All published articles of this journal are available on ScienceDirect.

Effectiveness of an Educational Program on Knowledge Change of Nurses Regarding Children with Moderate-to-severe Dehydration under Five Years
Abstract
Introduction:
Dehydration is a major factor in both illness and mortality among children under five years old. The health of children is negatively impacted when nursing care lacks attention to dehydration.
Objectives:
We aimed to examine the effectiveness of a nursing education program on nurses' knowledge regarding the management of moderately to severely dehydrated children under the age of five.
Materials and Methods:
A quasi-experimental study design, which included the request for pre-test and post-test procedures for the experimental and control groups in Kurdistan Region. Using 48 nurses as non-probability purposeful participants, the samples were divided into two groups: the study group, which included 24 nurses, was exposed to an educational program; the control group, which included 24 nurses, was not exposed to the educational program. The information was gathered between March 6, 2022, and June 12, 2022.
Results:
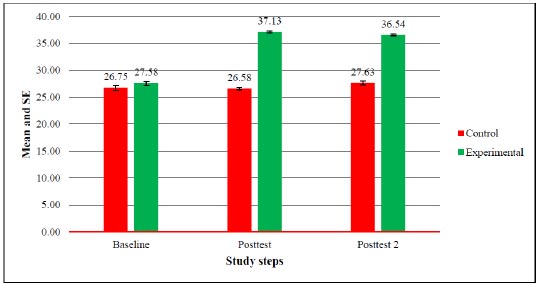
The study findings revealed that the mean scores of nurses' knowledge in the control group were 26.75, 26.58, and 27.63 for the pre-test, post-test 1, and post-test 2, respectively, indicating an inadequate level of knowledge. On the other hand, the mean score of nurses' knowledge in the experimental group was 27.58 during the pre-test. After implementing the educational program, the results showed an improvement, with mean scores of 37.13 and 36.54 for post-tests 1 and 2, respectively. Additionally, a significant number of nurses in the experimental group demonstrated good knowledge levels.
Conclusion:
This study demonstrates that an educational program effectively enhances nurses' knowledge regarding managing dehydration in children.
1. INTRODUCTION
The human body needs water to sustain adequate blood and other fluids to function correctly. Besides, the body needs electrolytes in the blood, other fluids, and cells [1]. Dehydration is a major cause of morbidity and mortality in infants and young children worldwide [2]. The greatest public problem of disease that usually detects in pediatric patients awarded to the emergency department (ED) is dehydration. Initial recognition and involvement are significant in diminishing the hazard of advance to hypovolemic shock and end-organ failure [3].
Dehydration is defined as a condition that happens when an excessive amount of body fluid is lost. In cases where both vomiting and diarrhea are present, gastroenteritis is one of the most prevalent causes of dehydration in children. Dehydration is a physiological disruption brought on by a decrease or imbalance in bodily fluids, which results in hypovolemia. Dehydration is an abnormally negative drop in total body water, sodium, or both due to inadequate consumption of water and sodium [4]. Dehydration can be mild, moderate, severe, or life-threatening. It can impact the proper balance of vital electrolytes, such as sodium and potassium, which are also essential to the healthy functioning of the body [5]. In the United States, there are about 220/000 hospitalizations annually for children under five years of age due to gastroenteritis and dehydration, including 10% of all children requiring hospitalization and 400 deaths per year [6].
Dehydration from illness is a common cause of death in children under five years in developing countries. The health consequences of inadequate water and sanitation services as well as poorer overall health and nutritional status, include an estimated 4 billion cases of diarrhea and mostly among young children in developing countries, and 1.9 million deaths annually (CDC). In infants and children in developing nations, diarrheal illnesses with subsequent dehydration account for nearly 4 million deaths per year. Therefore, numerous extra-related clinical features must be measured, as well as: urine output, sunken eyes, deficiency of tears, dehydrated mucous membranes, heart rate (RR), respiratory rate (RR) and effort, capillary refilling time (RT), skin turgor [7].
