All published articles of this journal are available on ScienceDirect.

The Effect of Holy Quran Audio Therapy on Depression and Anxiety Among Jordanian Patients Following CABG: A Randomized Control Trial
Authors Info & Affiliations
Abstract
Background:
The positive outcomes of the CABG procedure are affected by several factors, including the patient’s psychological status, measured by the level of depression and anxiety. The prevalence of depressive symptoms among Jordanian post-CABG patients is high. However, clinicians do not consider anxiety and depression and their impacts in the daily screenings. The effects of non-pharmacological interventions ( i.e. Holy Quran Audio Therapy and Music Therapy) on anxiety and depression have been investigated in some cardiac populations, although no single study was designed specifically to investigate the effect of Holy Quran Audio Therapy on anxiety and depression post-CABG.
Objective:
To examine the effect of Holy Quran audio therapy on anxiety and depression among Arabic-speaking post-CABG patients.
Materials and Methods:
A randomized controlled trial was conducted among 165 post-CABG ICU patients at four major hospitals in (in Amman), (Jordan). They were randomly distributed into control (N = 83) and intervention (N = 82) groups. The intervention group received Holy Quran audio therapy on two days (typically the second and third days after CABG, when patients were alert and not intubated). The therapy session was of ten minutes duration, with four hours in between sessions. Depression and anxiety were measured at baseline and follow-up using the Depression Anxiety Stress Scale. Independent and paired t-tests were used for data analysis.
Results:
Holy Quran audio therapy was linked to statistically significant positive effects. In which Intervention group of patients displaying lower mean depression and anxiety levels compared to the control group (M [SD]; 8.82 [6.35] vs. 13.38 [5.52]) (M [SD]; 6.26 [1.59] vs. 7.48 [3.44], respectively).
Implications for Nursing:
Holy Quran audio therapy is a non-invasively and non-pharmacologically intervention that might be used to decrease depression and anxiety.
Conclusion:
Holy Quran audio therapy significantly improved post-CABG patients’ anxiety and depression and is recommended for Muslim patients to improve their psychological status.
Registration Number:
The clinical trial studies have the registration number NCT 05419554.
1. INTRODUCTION
The most common coronary artery disease (CAD) surgery is coronary artery bypass graft (CABG) [ 1]. Approximately 400,000 CABG surgeries are performed globally each year [ 2], with better survival rates compared to other CAD treatment modalities [ 3]. Furthermore, evidence from a meta-analysis of five clinical trials comprising 4,500 patients revealed that CABG procedures lower the risk of developing new myocardial infarctions and undergoing repeated revascularization procedures [ 4]. Nevertheless, evidence demonstrates that the positive outcomes of the CABG procedure are affected by several factors, including the patient’s psychological status, measured by the level of depression and anxiety (D&A). Anxiety among patients diagnosed with CAD predicts the occurrence of in-hospital complications, including fibrillation, recurrent ischemia, and ventricular tachycardia; indeed, it has even been associated with increased mortality [ 5]. Moreover, the literature revealed similar concerns associated with other heart diseases. For instance, a prospective observational study of 127 patients diagnosed with heart failure showed that persistent anxiety and depression predicted low quality of life [ 6].
In Jordan, the prevalence of depressive symptoms among post-CABG patients ranged from 55% [ 7] to 65.7% [ 8]. Despite these high levels of depression, almost 60% of cardiovascular physicians admitted that they did not screen or only screened less than 25% of their patients for depression [ 9]. This is important because persistent levels of depression are linked to acute myocardial infarction and prolonged length of stay post-CABG [ 7, 10]. Similarly, the impact of depressive symptoms occurring at six months post-CABG on long-term cardiac morbidity was measured at 6-36 months, during which it was found that the increment of depression levels increased the likelihood of developing a variety of morbidities such as adult respiratory distress syndrome, cardiogenic shock, cardiopulmonary arrest, new myocardial infarction, and pulmonary edema [ 11].
