All published articles of this journal are available on ScienceDirect.

Evaluation of the Quality of Clinical Education and the Clinical Self-efficacy of Nursing Students during the COVID-19 Pandemic
Authors Info & Affiliations
Abstract
Background:
Clinical education is the most important part of the education of nursing, operating room, and anesthesia students. During the COVID-19 pandemic and the suspension of clinical training, these students became very concerned. Nursing schools also limit clinical education to create a balance between students' educational needs and safety. Therefore, the present study aimed to investigate the effect of changing clinical education conditions during the COVID-19 pandemic on the quality of clinical education and the clinical self-efficacy of nursing, operating room, and anesthesia students in Tehran, Iran.
Methods:
This descriptive cross-sectional study was conducted in 2020 on 277 seventh and eighth-semester nursing, operating room, and anesthesia students in Tehran, Iran. Students were selected by simple random sampling using a random number table. The study tools included the demographic questionnaire, the clinical education quality questionnaire, and the clinical self-efficacy questionnaire, which were sent to the participants via WhatsApp and Telegram after confirming their validity and reliability.
Results and Discussion:
64.30% of students were female, and the mean age was 23.59±3.49. The mean of total scores for the quality of clinical education and clinical self-efficacy was equal to 57.38±12.43 and 104.88±23.01, respectively. 57% of students considered moderate the level of the quality of clinical education and 51.60% of them moderate the level of clinical self-efficacy. The total score for clinical self-efficacy significantly correlated with the quality of clinical education (r=0.12, P-value=0.04).
Conclusion:
The use of new educational methods, planning the course based on the needs of learners and in accordance with the conditions, and increasing the capability and the clinical self-efficacy of nursing students should be considered by nursing professors.
1. INTRODUCTION
The outbreak of COVID-19, followed by a forced shutdown of the world to prevent the transmission of the SARS-CoV-2 virus, severely disrupted the world education system [1]. As health care systems prepared to treat a large number of infected patients, the health education system faced the problem of creating a balance between the educational needs and the safety of students so that nursing schools suspended or limited face-to-face theatrical education and clinical training [2]. Despite the challenges related to the COVID-19 pandemic, the education system was helping to develop the next generation of care providers [3].
As nursing students spend their internships in medical centers, they are one of the groups that experienced the most problems during the COVID-19 pandemic. One of the most important challenges of e-learning during the outbreak of Coronavirus disease was the many problems that nursing schools faced in the field of practical and clinical education of students, causing many concerns [4].
Before the COVID-19 pandemic, most of the training of nursing students was carried out in hospitals and at the patient's bedside. At the beginning of the epidemic, nursing students, intensive care nursing students, and operating room nursing students suffered a lot of stress due to the rapid spread of the disease as well as the resulting deaths [5, 6].
Due to the clinical nature of such fields as nursing, operating room, and anesthesia, the students in these fields should study them through an internship in a clinical setting instead of a classroom. Under direct or indirect supervision, the students should be able to implement nursing procedures practically that have been learned during the theoretical courses [4].
Operating room (OR) nurses participate in surgery teams with healthcare professionals such as surgeons, residents, anesthesiologists, anesthesia nurses, and radiologists. OR nurses must perform the tasks quickly and accurately by collaborating with healthcare professionals and exerting various competencies such as communication ability, leadership, and surgical knowledge and technology. OR nurses' perioperative competency is essential for coping with clinical situations, job involvement, job continuity, efficient operation management, and patient safety [7].
Anesthesia training programs' needs changed in the era of coronavirus (COVID-19). Mandatory social isolation precipitated in response to the viral pandemic radically altered the dynamics of anesthesia education. As the pandemic altered the options for all traditional educational forums, online distance teaching assumed a major role in substituting for former in-person learning [8]. The COVID-19 pandemic deprived students of the opportunity for clinical education and changed the way they were taught, the quality of clinical education was challenged around the world and many countries tried to use new online education tools to provide clinical training for students [9]. Given that clinical education is the most important part of nursing students' education [10], theoretical knowledge alone is not enough to provide safe care [10, 11]. During the dynamic process of clinical education, students gain experiences by being present at the patient's bedside and putting into practice the concepts learned while interacting with the educators and the environment [11]. Problems in clinical education have adverse effects on achieving the goals of nursing education. Thus, more attention and effort are needed to identify challenges and solve the problems [9].
