abdominal surgery.
Methods
The concept analysis based on Walker and 'Avant's framework was adopted in this study. Data were explored and collected from different databases, namely, PubMed, Science Direct, Scopus, and SAGE Journals, by using the following keywords: “patients receiving abdominal surgery,” “post-operative recovery,” and “concept analysis.”
Results
The attributes of post-operative recovery after abdominal surgery varied depending on different phases of recovery.The antecedents included physiological factors, psychological factors, social factors, and habitual factors.The consequences were as follows: 1) decreased unpleasant physical symptoms; 2) restoration of bodily functions; 3) achievement of a level of emotional well-being; and 4) ability to resume normal activities.
Conclusion
Factors influencing post-operative recovery after abdominal surgery should be taken into consideration when developing medical interventions and further studied to favor future research development. The comprehension of concepts will guide health professionals formulate in evaluating the quality of nursing care, develop the desired tools for evaluating research outcomes, and formulate new theories.
1. INTRODUCTION
Digestive disorders are common among the global population. Consistent with Wang et al.'s study, digestive diseases are one of the significant causes of death among the global human population. These include Gastro- intestinal (GI) bleeding, GI sepsis, cancers, and abdominal trauma. Medical treatments vary, depending on the specific etiology of the disorder [1]. Surgery is typically performed with the intention to cure GI diseases; however, surgery poses potential effects on various systems in the body. The data supports a link between emergency surgery cases and increasing post-operative complications such as wound infection and sepsis, dehiscence, leaky gut syndrome, and ileus [2]. Apart from recovery, the purposes of surgery are promoting rapid restoration, reducing complications, and preventing hospital readmission.
Concept analysis involves identifying and classifying the attributes of concepts while promoting a profound understanding of the concepts and giving clear, precise operational definitions. This challenging task can provide a broad understanding of nursing phenomena, particularly patient recovery. Concept analysis is often referred to and considered one of the main objectives in different research fields. The literature reveals that most studies on abdominal surgery focus on post-operative recovery. However, neither the definition nor the criteria of abdominal surgery recovery have been clearly stated. For instance, there were two studies relevant to abdominal post-operative recovery, one focusing on the effect of preoperative education on recovery [3], and the other studying the effect of anxiety during pre and post-operative periods on the quality of recovery among patients having abdominal surgery [4]. Neither study however, gave full details about the attributes and the criteria of abdominal post-operative recovery. Though some studies on post-operative recovery have been conducted, the proposed results of concept analysis were not directly based on nursing phenomena associated with abdominal surgery. Therefore, the concept of abdominal surgery recovery requires analysis to gain real insights and illuminating views.
This study aimed to analyze the concepts of abdominal surgery recovery. The results will yield fresh insights into the definitions, characteristics, and scopes of post-operative recovery, which could promote comprehensive knowledge in all nursing phenomena, enable healthcare professionals to give proper care to abdominal surgery patients, and provide good ground for the development of new theories with effective tools for evaluating research outcomes.
2. METHODS
This study involved no human subjects. The 8-step method from Walker and Avant’s approach was applied to examine post-operative recovery concepts among patients receiving abdominal surgery.The definitions of abdominal surgery patients were explored from various literature. Then, the determining attributes and cases (model, borderline, related, and contrary) were analyzed, followed by the identification of antecedents and consequences of post-operative recovery among abdominal surgery patients.Finally, the empirical referents were introduced to clarify the measurement of abdominal surgery recovery.Data were gathered from credible sources (PubMed, Science Direct, Scopus, and SAGE Journals) with key terms: recovery, post-operative recovery, and abdominal surgery.Quantitative and qualitative research published in English (2013–2023) were examined for context-relatedness. Available, applicable full-text abstracts were screened to select papers. After checking for duplication, 19 studies formed the basis for concept analysis.
3. RESULTS
3.1. Identifying Uses and Definitions of the Concept
According to Walker and Avant (2019), all uses of a concept should be considered, not limiting the search to a particular field (not only nursing or medical) to obtain broad information. All aspects, both explicit (physical) and implicit (psychological), must be considered to get “the true nature of the concept.”