The evaluation and management of dehydration proceed addicted to concern the grade of dehydration, repair fluid desires, in addition continuing fluid loss. The processes of dehydration can be largely alienated, interested in (3) groups: enlarged fluid loss, diminished fluid drinking, otherwise together [8]. Management of dehydration is based on its severity or degree of mild dehydration, 50ml per kg of ORS, and for moderate dehydration, 100 mL per kg of ORT solution must be assumed over (4) hrs. in the doctor's office or emergency units [9]. Infusion therapy is one of the most important duties of nurses.
In dealing with intravenous infusion, nurses must know what is well-organized, why it is indicated, its proposed effect on the patients, and any potential side effects that may occur. There for, they should have knowledge which means information gathered from experience and reasoning. They too essential to know the reasoning for intravenous fluid administration and the type of intravenous solution ordered [10]. Generally, the nurse plays a dynamic character given that the carefulness intended for children in any case of situation and causes accessible toward them, as well as documentation of dehydration, clinical features, quantity and sort of fluid nourish to the baby, which are dynamic for pediatric existence [11]. In this regard, we aimed to examine the effectiveness of a nursing education program on nurses' knowledge regarding under-five children with moderate to severe severity.
2. SUBJECTS AND METHODS
2.1. Study Design and Sampling
We applied a quantitative, quasi-experimental study design to evaluate nurses' knowledge concerning children with moderate-to-severe dehydration under five years at two pediatric hospitals. The study was conducted in two main pediatric hospitals, the Duhok and Zakho Cities of the Iraqi Kurdistan Region. The nurses were recruited from two main pediatric hospitals, Heevi Pediatric Teaching Hospital and Bedar General Hospital, from the 3rd of February 2022 till the 12th of June 2022.
The nurses were divided into two experimental and control groups as follows. The experimental group was recruited from nurses who work in the Bedar General Hospital in Zakho City. The control group was recruited from the Pediatric Teaching Hospital in Duhok City. The nurses were followed up before and after the nursing education. The nurses in the experimental group (n=24) received a nursing education about the knowledge of dehydration in children under five years old. The nurses in the control group (n=24) did not receive nursing education.
2.2. Procedure
A purposive probability participant of 48 nurses who were employed in pediatric hospitals and met the sample criteria was included in this study. The samples were separated into two groups; the first group comprised 24 nurses in the experimental group who were exposed to the educational program. But the second group of 24 nurses in the control group were not exposed to the involvement of the educational program. Every set had nearby similar features as probable. The groups were recruited from two independent hospitals to avoid allocation bias.
2.3. Outcome Measurements
The level of knowledge about dehydration among children under five years was assessed before and after the completion of education. In order to assess the effectiveness of the health education program earlier and after the running of the instructive program, knowledge instruments were structured to assess the nurse's knowledge. It consists of 2 parts: - Part One: demographic characteristics: This linked to the sample demographical characteristics, which included age, gender, educational level, marital status, years of experience, unit of work, participation in a training course regarding dehydration, and residential area. Related to nurses' knowledge about dehydration management which included 20 items of multiple choice questions, each item had two alternatives. Each item in the knowledge questionnaire was scored as an incorrect or correct answer. Each nurse received one score for each correct answer and zero for an incorrect answer. The total scores given to each nurse were added together, and obtained the knowledge score.
2.4. Statistical Analyses
The general characteristics of nurses were presented as numbers and percentages. The comparisons of demographic characteristics between control and experimental nurse groups were examined using Pearson chi-square tests. Moreover, the comparisons of knowledge frequencies between control and experimental nurse groups at baseline were examined using Pearson chi-square tests. The comparisons of knowledge scores between control and experimental nurse groups at different times were examined using an independent t-test. The comparisons of knowledge scores between study steps in control and experimental nurse groups at different times were examined using Bonferroni correction. The associations of knowledge scores with demographic characteristics in the experimental groups at the second follow-up were examined using an independent t-test or ANOVA one-way. The pairwise comparisons were examined using a Tukey test. The significant level of difference was determined at a p-value <0.05. The statistical calculations were performed by JMP Pro 14.3.0 (https://www.jmp.com/en_us/home.html).