Previous studies have reported that nursing students are afraid of increased risks in the clinical setting during a pandemic [12].
The results of a study conducted during the COVID-19 pandemic showed that 65.9% of students in the hospital environment suffered from anxiety due to fear of being infected with the Coronavirus and transmitting the disease to their family members [13]. On the other hand, changes in educational conditions and interruptions in internships can also cause anxiety in them [3]. Fear and anxiety negatively affect educational performance as well as clinical performance [12]. Effective education leads to a sense of self-esteem and clinical self-efficacy in nursing students [14]. In nursing education, self-efficacy can be used to measure how the nurses' clinical skills are reliable [15]. Nursing students are affected by the environment and an inappropriate educational environment can have detrimental consequences on their clinical self-efficacy [15]. Lack of attention to promoting self-efficacy in clinical settings lead undoubtedly to the reduced quality of the performance of the workforce trained for nursing [16].
A review of studies shows that the effect of changing educational conditions during the COVID-19 pandemic on the quality of clinical education and clinical self-efficacy of nursing students should be examined [3, 17] because they were anxious that the educational goals set for them would not be achieved and they would not acquire the necessary skills during the COVID-19 pandemic [3].
Furthermore, nursing competency differs depending on clinical experience and the competency may differ even with similar experiences. In other words, the level of competency may vary depending on the level of experience and education [7].
Continuous evaluation of the quality of education is of special importance for educational programs so the study of the current conditions seems necessary to improve the quality of clinical education of students by improving and updating educational programs [3]. Most studies on the quality of clinical education of nursing students have been conducted before the COVID-19 pandemic and the studies have recognized that the quality of clinical education is moderate or unfavorable [11, 18-22]. Additionally, studies on the clinical education of nurses indicate less attention to the clinical self-efficacy of students. Lack of attention to promoting self-efficacy in clinical settings undoubtedly reduces the quality of the performance of nurses [10, 11].
Analyzing nursing competency, assessing the need for additional education that changes based on career stage and improves professionalism, and providing different education according to the clinical ladder is very important for building capacity [7].
Therefore, considering the importance and the challenges of clinical education for nursing, operating room, and anesthesia students during the COVID-19 pandemic, the present study aimed to identify the strengths and weaknesses of this group of students to determine the quality of clinical education from the students' points of view and assess their clinical self-efficacy during the pandemic.
2. MATERIALS AND METHODS
2.1. Study Design
This cross-sectional study was performed in the faculty of Nursing and Midwifery of the Shahid Beheshti University of Tehran in 2021. The study population included seventh and eighth-semester nursing, operating room, and anesthesia students.
2.2. Samples
The simple random sampling technique was used in this study. Accordingly, a list of characteristics of students was provided and students were selected and included in the study based on a random number table. Inclusion criteria included being 7th and 8th-semester students, having smartphones and having no work experience in the COVID-19 wards. Exclusion criteria included not completing the questionnaires fully and unwillingness to continue participation in the study. The online version of the questionnaires was provided and then sent to participants through messaging apps such as WhatsApp or Telegram. The sample size was determined based on the study conducted by Mehrabi et al. [23]. Therefore, the standard deviation (SD) of 21.19, precision (d) of 2.5, and a type 1 error of 5% were placed in the following formula. Finally, out of 360 students studying in the fourth year, 277 students participated in the study:
2.3. Data Collection Tools
The questionnaires used in this study were the demographic questionnaire, the clinical education quality questionnaire, and the clinical self-efficacy questionnaire.
2.3.1. Demographic Characteristics
Demographic questionnaire included the following five questions: age, gender, semester, the field of study, and employment status at the time of the study (simultaneity of employment and education).