It is imperative for nurses to implement appropriate treatment and management for D&A, including both pharmacological and non-pharmacological solutions to improve post-CABG outcomes. Holy Quran audio therapy (QAT) is a non-pharmacological solution used to improve D&A symptoms among patients listening to the original Arabic recitation [ 12-14]. Several studies and clinical trials examined this impact among different patient populations. A randomized controlled trial (RCT) by Maziha et al. [ 15] showed that smokers who recited four chapters of the Quran ( Al-Fatihah, An-Naas, Al-Falaq, and Al-Ikhlas) over four weeks smoked a significantly lower number of cigarettes at week 12 compared to the control group. The same study reported that withdrawal symptoms, such as anxiety, anger, and cravings, were also affected by reciting the Quran. One study even supported the impact of QAT (without translation) on lowering levels of anxiety, depression, and stress among pregnant women in Iran [ 16]. Specific to patients with cardiac conditions, QAT was found to improve sleep quality after cardiac surgeries [ 17], decrease anxiety levels before the cardiac catheterization procedure [ 18], and decrease levels of depression among patients undergoing CABG [ 19]. Although the latter study examined depression after CABG, QAT was integrated with other practices in a comprehensive religious–spiritual program, including prayer and analysis of religious stories.
However, the use of QAT alone on D&A among post-CABG patients has not been explored in Arabic countries. Thus, this RCT seeks to examine the effect of QAT on D&A among Muslim, Arabic-speaking post-CABG patients.
2. MATERIALS AND METHODS
2.1. Design, Sample, and Setting
A Randomized Control Trial was conducted to check the effect of the intervention between the two groups (intervention and control). Consecutive patient samples were included in the study if patients: (1) were adults (aged 18 years old and older); (2) had undergone elective CABG surgery; (3) were hemodynamically stable and able to communicate during interventions and interviews; (hemodynamically stable); (4) were literate in Arabic; (5) were willing to take part in the study and sign their informed consent; (6) were not subject to psychiatric diagnoses of D&A disorders (according to their medical records); (7) were not receiving anti-depression or anti-anxiety medication; and (8) did not have hearing deficiencies.
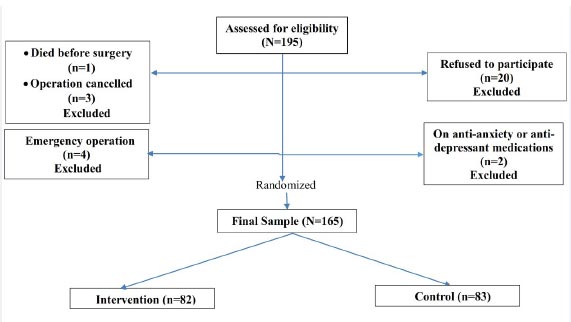
To make sure that the sample size is sufficient to reach the statistical significance, the sample size was calculated using power analysis by G power software 3.1.9.2 with the following assumptions: (1) alpha of 0.05 (2) power of 0.8 (3) medium effect size of 0.5 (4) two-tailed test and (5) paired and independent t-test (as explained). Based on these assumptions, the needed sample size per group for the paired t-test is 34, and for the independent t-test, it is 64 for each group. The 165 participating patients were randomly assigned to control (N = 83) and intervention (N = 82) groups of approximately equal size by a statistician, using tables of random numbers. The study was conducted at four major hospitals (in Amman), (Jordan), including one governmental, one teaching, and two private hospitals (Fig. 1).
2.2. Intervention
The experimental group received QAT for ten minutes over two sessions on two days, one after the other (typically the second and third days following CABG, when patients were stable and not intubated). The daily sessions were four hours apart ( i.e., at 10 am and 2 pm). Surah Al-Rahman was chosen as it is generally regarded as one of the most rhythmic and soothing chapters of the Quran, particularly as rendered by the popular reciter Qari Abdul Basit [ 20]. The listening was undertaken using disposable headphones on an iPad. Conventional ( i.e., biomedical) care was delivered by healthcare professionals to the control group.
2.3. Measurement of Variables
Patients were interviewed, and their medical records were consulted (with appropriate ethical permission) to determine their clinical status (body mass index (BMI) and medical history of acute myocardial infarction, diabetes mellitus, hypertension, left ventricular ejection fraction) and sociodemographic features (age, gender, and marital, smoking, and employment status).
D&A was measured using the Depression Anxiety Subscale of the Depression Anxiety Stress Scale (DASS21), comprising 21 self-reported items measuring D&A severity during one week. DASS21 is a shortened version of DAS S-42 [ 21], with 21 items distributed over three scales (with seven items each): the anxiety (AS), depression (DS), and scale (SS) scales. Only the D&A subscales of DASS21 ( i.e., DS and AS) were used in this study. Participants respond to items using a four-point Likert scale, with responses ranging from “ did not apply to me at all” (0) to “ applied to me very much/ most of the time” (3). All items are added up and doubled to attain equivalence to the DAS S-42 scale, with greater scores indicating greater levels of DAS, as adumbrated below [ 21]:
• Depression: 0-4: Normal, 5-6: Mild, 7-10: Moderate, 11-13: Severe, >13: Extremely severe.