Several studies have identified the definitions and characteristics of post-operative recovery concepts, revealing that recovery concepts are used in different fields with broad definitions. Citing credible sources, “recovery” means the state of “becoming healthy after being sick or hurt” [5] or “return to normal health after injury or illness” [6]. Recovery can be a process of changes or improvement of health, wellness, and quality of life [7], as well as regaining strength and eliminating sickness [8].
Psychological patient recovery is both a process and a result, which requires assistance from others. The definitions involve patient changes, no repetitive disorders, and return to daily routines [9].
Returning to daily routines without help makes patients feel better, while signs of recovery include medication-free emotional regulation and expression [10].
The literature revealed that health science studies have also focused on recovery and relevant explanations. Recovery can be defined as physical and psychological adaptation enhancing bodily restoration and function as patients return to activities without assistance.Post-operative recovery involves returning to normal conditions, restoring preoperative physical function, and having no complications In addition, this process covers physical, emotional, and social aspects, as well as restoring normal function [11].
Alvin et al. explained that the attributes of post-operative recovery include physical, mental, and social dimensions as well as bodily functions.Physical recovery refers to the complete restoration of bodily function without post-operative discomforts and complications, whereas psychological recovery includes emotional stability, contentment, and the ability to cope with illness [12]. Socially, post-operative recovery involves returning to normal life, such as accomplishing daily routines and appropriate interpersonal relationships. Allvin, Ehnfors, Rawal, and Idvall described post-operative surgery as an ongoing process requiring tremendous effort to pursue daily needs. Physical, mental, social, and habitual aspects are essential in this process [13], which covers the restoration of mind and bodily functions. Energy consumption is needed for complete mental and physical well-being [11].
Rajabiyazdi et al. defined post-operative recovery among abdominal surgery patients and found that it involved returning to habits and routines, resolution of symptoms, overcoming mental strains, regaining independence, and enjoying life [14]. Alam et al. investigated the experiences of abdominal surgery patients to develop conceptual frameworks of post-operative recovery and found recovery to involve bodily functions, activity, and participation. Bodily functions involve pain, emotional function, energy and drive, defecation, and exercise tolerance. Activities and participation are linked to walking, changing basic body positions, daily routines, moving around, and dressing [15]. Some studies also pointed out that hospital discharge criteria, consisting of pain control, mobilization, and self-care ability, tolerance of oral intake, and good physical signs, are considered indicators of post-operative recovery [16].
As mentioned, abdominal surgery recovery is a body restoration and fitness process without post-operative complications. Pain and suffering are controlled, while contentment and emotional stability encourage appropriate emotional expression and social interaction. Daily routines are performed without assistance. The phases of abdominal surgery recovery can be categorized as the early, intermediate, and late phases of recovery.
4. DEFINING ATTRIBUTES
Walker and Avant identified concept analysis as characterizing or designating a cluster of attributes to describe a concept. Analysis requires examination of many patterns of concepts and records of all repetitive features of the concept [17]. The list of repetitively appearing characteristics of the concept defines the desired attributes.The significant attributes of recovery are categorized into three phases, as demonstrated in Fig. (1).
4.1. Early Recovery Phase
In assessing early recovery, the primary focus is the physiological domain. At this stage, patients display the ability to control reflexes and movement, thereby indicating improvements in bodily functions as vital signs are expected to stabilize within the preoperative range.In addition, laboratory test results are likely to be within acceptable ranges. Moreover, patients in early recovery are expected to be able to empty their bladders during urination with ease comparable to preoperative bladder function.
4.2. Intermediate Phase of Recovery
In assessing the intermediate phase of recovery, the primary focus is on the physiological and psychological domains. Patients generally display the ability to control pain, move, and be free from significant pain or tiredness as the physical state stabilizes with energy maintainability. Early ambulation, increased walking distance, deep breathing, coughing, ADL performance (going to the toilet, dressing, and showering), and self-care are key indicators of recovery. In addition, indications of restored lower gastrointestinal function include bowel movement, flatulence, and defecation. Psychologically, patients in this phase tend to exhibit overall well-being, greater comfort, less symptom distress, a change from illness to good health, no depressive symptoms, anxiety, fatigue, or passivity.