2.3.2. Clinical Education Quality
The tool used to assess the quality of clinical education among students was the clinical education quality questionnaire. It was designed based on the various studies and the professors' experiences in clinical teaching for the students of Iranian universities and the content validity and Cronbach's alpha were used to assess its validity and reliability. In several studies, Cronbach's alpha for this questionnaire was obtained to be 0.91, 0.88, and 0.85 [11, 18, 19]. This questionnaire contains 33 items and five indicators as follows: educational goals and curriculum (11 items), educators' performance (9 items), the way of communication between the educators and students (4 items), educational environment (5 items), and supervision and evaluation (4 items). The answers are scored based on a nominal scale, including yes (score=3), to some extent (score=2), and no (score=1). The total score ranges from 33 to 99, which is classified into three levels (score 33-53 (weak), score 54-78 (moderate), and score 79-99 (good)), and a higher score indicate a better quality of clinical education. The score ranges for the indicators of educational goals and curriculum, educators' performance, the way of communication between the educators and students, educational environment, and supervision and evaluation are 11-33, 9-27, 4-12, 5-15, and 4-12, respectively. The scores for the indicators are classified into three levels: 11-18 (weak), 19-25 (moderate), and 26-33 (good) for the indicator of educational goals and curriculum, 9-14 (weak), 15-20 (moderate), and 21-27 (good) for the indicator of educators' performance, 4-6 (weak), 7-9 (moderate), and 10-12 (good) for the indicators of the way of communication between the educators and students and supervision and evaluation, and 5-8 (weak), 9-11 (moderate), and 12-15 (good) for the indicator of educational environment [18]. The present study obtained a Cronbach's alpha of 0.92 for this questionnaire.
2.3.3. Clinical Self-efficacy
The clinical self-efficacy questionnaire comprises 37 items and four indicators, including the patient examination (12 items), nursing diagnosis (9 items), implementing care practices (10 items), and evaluation of care practices (6 items). Items are scored using a 4-point Likert scale (Complete incertitude=1, 0-20%), (incertitude=2, 30%-40%), (Relative certitude=3, 50%-70%), and (complete certitude =4, 80%-100%). The total score ranges from 37 to 148, and a higher score indicates higher self-efficacy. The total score is categorized into three levels: weak (37-74), moderate (74.10-111), and good (111.10-148). Cheraghi et al. developed this tool and reported its content validity, face validity, and reliability (Cronbach's alpha=0.96) [24]. In addition, this questionnaire has been used in several studies in Iran and its content validity and reliability have been approved [23, 25, 26]. The Cronbach's alpha of 0.98 was obtained for this questionnaire in the present study.
2.4. Ethical Considerations
The permission was obtained before the study from the Clinical Research Development Unit of Loghman Hakim Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran (Ethics Code: IR.SBMU.RETECH.REC.1400. 546).
2.5. Data Analysis
Descriptive statistics were reported in the form of frequency (percent), mean ± standard deviation, median, and minimum and maximum values for the study variables. The Shapiro–Wilk test and histogram charts were used to check the normality assumption. Then, the statistical tests, including Mann-Whitney U and Kruskal-Wallis test, were applied to compare the variables. The Spearman correlation coefficient test was used to explore the relationships between the scores for the two questionnaires and the statistical analyses were carried out by SPSS 22.
| Demographic Variables | Value | Clinical Education Status (Total Score) | P-value | Self-efficacy of Clinical Performance (Total Score) | P-value | |
|---|---|---|---|---|---|---|
| Age | Mean±SD | 23.59±3.49 | 0.150 | 0.01*a | 0.05 | 0.44a |
| [Minimum, Maximum] | [19, 46] | |||||
|
Gender n (%) |
Male | 99 (35.70%) | 60.43±12.52 | 0.002**b | 107.67±20.71 | 0.17b |
| Female | 178 (64.30%) | 55.68±12.10 | 103.33±24.12 | |||
|
Semester n (%) |
7th | 149 (53.80%) | 58.03±12.68 | 0.35b | 104.63±23.03 | 0.79b |
| 8th | 128 (46.20%) | 56.63±12.13 | 105.17±23.08 | |||
|
Study field n (%) |
Nursing | 220 (79.40%) | 57.52±11.86 | 0.27c | 105.03±23.05 | 0.23c |
| Operating room | 26 (9.40%) | 59.65±12.99 | 98.07±20.50 | |||
| Anesthesia | 31 (11.20%) | 54.45±15.47 | 109.51±24.11 | |||
|
simultaneity (employment, education) n (%) |
Yes | 137 (49.50%) | 56.15±11.96 | 0.10b | 106.04±21.85 | 0.69b |
| No | 140 (50.50%) | 58.58±12.80 | 103.74±24.12 | |||
3. RESULTS
3.1. Characteristics of Participants
A total of 277 students with a mean age of 23.59±3.49 participated in the study and most of them were nursing students (79.40%). 64.30% were female, 53.80% were students in the 7th semester, and 49.50% worked simultaneously with education. The variables of age and gender significantly correlated with the total score for the quality of clinical education. As the age of students increased, the total score for the quality of clinical education increased (r=0.15, P-value=0.01). The mean of the total score for the quality of clinical education was higher in males (60.43±12.52) than in females (55.68±12.10, P-value<0.01). Other relationships were not significant (Table 1).