• Anxiety: 0-3: Normal, 4-5: Mild, 6-7: Moderate, 8-9: Severe, >13: Extremely severe.
DASS21 reliability is indicated by its Cronbach’s alpha coefficient values, comprising 0.91 and 0.80 for DS and AS [ 22]. The Arabic DASS21 has Cronbach’s alpha coefficient values of 0.76 and 0.75 for DS and AS [ 23]. In this study, the values were 0.82 for DS and 0.85 for AS.
2.4. Ethical Considerations
This study was approved by the IRB committee at (the Applied Science Private University), (Amman), (Jordan), and by the selected hospitals’ administrative authorities prior to beginning data collection. Moreover, the study was registered as a clinical trial (NCT 05419554). The study was explained in detail to the participants, with assurance of confidentiality, voluntary participation, and the ability to withdraw at any time without any consequences for their healthcare services or statutory rights. Participants who agreed to participate signed an informed consent form, including permission to review their medical records (which was also explained orally). All data were kept in a password-protected computer with appropriate coding.
2.5. Data Collection Process
The co-investigators met with cardiothoracic surgeons and nurse managers of the cardiothoracic surgery clinics at the selected sites and explained the study to them. All patients scheduled for an elective CABG were approached by the co-investigators and were assessed for the eligibility criteria. The study was explained to patients, and if they agreed to participate, they signed an informed consent and were randomly assigned to either an intervention or to a control group.
On the second postoperative day, the co-investigators interviewed the participants and let them answer the sociodemographic questionnaire and the D&A subscales of the DASS-21. The intervention group received the intervention on the same day, as described above. On the third day, the intervention was repeated for the intervention group, while the control group received only regular care (with no QAT or other spiritual care components). On the fourth day, the participants in both groups repeated the D&A subscales of the DASS-21 for comparison purposes. Other required clinical and sociodemographic information (as explained previously) was sourced from patients’ medical records by the co-investigators while the patients were hospitalized.
2.6. Data Analysis
Data were analyzed using SPSS version 25. Descriptive statistics were used to describe the sociodemographic and clinical characteristics of the sample.
To check if the intervention affects D&A, four steps were undertaken.
1. D&A levels were measured for both groups at baseline (before the QAT intervention), and independent samples t-test was applied to avoid bias and ensure no problematic differences between them.
2. The levels of D&A were compared between the two groups after the intervention using independent samples t-test.
3. The levels of D&A were compared between the pre-intervention and post-intervention in the intervention group using the paired t-test.
4. The levels of D&A were compared between the baseline and follow-up measurements for the control group using the paired t-test.
| N (%) or Mean ± SD | |||||
| Characteristics | Total Sample | Intervention (n=82) | Control (n=83) | t or Chi-square | P |
| Age | 69.1 ± 9.6 | 69.7 ± 8.3 | 68.5 ± 10.7 | 0.8 | NS |
| Gender
Male Female |
92 (55.8) 73 (44.2) |
49 (59.8) 33 (40.2) |
43 (51.8) 40 (48.2) |
1.1 | NS |
| Marital status
Married Single/ divorced/ widowed |
106 (64.2) 59 (35.8) |
58(70.7) 24 (29.3) |
48 (57.8) 35 (42.2) |
2.9 | NS |
| History of smoking
Never smoked Current smoker Former smoker |
49 (29.7) 48 (29.1) 68 (41.2) |
19 (23.2) 21 (25.6) 42 (51.2) |
30 (36.1) 27 (32.5) 26 (31.3) |
7.0 | 0.03 |
| History of HTN | 130(78.8) | 70 (85.4) | 60 (72.3) | 4.2 | 0.03 |
| History of DM | 75 (45.6) | 38 (46.3) | 37 (44.6) | 0.08 | NS |
| History of HF | 34 (65.0) | 17(20.7) | 17 (20.5) | 0.002 | NS |
| LVEF | 47.2 ± 8.0 | 47.3 ± 8.5 | 47.1 ± 7.6 | 0.4 | NS |
| BMI, Kg/m 2 | 27.1 ± 4.9 | 27.2 ± 5.5 | 26.9 ± 4.2 | 0.5 | NS |
| Outcome | Group | M±SD | t | Sig (2-tailed) |
|---|---|---|---|---|
| Baseline measurement | ||||
| Depression | Intervention
Control |
12.10±5.68
13.91±6.45 |
-1.89 | NS |
| Anxiety | Intervention
Control |
8.32±1.76
8.22±2.46 |
0.30 | NS |
| Follow-up measurement | ||||
| Depression | Intervention
Control |
8.82±6.35
13.38±5.52 |
-4.93 | <0.001 |