4.3. Late Recovery Phase
Observation of the physiological, social, and habitual domains is required in assessing late-phase recovery.Clear indicators of physiological recovery include renewed muscular strength for ADL performance (exercising, lifting heavy objects, and engaging in outdoor activities).The indicators of social recovery include maintenance of interpersonal relationships, active engagement in social interactions, and effort toward affirming identity and gaining acceptance. In habitual recovery, primary attention is given to the ability to perform tasks, regulate and perform daily routines such as personal hygiene and regular habits (eating, drinking, driving, and working).
4.3.1. Model Case
Somchai, a 47-year-old man, was hospitalized for colon cancer surgery. Before surgery, the patient was stressed and anxious about the diagnostic results and surgery for cancer treatment. As recorded, the patient had never had any surgeries before. Thus, he was highly concerned about negative outcomes. Fortunately, there were no compli- cations. Postoperatively, nurses provided advice on self-care, and he received good care from his daughters. The patient had pain for 2 days, then improved slightly. However, he continued to experience mild post-operative pain and needed more rest. On Day 3, some warning signs indicated restoration of normal bowel function, such as flatulence and defecation.The doctors advised eating soft foods and drinking water. Later, there were no symptoms of tightness, abdominal pain/painful flatulence, nausea, or vomiting. At first, the patient could gradually move his body, then could move freely and perform activities such as eating, going to the toilet, and taking care of personal hygiene. After the operation, the patient was informed that the tumor was Stage 1 and cancerous. The patient had been praying regularly for years before the admission, so he kept engaging in nightly meditation and prayer. As a result, he realized his actual condition and was able to accept his illnesses with ease. The patient was psycho- logically supported by family members, well-instructed in rehabilitation, and positively encouraged to regain his previous physical condition. He was eventually discharged from the hospital. His family played a role in supporting all practical activities, and he managed to return to normality. Six weeks after surgery, he was able to return to work as usual. After leaving the hospital, he adjusted his eating plan and focused on a nutritious diet to promote good health and wellness.
4.3.1.1. Analysis
In the above example, it was illustrated that the patient had a good recovery. The results met all requirements, as defined in the attributes. In the physiological domain, pain became less and less. The gastrointestinal system returned to normality, and the body started to tolerate food and drink. Psychologically, although it was the patient’s first surgery, he was able to adapt quite well and successfully apply adaptive strategies. There was also good psychological support from both the patient’s daughters and nurses, who constantly provided counseling and advice. In terms of habitual recovery, he was able to take care of himself and offered cooperation in rehabilitation programs. Also, results from this analysis benefit the construction of effective tools promoting family participation. Nurses can apply coaching techniques or provide the patient’s relatives with instructional media, such as short video clips and handbooks, to enhance late-phase recovery.