3.2. Clinical Education Status
Table 2 presents the descriptive statistics for the quality of clinical education. The mean of the total score for the clinical education quality was equal to 57.38±12.43. The level of clinical education quality was considered weak by 37.20% of students, moderate by 57% and good by 5.80%. The indicator of educational goals and curriculum was rated as weak by 60.30% of the students, and 43.70% and 30.30% of students considered the indicator of educators' performance moderate and good, respectively. 50.50%, 38.30%, and 11.20% of the students considered the indicator of the way of communication between the educators and students weak, moderate, and good, respectively. Most of the students evaluated the indicator of the educational environment weak (41.20%) and moderate (52%). The indicator of supervision and evaluation was rated as weak by 49.80% of students, moderate by 38.30%, and good by 11.90%.
3.3. Self-efficacy of Clinical Performance
Table 2 presents the descriptive statistics for clinical self-efficacy. The mean of the total score for the self-efficacy of clinical performance was equal to 104.88±23.01. The level of clinical self-efficacy was considered weak by 11.60% of the students, moderate by 51.60%, and good by 36.80%.
3.4. Correlations between the Quality of Clinical Education and Clinical Self-efficacy
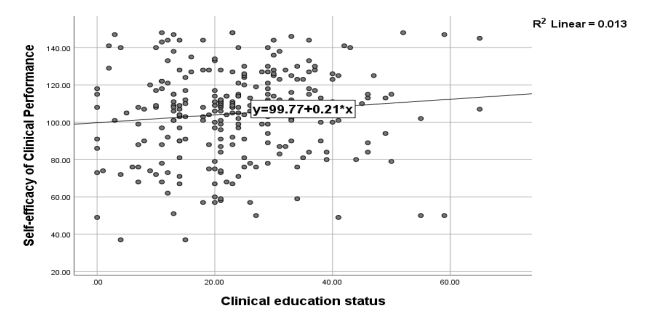
Table 3 shows the correlations of the indicators of the two questionnaires. The indicator of nursing diagnosis had a significant positive correlation with the educational goals and curriculum (r=0.12, P-value=0.04), the way of communication between the educators and students (r=0.13, P-value=0.04), the educational environment (r=0.14, P-value=0.02), and the total score for the quality of clinical education (r=0.13, P-value=0.03). There was a significant correlation between the indicator of implementing care practices and the way of communication between the educators and students (r=0.15, P-value=0.01) and the total score for the quality of clinical education (r=0.12, P-value=0.04). The total score for clinical self-efficacy had a significant correlation with the educational environment (r=0.13, P-value=0.04), the way of communication between the educators and students (r=0.13, P-value=0.04), and the total score for the quality of clinical education (r=0.12, P-value=0.04). Fig. (1) shows the positive correlation between the total scores for the two questionnaires.