3. RESULTS
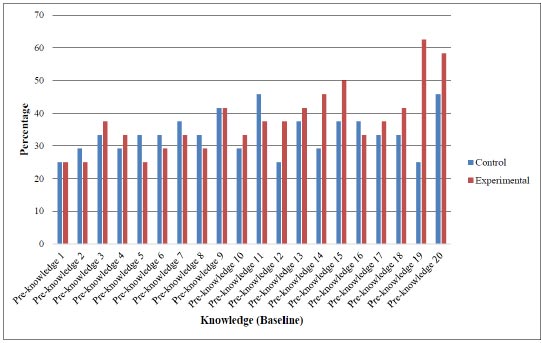
The study found that the control and experimental nurses are similar in age group (P=0.9325), gender (P=0.7679), education (P+0.7537), and other socio-demographic characteristics, including marital status, working units, experience in nursing, training courses, and residency (Table 1). The study showed that the control and experimental nurses were similar in correct and incorrect answers for all knowledge items except for item 19. A higher percentage of nurses in the experimental group had correct answers towards tem 19 than those in the control group (62.5% vs. 25.0; P=0.0189). In addition, the control and experimental nurses had a similar knowledge score at baseline; 26.75 vs. 27.58 (P=0.1561; Table 2 and Fig. 1).
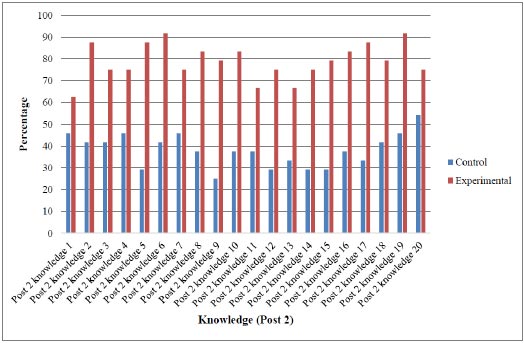
The study showed that the nurses in the experimental group had a higher percentage of correct answers compared to the nurses in the control group, except for item 20. In addition, the nurses in the experimental groups had significantly higher knowledge scores than the nurses in the control group, 37.13 vs. 26.58 (P<0.0001; Table 3 and Fig. 2). A similar pattern as the post-test was found at the second follow-up time expected for items 1 and 20. The nurses in the experimental group had a significantly higher percentage of correct answers compared to the nurses in the control group. In addition, the nurses in the experimental group had a significantly higher knowledge score than those in the control group at the second follow-up time, 36.54 vs. 27.63 (P<0.0001; Table 4 and Fig. 3).