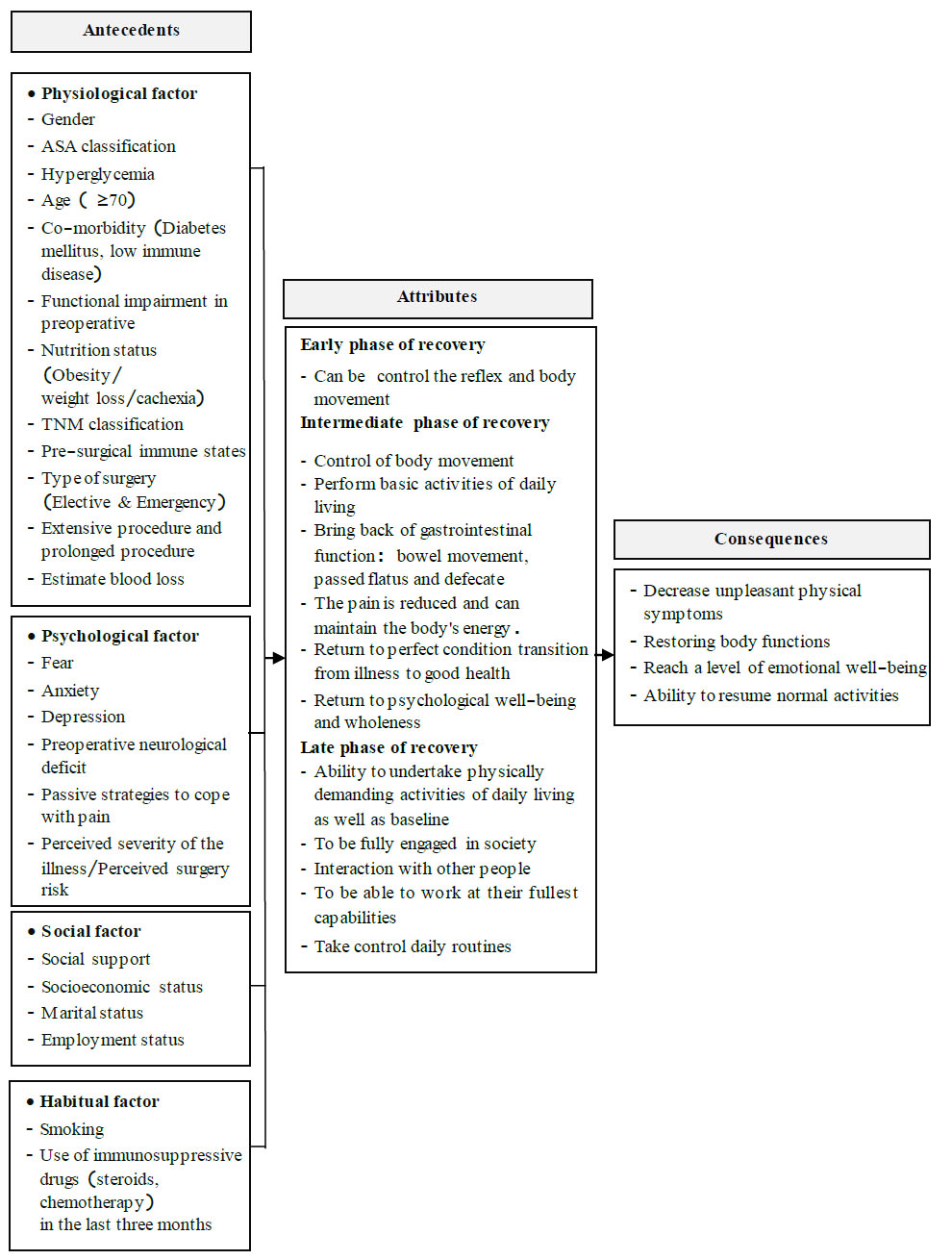
Post-operative recovery after abdominal surgery: antecedents, attributes, and consequences.
4.3.2. Borderline Case
Somsri, a 55-year-old Thai woman, came to the hospital with abdominal pain. She was diagnosed with an abdominal mass and weight loss. An ultrasound revealed a mass in the pancreas, and a surgical plan was made. Postoperatively, the tumor was classified as cancerous. Pain levels were high during the first days but later became much better. The patient was able to do things as normal, interacted with other patients, and was discharged from the hospital on Day 5 after surgery. Radiotherapy and chemotherapy were administered as supplementary treatment. One month after receiving chemotherapy, the patient felt uncomfortable due to nausea, vomiting, fatigue, loss of appetite, and hair loss, all of which interfered with daily life. Additionally, the undesirable symptoms embarrassed the patient and prevented her from returning to work. The patient returned to the hospital seeking consultation. The nurses offered useful advice to reduce chemotherapy effects and find ways to improve her appearance. The patient received positive psychological support from her family members, which built a sense of well-being and self-confidence. Regardless, she was somewhat concerned about other potential symptoms in the next chemotherapy round.
4.3.2.1. Analysis
The above example shows that the patient had a physiological recovery, and body movement could be made without the interference of any discomfort as the pain gradually decreased.