| Questionnaire | Mean ±SD | Median (Min, Max) |
Classification n (%) |
||
|---|---|---|---|---|---|
| Weak | Moderate | Good | |||
| Clinical Education Status | - | - | - | - | - |
| Total score | 57.38±12.43 | 56 [33,98] | 103 (37.20) | 158 (57) | 16 (5.80) |
| Educational goals and curriculum | 17.22±4.72 | 16 [11,32] | 167 (60.30) | 97 (35) | 13 (4.70) |
| Educators' performance | 17.83±4.87 | 18 [9,27] | 72 (26) | 121 (43.70) | 84 (30.30) |
| The way of communication between the educators and students | 6.78±2.16 | 6 [4,12] | 140 (50.50) | 106 (38.30) | 31 (11.20) |
| Educational environment | 8.78±2.19 | 9 [5,15] | 114 (41.20) | 144 (52) | 19 (6.90) |
| Supervision and evaluation | 6.77±2.15 | 7 [4,12] | 138 (49.80) | 106 (38.30) | 33 (11.90) |
| Self-efficacy of Clinical Performance | - | - | - | - | - |
| Total score | 104.88±23.01 | 108 [37,148] | 32 (11.60) | 143 (51.60) | 102 (36.80) |
| Patient examination | 34.31±7.65 | 35 [12,48] | - | - | - |
| Nursing diagnoses | 24.82±6.46 | 27 [9,35] | - | - | - |
| Care practices | 29.09±6.42 | 30 [10,40] | - | - | - |
| Evaluation of care practices | 16.66±4.78 | 18 [6,24] | - | - | - |
| - | - | Self-efficacy of Clinical Performance | ||||
|---|---|---|---|---|---|---|
| Indicators | Patient examination | Nursing diagnosis | Implementing care practices | Evaluation of care practices | Total score | |
| Clinical education status | Educational goals and curriculum | r=0.04 P=0.46 |
r=0.12 P=0.04* |
r=0.07 P=0.21 |
r=0.06 P=0.35 |
r=0.09 P=0.13 |
| Educators' performance | r=0.00 P=0.99 |
r=0.02 P=0.72 |
r=0.07 P=0.26 |
r=0.54 P=0.28 |
r=0.04 P=0.48 |
|
| The way of communication between the educators and students | r=0.06 P=0.36 |
r=0.13 P=0.04* |
r=0.15 P=0.01* |
r=0.11 P=0.06 |
r=0.13 P=0.04* |
|
| Educational environment | r=0.11 P=0.07 |
r=0.14 P=0.02* |
r=0.08 P=0.16 |
r=0.07 P=0.28 |
r=0.13 P=0.04* |
|
| Supervision and evaluation | r=0.05 P=0.45 |
r=0.10 P=0.09 |
r=0.08 P=0.16 |
r=0.09 P=0.11 |
r=0.11 P=0.07 |
|
| Total score | r=0.06 P=0.35 |
r=0.13 P=0.03* |
r=0.12 P=0.04* |
r=0.09 P=0.12 |
r=0.12 P=0.04* |
|
4. DISCUSSION
This study aimed to determine the quality of clinical education and the clinical self-efficacy of nursing students during the COVID-19 pandemic. The study's findings showed a significant correlation between the total score for the clinical self-efficacy of nursing students and some of its aspects and the total score for the quality of clinical education. Clinical education includes such indicators as the educators' performance, educational goals and curriculum, the way of communication between the educators and students, educational environment, and supervision and evaluation, each of which has been discussed below.
In the present study, the mean score for the quality of clinical education of nursing students was reported to be at a moderate level, which is consistent with the results of most studies conducted on the quality of clinical education in Iran [18, 21]. Clinical educators greatly impact the quality of education, and their performance is considered the most effective indicator of clinical education [27]. In this study, students confirmed the relationship between the quality of clinical education and the educators' performance and educational goals, consistent with most studies conducted in Iranian nursing and midwifery schools [11]. In the study by Rahbar et al. [28], which was conducted in the context of traditional education before the COVID-19 pandemic, the performance of educators and their knowledge were reported to be at an undesirable level. In clinical settings, educators must be able to make connections between theoretical and clinical education, and the acquisition of clinical skills by students is directly related to the characteristics of the educators. Differences in students' views on the educators' performance can be due to cultural and social differences, the level of educators' skills, the level of education, the lack of sufficient qualified educators, and different conditions of education [11]. Thus, the changes in the method of education and the conditions of hospitals due to the COVID-19 pandemic could also affect students' views on the quality of clinical education in the present study.
Communicating appropriately with students is one of the characteristics of an effective educator [11]. In this study, the students considered the communication between the educators and the students undesirable. This is in line with the results of the studies by Baraz et al. [29], Jamshidi et al. [30], and Delaram et al. [31], in which this indicator was reported to be at a moderate level. However, it is in contrast to the findings of the study by Bahrami et al. [32] that reported a high level of this indicator. The most important reasons for students' dissatisfaction with how educators communicate with them are insufficient clinical supervision, inappropriate approach to using educational strategies, inappropriate evaluation process, lack of sufficient faculty members, lack of nurses, clinical training by educators with no experience in clinical practice, and financial constraints for training nurses [29, 33]. On the other hand, the present study was conducted during the COVID-19 pandemic when the universities were closed, the internships were postponed, and the teaching methods were changed [34], all of which can affect educators' communication with students.