| Demographic Characteristics | Study Groups No (%) | p-value (two-sided) | |
|---|---|---|---|
| Control (n=24) | Experimental (n=24) | ||
|
Age groups < 25 years 26-32 years 33-40 years |
2 (8.33) 17 (70.83) 5 (20.83) |
2 (8.33) 18 (75.00) 4 (16.67) |
0.9325 |
|
Gender Male Female |
14 (58.33) 10 (41.67) |
15 (62.50 9 (37.50 |
0.7679 |
|
Education Secondary Institute College |
3 (12.50) 16 (66.67) 5 (20.83) |
2 (8.33) 15 (62.50) 7 (29.17) |
0.7537 |
|
Marital status Single Married |
9 (37.50) 15 (62.50) |
8 (33.33 16 (66.67 |
0.7628 |
|
Experience < 5 years > 15 years 11-15 years 5-10 years |
3 (12.50) 2 (8.33) 2 (8.33) 17 (70.83) |
2 (8.33) 2 (8.33) 1 (4.17) 19 (79.17) |
0.8862 |
|
Working unit Medical ward NICU PICU Surgical ward |
16 (66.67) 3 (12.50) 3 (12.50) 2 (8.33) |
17 (70.83) 3 (12.50) 2 (8.33) 2 (8.33) |
0.9726 |
|
Training course No Yes |
3 (12.50) 21 (87.50) |
2 (8.33) 22 (91.67) |
1.0000 |
|
Residency Rural Suburban Urban |
5 (20.83) 2 (8.33) 17 (70.83) |
5 (20.83) 4 (16.67) 15 (62.50) |
0.6731 |
| Knowledge Items | Study Groups | p-value (two-sided) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Control | Experimental | ||||||||
| - | Incorrect Answer | Correct Answer | Incorrect Answer | Correct Answer | - | ||||
| - | no | % | no | % | no | % | no | % | - |
| Pre-knowledge 1 | 18 | 75.00 | 6 | 25.00 | 18 | 75.00 | 6 | 25.00 | 1.000 |
| Pre-knowledge 2 | 17 | 70.83 | 7 | 29.17 | 18 | 75.00 | 6 | 25.00 | 0.7543 |
| Pre-knowledge 3 | 16 | 66.67 | 8 | 33.33 | 15 | 62.50 | 9 | 37.50 | 0.7628 |
| Pre-knowledge 4 | 17 | 70.83 | 7 | 29.17 | 16 | 66.67 | 8 | 33.33 | 0.7555 |
| Pre-knowledge 5 | 16 | 66.67 | 8 | 33.33 | 18 | 75.00 | 6 | 25.00 | 0.5254 |
| Pre-knowledge 6 | 16 | 66.67 | 8 | 33.33 | 17 | 70.83 | 7 | 29.17 | 0.7555 |
| Pre-knowledge 7 | 15 | 62.50 | 9 | 37.50 | 16 | 66.67 | 8 | 33.33 | 0.7628 |
| Pre-knowledge 8 | 16 | 66.67 | 8 | 33.33 | 17 | 70.83 | 7 | 29.17 | 0.7555 |
| Pre-knowledge 9 | 14 | 58.33 | 10 | 41.67 | 14 | 58.33 | 10 | 41.67 | 1.000 |
| Pre-knowledge 10 | 17 | 70.83 | 7 | 29.17 | 16 | 66.67 | 8 | 33.33 | 0.7555 |
| Pre-knowledge 11 | 13 | 54.17 | 11 | 45.83 | 15 | 62.50 | 9 | 37.50 | 0.5582 |
| Pre-knowledge 12 | 18 | 75.00 | 6 | 25.00 | 15 | 62.50 | 9 | 37.50 | 0.3502 |
| Pre-knowledge 13 | 15 | 62.50 | 9 | 37.50 | 14 | 58.33 | 10 | 41.67 | 0.7679 |
| Pre-knowledge 14 | 17 | 70.83 | 7 | 29.17 | 13 | 54.17 | 11 | 45.83 | 0.2330 |
| Pre-knowledge 15 | 15 | 62.50 | 9 | 37.50 | 12 | 50.00 | 12 | 50.00 | 0.3827 |
| Pre-knowledge 16 | 15 | 62.50 | 9 | 37.50 | 16 | 66.67 | 8 | 33.33 | 0.7628 |
| Pre-knowledge 17 | 16 | 66.67 | 8 | 33.33 | 15 | 62.50 | 9 | 37.50 | 0.7628 |
| Pre-knowledge 18 | 16 | 66.67 | 8 | 33.33 | 14 | 58.33 | 10 | 41.67 | 0.5510 |
| Pre-knowledge 19 | 18 | 75.00 | 6 | 25.00 | 9 | 37.50 | 15 | 62.50 | 0.0189 |
| Pre-knowledge 20 | 13 | 54.17 | 11 | 45.83 | 10 | 41.67 | 14 | 58.33 | 0.3861 |
| Pre-knowledge score | Mean | 26.75 | SD | 2.27 | Mean | 27.58 | SD | 1.69 | 0.1561* |
The red bold numbers show significant differences.