| Anxiety | Intervention
Control |
6.26±1.59
7.48±3.44 |
-2.79 | <0.01 |
| Outcome |
Baseline M±SD |
Follow-up M±SD |
t | Sig (2-tailed) |
|---|---|---|---|---|
| Intervention group | ||||
| Depression | 12.10±5.68 | 8.82±6.35 | 7.92 | <0.001 |
| Anxiety | 8.32±1.76 | 6.26±1.59 | 7.20 | <0.001 |
| Control group | ||||
| Depression | 13.91±6.45 | 13.38±5.52 | 1.44 | NS |
| Anxiety | 8.22±2.46 | 7.48±3.44 | 1.58 | NS |
3. RESULTS
A total of 165 patients (82 in the intervention and 83 in the control group) participated in this trial, with a mean age of 69.1±9.6 years. More than half of the sample (N = 92, 55.8%) were male. Approximately two-thirds were married, and more than three-quarters had a history of hypertension. The intervention group had more patients with a history of hypertension than the control group (85.4% vs. 72.3%) and more former smokers (51.2% vs. 31.3%) (Table 1).
To check if the intervention affected D&A, four steps were undertaken. First, the levels of D&A between the two groups at baseline prior to initiation of the intervention were compared using an independent samples t-test to ensure no differences and avoid bias (Table 2). Second, the levels of D&A were compared between the two groups after the intervention using an independent samples t-test (Table 2). Third, the levels of D&A were compared between the pre-intervention and post-intervention in the intervention group using the paired t-test (Table 3). Fourth, the levels of D&A were compared between the baseline and follow-up measurements for the control group using the paired t-test (Table 3).
4. DISCUSSION
Depression and anxiety are prevalent among patients undergoing cardiac surgery, and these associated conditions affect their cardiac prognosis and are intrinsic forms of mental health issues and low well-being [ 24]. Non-pharmacological interventions are generally recommended for all patients where they do not interfere with biomedical treatment, including psycho-social and spiritual care, a growing and important area of clinical practice worldwide [ 12]. Given the religious background of Jordanian people, it is clearly germane to consider the use of non-pharmacological interventions that include QAT and an intrinsic part of Islamic religious practice. Neurological studies have demonstrated the physiological impacts of this practice, and the QAT has been found to stimulate alpha brain waves that are associated with the release of endorphins, enhancement of the stress threshold, creating a sense of relaxation, and mitigating negative emotions. Therefore, this RCT was implemented to examine the effect of QAT on D&A levels among Jordanian post-CABG patients [ 12].
This was done in a four-step data analysis process. First, the levels of D&A between the intervention and control groups were contrasted before QAT implementation ( i.e., at baseline), and the results revealed that both groups of patients were experiencing high D&A levels, with no significant statistical differences. This was not unexpected since it has been reported that the prevalence of D&A after cardiovascular surgery is higher than that of the general population [ 24].
The second step of the analysis process in the current study compared the levels of D&A between the two groups after the intervention. The results revealed that the levels of D&A were significantly different among the intervention groups. The control group reported higher levels of D&A than the intervention group, indicating a positive impact of QAT on D&A levels. This finding is consistent with a previous study conducted in Iran among 108 patients who underwent cardiac surgery using the same design and intervention [ 25] as well as the general affirmation that non-pharmacological interventions tend to improve cardiovascular surgery patients’ psychological conditions.
Thirdly, the current study's findings revealed that significant differences were reported in the levels of D&A before and after the intervention among the intervention group. This is in line with a systematic review whose results revealed that QAT can function as an effective non-pharmacological solution for anxiety reduction [ 12]. Moreover, this result agreed with an experimental study finding conducted for 70 patients with myocardial infarction who listened to QAT over two days in four daily sessions and revealed that the level of anxiety was significantly lower in the experimental group compared with the control group [ 26].