The social interactions were achieved. However, chemotherapy-related physical problems later arose and affected her psychological recovery. Although healthcare professionals had already given advice on how to reduce chemotherapy effects and family members provided constant support for the patient, the anxiety persisted. Since the patient had not experienced chemotherapy before, she became concerned about her illness, which led to psychological problems. Thus, the patient reached a few targets but did not achieve all aspects of recovery.
4.3.3. Related Case
Somjai, a 50-year-old Thai woman undergoing surgery for subtotal gastrectomy with jejunostomy, was treated with NPO and an NG-tube for secretion suction and drainage. She had mild pain but required no analgesia. On day 1 after surgery, she became mobile, starting from Fowler’s position to slowly sitting by the bed and eventually walking around the ward. She could take good care of personal hygiene. The patient always followed the nurses’ instructions. On Day 3, the physician evaluated her bowel function and found bloating, distension, and no flatulence. The patient was also unable to make a fist, so she could not have the NG tube removed, and nurses could not start tube feeding. In her free time, the patient was always reading books and relaxed herself with good music. She liked greeting nurses and talking to her roommates. She was obviously able to adapt and get along with everyone. Talking to roommates who were about to return home encouraged to fight the illness. In addition, she had a strong belief that she would recover and be discharged from the hospital as soon as possible. She planned to take good care of her health and exercise regularly whenever she left the hospital to restore her previous strength and fitness.
4.3.3.1. Analysis
The above example shows that, despite incomplete physical recovery, she applied coping strategies and interacted with others, so she easily accepted her illness. In addition, she had self-esteem, which brought encouragement and strong determination to rehabilitate. Despite her incomplete recovery, the patient expressed positive thinking and optimism in achieving good recovery or a condition relatively close to recovery in all dimensions.
4.3.4. Contrary Case
Suda, a 35-year-old Thai woman, had a motorcycle accident and was knocked unconscious. The doctor found abdominal bleeding, so she was rushed to the operating room for exploratory laparotomy. Spleen tearing and severe uterine rupture were discovered. Hence, the doctor repaired the spleen and performed a hysterectomy. Postoperatively, the patient recovered from anesthesia. Knowing of her complete hysterectomy and inability to conceive, the patient was very sad and stressed, disbelieving what had happened, because she was still young. Her post-operative pain was severe due to large incisions. She kept still, not moving or even changing positions. She did not have the motivation to follow the nurses’ instructions. She did not eat much. The digestive system was considered malfunctioning because the intestines did not work properly, leading to weight loss and muscle weakness with insufficient energy to restore strength and difficulty performing daily routines without nursing assistance. She was completely dependent on others, particularly dayshift nurses, because she had no relatives, and her husband was only there after work. Later, the patient had a high fever due to infected surgical wounds. Her hospital stay was extended because of the infection. Knowing of the longer hospital stay, the patient’s anxiety grew concerning loss of salary and inability to afford the medical fees.
4.3.4.1. Analysis
This situation shows that the patients’ condition clearly failed to cover all components of recovery. Her major surgery had generated severe pain, later resulting in inadequate physical condition, hindering a good recovery. In addition, the patient was still young but had already undergone major surgery and organ removal; thus, she was anxious about her illness affecting her employment. She could not adapt, and her hope of returning to normal life was threatened. Since she had no caregivers to assist her during recovery, self-care was particularly difficult. Psychological problems affected her physiological recovery, which resulted in insufficient physical strength and motivation for rehabilitation.
4.4. Identification of Antecedents and Consequences
Concept analysis in this stage involves identifying antecedents and consequences. Antecedents are events occurring before the concept, whereas consequences are events or incidents caused by the occurrence of the concept [17]. Identifying the antecedents and consequences of a concept provides an understanding of the social contexts in which the concept is used.
4.5. Antecedents
Antecedents are situations or things preceding the concept [17]. Identifying antecedents serves as a guideline for conducting research, developing research instruments, determining nursing practice, and forming nursing theories. According to the literature, the antecedents related to recovery can be classified by group as follows:
4.5.1. Physiological Factors
Physiological factors directly affect recovery and relate to personal factors and physical status preceding surgery and treatment.