| Knowledge and Practice | Study Groups | p-value (two-sided) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Control | Experimental | ||||||||
| - | Incorrect Answer | Correct Answer | Incorrect Answer | Correct Answer | - | ||||
| - | no | % | no | % | no | % | no | % | - |
| Post-knowledge 1 | 18 | 75.00 | 6 | 25.00 | 4 | 16.67 | 20 | 83.33 | <0.0001 |
| Post-knowledge 2 | 17 | 70.83 | 7 | 29.17 | 4 | 16.67 | 20 | 83.33 | 0.0002 |
| Post-knowledge 3 | 16 | 66.67 | 8 | 33.33 | 4 | 16.67 | 20 | 83.33 | 0.0004 |
| Post-knowledge 4 | 16 | 66.67 | 8 | 33.33 | 3 | 12.50 | 21 | 87.50 | 0.0001 |
| Post-knowledge 5 | 16 | 66.67 | 8 | 33.33 | 2 | 8.33 | 22 | 91.67 | <0.0001 |
| Post-knowledge 6 | 15 | 62.50 | 9 | 37.50 | 6 | 25.00 | 18 | 75.00 | 0.0088 |
| Post-knowledge 7 | 14 | 58.33 | 10 | 41.67 | 4 | 16.67 | 20 | 83.33 | 0.0065 |
| Post-knowledge 8 | 16 | 66.67 | 8 | 33.33 | 4 | 16.67 | 20 | 83.33 | 0.0010 |
| Post-knowledge 9 | 15 | 62.50 | 9 | 37.50 | 5 | 20.83 | 19 | 79.17 | 0.0077 |
| Post-knowledge 10 | 17 | 70.83 | 7 | 29.17 | 5 | 20.83 | 19 | 79.17 | 0.0005 |
| Post-knowledge 11 | 12 | 50.00 | 12 | 50.00 | 4 | 16.67 | 20 | 83.33 | 0.0305 |
| Post-knowledge 12 | 15 | 62.50 | 9 | 37.50 | 4 | 16.67 | 20 | 83.33 | 0.0027 |
| Post-knowledge 13 | 14 | 58.33 | 10 | 41.67 | 4 | 16.67 | 20 | 83.33 | 0.0065 |
| Post-knowledge 14 | 16 | 66.67 | 8 | 33.33 | 3 | 12.50 | 21 | 87.50 | 0.0003 |
| Post-knowledge 15 | 15 | 62.50 | 9 | 37.50 | 3 | 12.50 | 21 | 87.50 | 0.0008 |
| Post-knowledge 16 | 17 | 70.83 | 7 | 29.17 | 5 | 20.83 | 19 | 79.17 | 0.0012 |
| Post-knowledge 17 | 17 | 70.83 | 7 | 29.17 | 6 | 25.00 | 18 | 75.00 | 0.0015 |
| Post-knowledge 18 | 16 | 66.67 | 8 | 33.33 | 5 | 20.83 | 19 | 79.17 | 0.0032 |
| Post-knowledge 19 | 14 | 58.33 | 10 | 41.67 | 3 | 12.50 | 21 | 87.50 | 0.0020 |
| Post-knowledge 20 | 11 | 45.83 | 13 | 54.17 | 5 | 20.83 | 19 | 79.17 | 0.1246 |
| Post-knowledge score | Mean | 26.58 | SD | 1.06 | Mean | 37.13 | SD | 0.90 | <0.0001* |
Pearson chi-square test was performed for others.