In this study, the educational environment was not favorable from the students' points of view. This can be because clinical settings are inherently stressful. Such factors as new situations, fear of providing the wrong care, uncertainty about the results of care practices, changes in patient conditions, lack of familiarity with the clinical setting, and the feeling of being under supervision play a role in making students anxious in the clinical settings [11]. A large number of students versus the insufficient number of patients in clinical wards, lack of adequate physical space in hospital wards, and insufficient training of students in the clinics are the most common causes of the dissatisfaction of nursing students with the clinical settings [30]. On the other hand, this study was performed during the COVID-19 pandemic when the duration of internships in the faculty of Nursing and Midwifery of Shahid Beheshti University was limited and students and educators had limited access to personal protective equipment and students were very anxious about being infected with the virus in clinical settings [35]. Increased anxiety in the settings considered for the internship can have a negative effect on the quality of life and clinical education [34]. The clinical settings are a key place for nursing students and a suitable clinical learning environment is created through good cooperation between the schools of nursing and clinical educators [36]. Therefore, it is necessary to establish standards for teaching hospitals to ensure high-quality education [20].
In the present study, students were dissatisfied with the supervision and evaluation methods and the educational goals and curriculum. Thus, they were considered undesirable. This is consistent with the results of the study of Tavakoli et al. [21]. This study was conducted during the COVID-19 pandemic when nursing students were at the forefront of the fight against coronavirus disease. There was little evidence of official plans to support them in this transition from education to full-time professional nursing [34]. With the outbreak of the coronavirus disease, universities were closed, internships were postponed, students did not take the courses needed to administer care to patients, and there was no plan to assess their educational needs [34].
Many studies have considered the clinical self-efficacy of nursing students because nursing students should be able to apply independently what they have learned during their studies [37]. Clinical self-efficacy indicates the ability to provide independently patient care and its increase is associated with improved clinical performance of nursing students [38]. In the present study, the mean score for the clinical self-efficacy of nursing students was reported to be at a moderate level, which is consistent with the results of the studies by Bahador et al. [37], Mohammadi et al. [25], and Salimi et al. [10]. Lack of attention to improving clinical self-efficacy leads to reduced quality of the performance of the workforce trained for nursing [38]. The results obtained by some studies [39, 40] are inconsistent with the present study's findings and a high mean score has been reported for clinical self-efficacy. This could be due to the changes in clinical education conditions during the COVID-19 pandemic and the differences between the education system of Iran and other countries.
In this study, nursing students' clinical self-efficacy was low in evaluating the care practices needed for patients. This could be due to the insufficient presence of nursing students at the patient's bedside and the reduction of the clinical training hours to prevent the transmission of the virus during the COVID-19 pandemic. The internship programs are one of the most important components affecting students' clinical performance, which aims to strengthen the self-efficacy of nursing graduates [41]. On the other hand, evaluating the care practices needed for some chronic patients requires monitoring for several days, which is beyond the responsibility of nursing students during the internship. Additionally, the clinical self-efficacy of nursing students was high in terms of patient examination, which could be due to participating in workshops on health status examination during the COVID-19 pandemic.
The findings of the study have shown that the higher students’ satisfaction with the educational goals and curriculum, educational environment, and the way of communication between educators and students, the higher the mean score for the clinical self-efficacy of nursing students in terms of nursing diagnosis. Therefore, it can be concluded that education in a clinical setting is influenced by the educators' performance, the characteristics of the clinical setting, and the goals of clinical education, which also affect the clinical self-efficacy of the students' performance. Studies show that inconsistencies between theoretical and clinical courses, unclear goals of clinical education, stressful hospital environment, less inclination of experienced educators to participate in clinical education, poor teacher-student interaction, and inadequate evaluation system are the most important factors influencing the quality of clinical education [18]. On the other hand, the present study was conducted at the time of the outbreak of coronavirus disease when nursing students and educators in hospitals were afraid of COVID-19 and had limited access to personal protective equipment, educational goals and programs had changed, and attending a clinical education setting was associated with a risk of disease transmission.