4.5.1.1. Age
Patients over 70 years with multiple diseases and ASA scores exceeding 3 points after surgery experience more systemic complications compared to younger patients [18, 19].
4.5.1.2. Gender
Gender influences treatment outcomes. Premeno- pausal women have better body responses to anesthesia than men, but overall recovery is lower than in males. This is believed to be the result of the progesterone hormone [20].
4.5.1.3. Co-morbidity
Co-morbidities are associated with post-operative complications at all ages. According to findings in colorectal surgery patients with colorectal inflammation, the effects of pneumonia and blood clots may be increased [21], which has also been found in colorectal cancer patients with concomitant heart disease and chronic obstructive pulmonary disease as risk factors for post-operative complications [22]. In patients aged 70 years and over, heart disease and lung disease are common, with heart disease having an incidence of 51.1%. This group has significantly increased post-operative colorectal surgery complications [23].
4.5.1.4. Nutrition Status
Malnutrition results in delayed post-operative recovery and return to normal intestinal function [24].
4.5.1.5. Preoperative Physical Activity
Patients with strong preoperative conditions are more likely to have better physical and mental recovery with shorter hospital days [25]. Consistently, those who perform well in low-level preoperative bodily functions are significantly associated with lower post-operative performance on the 6-minute walk test (6MWT) [26].
4.5.1.6. Type of Surgery
Emergency surgery increases the risk of post-operative complications more than elective surgery [27]. In an emergency surgery group, preoperative increases in IL-1β, IL-6, and CRP levels led to lower post-operative survival rates than in the elective surgical group [28].
High blood loss from colorectal surgery (250 ml or more) could be a sign of a longer hospital stay and more complications [29]. Additionally, anemia can generate short-term clinical effects and affect overall survival in the long run [30].
4.6. Psychological Factors
4.6.1. Depressive Symptom
In patients undergoing colorectal cancer surgery, even mild depression can result in decreased ability to perform functions and activities [31].
4.6.2. Anxiety
High and moderate pre- and post-operative anxiety are important factors in reducing post-operative efficacy and immunity in colorectal cancer surgery patients, which affects the wound healing process [32].
4.7. Social Factors
Social Connectedness: People with good social support are comforted, which reduces preoperative anxiety and pain while predicting post-operative recovery [33].
4.8. Habitual Factors
Smoking: Regular smokers can have complications involving the respiratory system and disrupting the wound healing process [34, 35].
4.9. Consequences
Consequences are conditions or events occurring as a result of the proposed concept [17]. The consequences of post-operative recovery in abdominal surgery patients can be grouped into five main categories:1)Decreased unpleasant physical symptoms; 2)Regained functions and re-established activities; 3) A degree of emotional well-being; 4) Independence and return to everyday life; 5) Ability to resume normal activities.
4.9.1. Decreased Unpleasant Physical Symptoms (Pain, Fatigue, Nausea and Vomiting, and Abdominal Discomfort)
There should be no signs of pain or undesirable feelings while the patient is taking oral analgesics or mobilizing.
4.9.2. Regained Functions and Re-established Activities
Improved muscle function, signs of bowel movement (flatulence), and higher tolerance of oral intake (no bloating or pain after consumption); increased lung capacity evidenced by higher activity tolerance.
4.9.3. A Degree of Emotional Well-being
Stress and anxiety are manageable, leading to emotional security and contentment. The patients can adjust themselves, admit physical changes, and fully cooperate in the healing process.
4.9.4. Ability to Resume Normal Activities
Physical performance and capacity are restored. Patients confidently perform the activities of daily living (going to the toilet, getting dressed, taking a shower, and walking upstairs). Patients can practice self-care properly, be confident in accomplishing tasks independently, and return to social engagement.