The red numbers show significant differences.
| Knowledge and Practice | Study Groups | p-value (two-sided) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Control | Experimental | ||||||||
| - | Incorrect Answer | Correct Answer | Incorrect Answer | Correct Answer | - | ||||
| - | no | % | no | % | no | % | no | % | - |
| Post 2 knowledge 1 | 13 | 54.17 | 11 | 45.83 | 9 | 37.50 | 15 | 62.50 | 0.2466 |
| Post 2 knowledge 2 | 14 | 58.33 | 10 | 41.67 | 3 | 12.50 | 21 | 87.50 | 0.0020 |
| Post 2 knowledge 3 | 14 | 58.33 | 10 | 41.67 | 6 | 25.00 | 18 | 75.00 | 0.0192 |
| Post 2 knowledge 4 | 13 | 54.17 | 11 | 45.83 | 6 | 25.00 | 18 | 75.00 | 0.0388 |
| Post 2 knowledge 5 | 17 | 70.83 | 7 | 29.17 | 3 | 12.50 | 21 | 87.50 | <0.0001 |
| Post 2 knowledge 6 | 14 | 58.33 | 10 | 41.67 | 2 | 8.33 | 22 | 91.67 | 0.0005 |
| Post 2 knowledge 7 | 13 | 54.17 | 11 | 45.83 | 6 | 25.00 | 18 | 75.00 | 0.0388 |
| Post 2 knowledge 8 | 15 | 62.50 | 9 | 37.50 | 4 | 16.67 | 20 | 83.33 | 0.0027 |
| Post 2 knowledge 9 | 18 | 75.00 | 6 | 25.00 | 5 | 20.83 | 19 | 79.17 | 0.0004 |
| Post 2 knowledge 10 | 15 | 62.50 | 9 | 37.50 | 4 | 16.67 | 20 | 83.33 | 0.0027 |
| Post 2 knowledge 11 | 15 | 62.50 | 9 | 37.50 | 8 | 33.33 | 16 | 66.67 | 0.0431 |
| Post 2 knowledge 12 | 17 | 70.83 | 7 | 29.17 | 6 | 25.00 | 18 | 75.00 | 0.0015 |
| Post 2 knowledge 13 | 16 | 66.67 | 8 | 33.33 | 8 | 33.33 | 16 | 66.67 | 0.0209 |
| Post 2 knowledge 14 | 17 | 70.83 | 7 | 29.17 | 6 | 25.00 | 18 | 75.00 | 0.0015 |
| Post 2 knowledge 15 | 17 | 70.83 | 7 | 29.17 | 5 | 20.83 | 19 | 79.17 | 0.0012 |
| Post 2 knowledge 16 | 15 | 62.50 | 9 | 37.50 | 4 | 16.67 | 20 | 83.33 | 0.0027 |
| Post 2 knowledge 17 | 16 | 66.67 | 8 | 33.33 | 3 | 12.50 | 21 | 87.50 | 0.0003 |
| Post 2 knowledge 18 | 14 | 58.33 | 10 | 41.67 | 5 | 20.83 | 19 | 79.17 | 0.0171 |
| Post 2 knowledge 19 | 13 | 54.17 | 11 | 45.83 | 2 | 8.33 | 22 | 91.67 | 0.0013 |
| Post 2 knowledge 20 | 11 | 45.83 | 13 | 54.17 | 6 | 25.00 | 18 | 75.00 | 0.1313 |
| Post 2 knowledge score | Mean | 27.63 | SD | 1.71 | Mean | 36.54 | SD | 0.78 | <0.0001* |
Pearson chi-square test was performed for others.