Moreover, the findings of a semi-experimental study indicated that QAT was effective in reducing anxiety in patients with acute coronary syndrome [ 27]. Previous studies have demonstrated significant impacts of QAT on anxiety, blood pressure, pulse and respiratory rate reduction [ 28]; reducing D&A after open heart surgery (as a complementary therapy) [ 29]; reducing anxiety prior to and following coronary angiography [ 30]; and anxiety reduction following cardiac surgery [ 17], although the latter reported that it did not significantly affect depression.
Among other populations, QAT has been found to positively affect weaning from mechanical ventilation, decreasing anxiety levels among critically ill patients [ 31]. It has also been found to be more effective than no intervention in decreasing depression among hemodialysis patients [ 32] and pregnant women [ 16]. Additionally, another study conducted in Iran concluded that QAT is an easy-to-implement and cost-effective strategy that may be used as a supplemental treatment of depression in hemodialysis patients in resource-challenged contexts [ 33].
While exploring the causation of such effects is beyond the immediate scope of this study, there are known neurological mechanisms that are likely to be instrumental in such impacts. For example, an increase in delta brain waves occurs when reading and listening to the Quran, which stimulates growth hormones responsible for the repair and growth of cells and tissues [ 34]. Additionally, QAT increases alpha waves, directly producing a relaxing effect, and increases attention span [ 35]. Moreover, QAT was found to help improve sleep quality after cardiac surgery, which might positively affect D&A ( i.e., secondary benefits of QAT may include the beneficial impacts of improved sleep quality and duration) [ 17].
The physiological parameters indicating QAT's calming and relaxing effect are related to traditional beliefs about its impact on the human heart, expressed in the production of hormones and chemicals that relax people [ 36, 37]. Such effects are declared in the Quran itself: “Who have believed and whose hearts have rested in the remembrance of Allah. Verily in the remembrance of Allah do hearts find rest!” ( The Meaning of the Glorious Koran 1930, 13:28).
The current study showed that non-significant differences were reported in the levels of D&A between the baseline and follow-up measurements for the control group. Phillip and Baker (2012) reported that between 30% and 40% of CABG patients experience D&A disorders [ 38]. Recent studies reported that the prevalence of depressive symptoms among Jordanian post-CABG patients ranged from 55% [ 7] to 65.7% [ 8]. It is worth noting that D&A levels decreased in the current study's control and intervention groups.
However, D&A levels in the follow-up measures for both groups were still considered moderate to high, which is common in post-CABG patients, as these symptoms are notably persistent [ 39]. Both D&A appear to confer greater morbidity risks, and it is commonly hoped that psycho-social interventions might mitigate the harmful impacts of D&A [ 39]. QAT could be recommended by psychologists for improving mental health and achieving patients’ spiritual needs [ 13].
CONCLUSIONS AND RECOMMENDATIONS FOR FUTURE RESEARCH
The present study revealed that QAT significantly and positively improved D&A among post-CABG patients. Based on the findings of this study, it is particularly recommended that Muslim patients listen to QAT to improve their psychological status following CABG. Researchers can conduct further future studies to compare the effectiveness of reciting and listening to the Quran in combination with other interventions. Moreover, further studies can be conducted to evaluate its impact on different outcomes related to psychological or physiological well-being among Muslims and non-Muslims prior to (as well as following) CABG among Arab populations and those of different ethnicities.
LIST OF ABBREVIATIONS
| AS | = Anxiety Scale |
| BMI | = Body Mass Index |
| CABG | = Coronary Artery Bypass Graft |
| CAD | = Coronary Artery Disease |
| D&A | = Depression and Anxiety |
| DASS21 | = Depression Anxiety Stress Scale |
| DS | = Depression Scale |
| QAT | = Holy Quran Audio Therapy |
| RCT | = Randomized Controlled Trial |
| SS | = Stress Scale |
LIMITATIONS
The intervention of interest in this RCT was restricted to QAT but not other Islamic, spiritual, or non-pharmacological interventions (e.g., prayer, meditation, and spiritual relaxation techniques). Furthermore, this RCT only focused on post-CABG patients’ D&A levels; thus, its findings cannot be used to infer the generalized effects of QAT on physiological indicators or general health.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Institutional Review Board (IRB) approval was obtained from the Faculty of Nursing, Applied Science Private University, Amman, Jordan by the selected hospital administrative authorities.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT TO PARTICIPATE
Each participant signed an informed consent before participating in this study.
STANDARDS OF REPORTING
CONSORT guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
FUNDING
None
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Our sincere appreciation goes to all participants of the present study.