4.10. Empirical Referents
The way to frame the concepts of abdominal surgery recovery involves setting the measurement of the defined attributes to ensure overall assessment. Many tools are currently being created to evaluate recovery. Most designed tools provide a comprehensive assessment of the features in each dimension of recovery and are well-suited for evaluating different recovery scenarios at different times, depending on the user's choice of tools. The literature revealed that several studies have identified methods for assessing recovery in post-operative patients, including patient interviews, physical performance tests, and recovery instruments. To summarize, the measure- ment approach that corresponds with the characteristics of recovery evaluation is as follows: Physical recovery can be measured by directly talking to patients (tolerance of oral foods, excretion, flatulence and defecation, having no pain at rest while moving and coughing) and physical performance tests (six-minute walk test, incremental shuttle walk test, stair climbing test).Recovery can also be evaluated by using instruments.The Quality of Recovery questionnaire (QoR-40), developed to evaluate the quality of post-operative recovery under general anesthesia, consists of 40 questions divided into five dimensions: emotional state, physical comfort, patient support, physical independence, and pain [34].
Post-operative recovery can be assessed by patient perception, using the current recovery self-assessment, namely the Post-operative Quality of Recovery Score (PQRS) [36, 37], 24-h Functional Ability Questionnaire (24-h FAQ) [38], Post-Discharge Surgical Recovery Scale (PSR) [39], Abdominal Surgery Impact Scale [40], Convalescence and Recovery Evaluation (CARE) [41], and Short-Form 36/RAND-36. [42] These assessments are suitable for evaluating intermediate recovery. Comprehensive 4-dimensional assessment is described as follows: restoration of normal eating, drinking, and hygiene; loss of anxiety, depression, or fatigue; mobili- zation and rehabilitation to full social functioning; and changing from a state of illness to a state of health.
Returning to daily routines, as well as interacting with others, are characteristics of the last phase of recovery. Quality of life is, therefore, assessed to evaluate desirable attributes. The short form 36 (SF-36) is an instrument for the evaluation of surgical outcomes. It consists of 36 items and is divided into 8 aspects: physical (physical functioning, physical role, and bodily pain), psychological (vitality, emotional roles, mental health), and social (social functioning). Each domain is scored on a scale of 0-100, with higher scores representing bodily functions and well-being [42].
5. DISCUSSION
Concept analysis pertaining to the 8-step framework of Walker and Avant enhances understanding of the definitions, attributes, and scopes of the concepts of abdominal surgery recovery. The analysis results revealed that abdominal surgery recovery is the process of returning to physical health and fitness (without post-operative complications), alleviating unpleasant conditions, and becoming mentally healthy and emotionally stable, as seen by appropriate emotional expression, more engagement in social interactions, and independence and confidence about achieving daily routines and activities.Recovery includes significant sub-attributes depending on different phases. At the early stages of recovery, the process is mainly concerned with abilities to control reflexes as well as body movement.For the intermediate phase of recovery, focus is placed on movement capabilities, ability to accomplish basic activities of daily living (ADL), return of gastrointestinal functions, decreased pain, and return to physical fitness and mental health.At the end phase of recovery, the major criteria are as follows: accomplishment of routine tasks, no request for assistance, and fully engaging in social interactions.
CONCLUSION
The insights from concept analysis enhance the construction of the tools used for the inclusive assessment of patient’s abdominal surgery recovery, thereby facilitating relevant research development, and enabling the formulation of nursing theories and nursing practice to promote rapid recovery for target patient groups.
AUTHORS’ CONTRIBUTION
The author confirms sole responsibility for the following study’s conception and design, data collection, analysis and interpretation of results, and manuscript preparation.
LIST OF ABBREVIATIONS
| GI | = Gastro-intestinal |
| QoR-40 | = The Quality of Recovery questionnaire |
| PQRS | = Post-operative Quality of Recovery Score |
| PSR | = Post-Discharge Surgical Recovery Scale |
| CARE | = Convalescence and Recovery Evaluation |
| ADL | = Activities of Daily Living |
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
ACKNOWLEDGEMENTS
The author thanks all credible sources of information for the development of the manuscript and the Royal Thai Air Force Nursing College for additional assistance. My gratitude also goes to my beloved family for moral support.