The red numbers show significant differences.
| Control | Post-test vs. Pre-test | Post-test 2 vs. Pre-test | Post-test 2 vs. Post-test |
|---|---|---|---|
|
Knowledge Score Mean vs. mean (p-value) Mean diff (95% CI) |
26.58 vs. 26.75 (p=0.6218) -0.17 (-0.86 to 0.52) |
27.63 vs. 26.75 (p=0.1119) 0.88 (-0.22 to 1.97) |
27.63 vs. 26.58 (p=0.0023) 1.04 (0.41 to 1.67) |
| Experimental | Post-test vs. Pre-test | Post-test 2 vs. Pre-test | Post-test 2 vs. Post-test |
|
Knowledge Score Mean vs. mean (p-value) Mean diff (95% CI) |
37.13 vs. 27.58 (p<0.0001) 9.54 (8.79 to 10.29) |
36.54 vs. 27.58 (p<0.0001) 8.96 (8.15 to 9.77) |
36.54 vs. 37.13 (p=0.0161) -0.58 (-1.05 to -0.12) |
The red numbers show significant differences.
The study showed that the level of knowledge score significantly increased from the post-test to the second follow-up in the control group, 27.63 vs. 26.58 (p=0.0023). However, the knowledge level was significantly increased from baseline to post-test and post-test 2 in the experimental groups (Table 5 and Fig. 4). The study showed that the higher level of knowledge score in the experimental group is related to education, marital status, and experience in nursing. The nurses with a secondary level of education had a significantly higher knowledge score compared to those nurses with a college degree (37.50 vs. 36.0; P=0.0249). In addition, nurses with less than 5 years of experience in nursing had a higher knowledge score compared to nurses with 5-10 years of experience (P=0.0195). Moreover, the single nurses had a higher knowledge score compared to the married nurses (36.88 vs. 36.00; P=0.0017; Table 6).
4. DISCUSSION
4.1. Discussion of the Comparison Between Nurses' Knowledge of the Experimental and Control Groups Regarding Pre-test, Post-test 1, and Post-test 2
The average knowledge score of the nurses was 26.75 (pre-test), 26.58 (post-test 1), and 27.63 (post-test 2) among the control group, with no significant differences. In a study [12], the majority of nurses' knowledge was discovered to be inadequate in test one (84.9%) and test two (79.2%) in the control group. Another study [13] found 88% of nurses had limited knowledge of intravenous fluid therapy for dehydrated infants under five years. Similar to what Mahmoud [14] discovered in their study—that approximately 40% of nurses had inadequate knowledge. However, Qamar, Afzal [15] disagreed with Alrubaiee, Baharom [16] and found in their study conducted in Pakistan that 87% of nurses in public hospitals had a good awareness of IV cannula protocols. There are no programs for ongoing education, and most nurses graduated from an institute.
The nurses in the experimental group had higher knowledge scores than the control group (37.13 and 36.54 in the post-tests 1 and 2, respectively). This showed that nurses' knowledge of how to treat dehydration in young infants was significantly improved. This study's findings are supported by Imazu, Faria [17], who discovered that there was an improvement in knowledge about the disease in the interventional group. Similarly, Maria, Kaur [18] compared video-assisted teaching versus self-instructional modules for the care of ventilated patients on staff nurses'. They found that the mean of nurses' knowledge and practice in the pre-test were increased in the post-test. Similar effects were found by AlReshidi [19] as well.
| Demographic Characteristics | Frequency Distribution | p-value (two-sided) | Pairwise Comparisons | |
|---|---|---|---|---|
| Mean | Std Dev | |||
|
Knowledge score < 25 years 26-32 years 33-40 years |
37.00 36.44 36.75 |
1.41 0.70 0.96 |
0.5538 | - |
|
Gender Male Female |
36.6 36.44 |
0.74 0.88 |
0.6462 | - |
|
Education Secondary Institute College |
37.50 36.53 36.00 |
0.71 0.74 0.00 |
0.0288 | Secondary vs. College (p=0.0249) Secondary vs. Institute (p=0.1378) Institute vs. College (p=0.2222) |
|
Marital status Single Married |
36.88 36.00 |
0.83 0.00 |
0.0017 | - |
|
Experience < 5 years > 15 years 5-10 years |
37.00 36.50 36.00 |
1.41 0.71 0.00 |
0.0171 | < 5 years vs. 5-10 years (p=0.0195) < 5 years vs. > 15 years (p=0.4819) > 15 years vs. 5-10 years (p=0.2955) |
|
Working unit Medical ward NICU PICU Surgical ward |
36.59 36.67 36.50 36.00 |
0.80 1.15 0.71 0.00 |
0.7979 | - |
|
Training course No Yes |
37.00 36.50 |
1.41 0.74 |
0.3968 | - |
|
Residency Rural Suburban Urban |
37.00 36.25 36.47 |
1.00 0.50 0.74 |
0.3095 | - |
The pairwise comparisons were examined using a Tukey test.