This study showed that the higher the total score for the quality of the clinical education and the way of communication between educators and students, the better the students' performance in implementing the care practices. This is consistent with the findings of Rich and Nugent [41]. Establishing proper communication between the educators and the students, informing the students about the educational goals, and transferring knowledge and experiences to them play a role in the effectiveness of clinical education, increase self-efficacy, and lead to providing high-quality care services to patients [41]. During the COVID-19 pandemic, the internship programs were limited due to the high prevalence of coronavirus disease and students gained no experience in clinical patient care while the nursing students spent most of their time in the clinic to provide patient care before the COVID-19 pandemic. Changing the conditions of education and the way of communication between the educators and the students affected the clinical performance of nursing students who provided care for patients. This manifests the importance of appropriate communication between the educators and the students and the improvement of the quality of clinical education because nursing students are the group who has the closest relationship with the treatment team and will be part of the health care system in the future.
There was a significant positive correlation between clinical self-efficacy and the total score of the quality of clinical education, the way of communication between educators and students, and the educational environment. This means that the higher the score for the quality of clinical education in the fields of communication between educators and students, the more total score of their clinical self-efficacy. Therefore, it can be said that proper communication between educators and students is of special importance in the effectiveness of clinical education and increasing self-efficacy. The present study was conducted at the time of the COVID-19 pandemic. Changing the education conditions, the need to follow health protocols when attending clinical settings, and shortening the internship programs could affect the quality of the clinical education, and as nurses are key elements in the health care system, their educators must be able to provide appropriate training for them.
Before the COVID-19 pandemic, medical and paramedical education tried to use alternative technologies, simulation of clinical courses, and virtual education [42]. COVID-19 led to the expansion of virtual educational methods with many advantages, such as educational flexibility, the possibility of accessing educational content, student-centered learning [43], and the expansion of education based on the simulation of clinical settings [44]. However, challenges and disadvantages such as high cost, dependence on the Internet, technical and financial problems, complete mismatch of the provided content with existing needs and low quality of learning were associated with them [45]. Thus, considering the possibility of the outbreak of various unpredictable diseases and pandemics in the future, new methods that are appropriate to the conditions and the needs of students who provide clinical care services for clinical education should be taken into account [9].
CONCLUSIONS
In the present study, students considered the quality of clinical education and the clinical self-efficacy of their performance to be at a moderate level. This finding shows that improving the quality of clinical education requires attention to the opinions of students as the main elements of education, continuous investigation of the current clinical education quality, recognizing strengths, and correcting weaknesses. Since the problems of clinical education have adverse effects on achieving the educational goals, the clinical performance of nursing students, and ultimately the community health, the improvement of the quality of clinical education should always be considered. During the COVID-19 pandemic, changes were made in the health needs and the prevention and treatment methods.
Therefore, to improve the ability and self-efficacy of the clinical performance of nursing, operating room nursing, and anesthesia nursing students, nursing educators should use new methods of virtual education and create a curriculum based on the needs of the learners, the conditions, and the evidence that reflect the students' educational needs.
This study may provide nursing educators and supervisors with ideas and material to design educational initiatives based on the specific educational needs in nursing student settings. Additionally, based on the findings of this study, future research could investigate the specific education content needed for each competency.
LIST OF ABBREVIATION
| OR | = Operating Room |
| SD | = Standard Deviation |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study has been reviewed and approved by the Research Ethics Committee of Shahid Beheshti University of Medical Sciences. The participants provided their consent for participation in this study.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from all participants.
STANDARDS OF REPORTING
STROBE guidelines and methodologies were followed in this study.
AVAILABILITY OF DATA AND MATERIALS
The datasets are available from the corresponding author on reasonable request.
FUNDING
This study was funded by Shahid Beheshti University of Medical Sciences.
CONFLICT OF INTEREST
There are no conflicts of interest.
ACKNOWLEDGEMENTS
The authors express their gratitude to the Clinical Research Development Unit of Loghman Hakim Hospital, Shahid Beheshti University of Medical Sciences, for their support and cooperation during the study.