The red numbers show significant differences.
4.2. Discussion of the Effectiveness of an Educational Program on Nurses' Knowledge of Experimental and Control Groups
The study showed that the experimental group in post-tests 1 and 2 had a higher mean score compared to the control group. Also, there were very significant differences in the experimental group's nurses' knowledge compared to pre, post-test1, and post-test2. These analyses supported the findings of studies by Aslam, Afzal [20], and Abd Elalem and Fouad [21], which found that nurses lacked sufficient knowledge about administering fluids and electrolytes, which had an impact on patient care. These studies suggested that special education programs would raise nurses' recognition and knowledge regarding body fluid balance assessment. Asfour [22] reported that more than a third of nurses lacked information about measuring fluid input and output. Furthermore, the current finding was supported by Sanders [23], who revealed that the majority of nurses knew that children with severe dehydration (Plan C) are resuscitated using intravenous fluids, which generally necessitates the kid to be transported to an inpatient ward. Our findings were also consistent with a study done by Abd El-SalamSheta and Mahmoud [24], who discovered that the overall nurse's knowledge and practice score regarding body fluid balance assessment increased from 6% to 86.7% after the teaching program. Similar to how this study's findings strongly concur with those of Al-Mussawi, Sajjad S. Issa [25], who examined how an educational program affected students at a nursing college's knowledge of intravenous therapy in Basra, Iraq. Their study discovered that students' knowledge had improved and that there was a highly significant correlation between nurses' knowledge on the pre-test and post-test.
This study showed that nurses with fewer than five years of experience scored higher on knowledge tests than nurses with five to ten years of experience. Similar results were reported by Orrisa as well [26]. They discovered that nurses with less than one year of professional experience (38.6%) had enough knowledge about intravenous therapy than those with more than two years of experience (29.4%). However, the findings indicated no correlation between working units and nurses' knowledge in the experimental group. The findings of a recent study [27] in Kenya did not support the findings of this study. They found that respondents in surgical wards had higher average knowledge scores on IV fluid therapy than their medical ward peers. Likewise, the majority of the participants did not attend any training courses, and the results showed no differences between the knowledge of nurses and the training course for either group. This finding disagreed with a study [24] that examined the effect of a structured educational program on nurses' knowledge and expertise concerning the assessment of body fluid balance for critically ill patients in the intensive care unit in Egypt. Additionally, a study [28] contradicted this conclusion by reporting that less than a quarter of nurses did not attend a training session. Nurses can stay up to date on current procedures and take advantage of possibilities for improvement by taking part in training programs and courses that are offered as part of continuing nursing education.
5. RECOMMENDATIONS
We recommend that the first step should involve examining the issues nurses face in managing diarrhea in children. This could be done by identifying the challenges they encounter, the mistakes that are commonly made, and areas for improvement in their practice. Based on these needs, the second step would involve designing and presenting an educational program that specifically addresses the identified areas of concern for the nurses.
CONCLUSION
This study showed that an educational program is an effective technique to increase the level of knowledge among nurses about the management of children with dehydration.
LIST OF ABBREVIATIONS
| ED | = Emergency department |
| RT | = Refilling time |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study is approved by the ethical committee of the Directorate of Planning Scientific Research Division. Approval # 18082021-8-1.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information is available within the article.
ACKNOWLEDGEMENTS
Declared none.

