All published articles of this journal are available on ScienceDirect.

Investigation of Burnout, its Associated Factors and its Effect on the Quality of Life of Critical Care Nurses Working in Buraydah Central Hospital at Qassim Region, Saudi Arabia
Abstract
Background:
Burnout is a grave problem for critical care workers because they are exposed to prolonged psychosocial stressors, including advanced technology, high responsibilities and great patient acuity. The aim of this study was to investigate burnout, its associated factors and its effect on self-care among critical care nurses.
Methods:
A descriptive correlational research design was carried out with 170 critical care nurses at Buraydah Central Hospital at Qassim Region in Saudi Arabia. A self-administered questionnaire including socio-demographic and work-related characteristics was used, as well as the Short Form SF12 to assess the quality of life, and the Maslach Burnout Inventory (MBI) to assess the level of burnout.
Results:
The three Maslach Burnout Inventory subscales, high emotional exhaustion and depersonalization, low personal accomplishment and moderate total burnout score were used. The quality of life measure (sF12) showed moderate levels of physical, mental component score and total score of quality for the critical care nurses. Factors associated with burnout include age, nationality, and years of experience and the wish to change department showed statistical significance. Burnout and quality of life score had a significant negative correlation.
Conclusion:
Age, nationality, years of experience and wish to change department are all significantly associated with burnout. Finally, burnout and quality of life score of these critical care nurses had a negative significant correlation.
1. INTRODUCTION
Well-being is an important health care aspect for professional support in health service delivery. Poor well-being can disturb their performance at work as well as patients’ safety [1]. Burnout is one of the destructive work-related health circumstances amongst healthcare workers. It is a syndrome of exhaustion related to work. It is characterized by emotional pressure, physical fatigue, and is frequently related to work strain and enthusiasm to a cause, a way of life that does not counterpart people’s expectations [2, 3, 4].
The prevalence of burnout can be elevated among Health Care Personnel in Arab countries as their health systems and financing status are either relatively low, overloaded or rapidly developing and responding to the altering disease forms and health status of the population. Numerous Arab countries have a serious lack of job responsibilities, causing them liable to burnout [5]. Intensive care unit nurses are highly probable to report high levels of work-related stress, and only a few of them are satisfied with their jobs compared with nurses employed in another ward [6, 7, 8]. Burnout is broadly termed, composed of three dimensions that include Depersonalization (DEP); decreased sense of professional and personal accomplishment (PA), which means failure to successfully manage work and reduced capability of self-motivation and Emotional Exhaustion (EE) defines the overextension in emotional feeling resulting in being overstrained in professional life and fatigue [2-4, 7]
It leads to unfitting psychological and physical consequences such as reduced occupation satisfaction, depression and reduced performance, serious family problems, absence from work and ultimately leaving a job in addition to, the bad physical condition of health care professionals suffering from disorders like cardiovascular disorders, physical fatigue, loss of motivation, depression, and anxiety [9, 10]. It may interrupt an organization's structures, lead to diminished efficiency in the workplace and to the decline of the quality of healthcare delivered, which can have an undesirable impact on the health system in general. Despite extensive research focused on this topic, burnout remains to be challenging for critical care nurses worldwide, [11]. It has been argued, for instance, that burnout is not merely accompanying with problems related to the working, but also influences learning theory, personality and environmental factors [12].
Quality of life (QOL) is one of the vital characteristics of human health. It is fixed in a cultural and social context. Poor QOL is strongly associated with reduced work performance, burnout and early retirement. Quality of life is determined to be linked to achieving a productive and healthy lifestyle and therefore, has been examined as an important parameter in several studies [13]. WHO describes the quality of life as people’s insight of their position in life in the setting of a culture in which they live and in relation to their expectations, goals, concerns and standards. It is a broad-ranging concept exaggerated in a complex method by the person' psychological state, physical fitness level of independence, social relationships, personal beliefs and their relationship to salient features of their environment [13, 14]. Besides, in the previous years have been linked with other's attacks as happiness, depression and life satisfaction in many populations such as healthcare workers. Many studies approve that psychological factors and burnout are interrelated. It is though not recognized, whether the quality of life is an additional factor that shows a role in this connection [15]. Minister of Health referred the matter to the High Authority of Health since2010 on the thought of quality of life at work as a portion of the guarantee of health care organizations. It has established the influence of deprived quality of life in the workplace on safety patient [16]. Burnout disturbs performance, productivity at work, and personality. The emotional reactions that the disease can induce in the long run contribute to a mental burden that will hardly naturally neutralize [8].
2. AIMS OF THE STUDY
The aim of this study was to investigate burnout, associated factor and its effect on the quality of life among critical care nurses working in Buraydah Central Hospital at Qassim Region in Saudi Arabia.
3. METHODS
The current descriptive correlational research design was used to implement this study.
3.1. Sample and Setting
The data has been implemented on working nurses at the intensive care unit, emergency units, step down ICU and Artificial Kidney unit (AHU) at Buraydah Central Hospital at Qassim Region, Saudi Arabia. The sample comprised of 170 from 200 nurses working in the before mentioned settings. A purposive sample used to select nurse's participants. The inclusion criteria are 18 years of age and older, worked full time to provide direct treatment to their patients, and employed in the hospital for minimum one year. Though, among the exclusion criteria were those who were on vacation, who did not respond correctly to the questionnaires, who suffered from any physical diseases, and who were not present within the data collection period required by the researchers.
3.2. The Tool of Data Collection
For data collection, a self-administrative questionnaire was implemented. These instruments consist of three parts as the following:
Part I: This part consist of two items first socio-demographic characteristics of the nurses such as age, gender, level of education, marital status, nationality, satisfaction with income and number of children. Second items include Work characteristics as years of experience, working hours/week, shifting working hours, first job in critical care and work rhythm.
Part II: Maslach burnout inventory (MBI)
This questionnaire tool used to assess burnout by using the French version of the Maslach Burnout Inventory (MBI) questionnaire [17]. It is consist of a 22-item questionnaire and composed of 3 dimensions of burnout include depersonalization (DP; 5 items) or dehumanization, emotional exhaustion (EE; 9 items), and personal achievement (PA; 8 items). Scoring system is the total score for each dimension is categorized as low, moderate or high. The lowest scores showed the absence of the burnout. Emotional exhaustion (EE) scores lower than 19 indicate low, while 19–26 are reflected average and scores above 26 are categorized as high EE. Depersonalization (DP) scores above 9 show high DP and scores amongst 6–9 are average. Personal achievement scores amongst 34 and 39 are reflected average and lower and above this variety are categorized as low and high. Each item has 7 Likert rating scale ranging from 1 to 7 points (1 = Strongly Disagree, 2 = Moderately Disagree, 3 = Slightly Disagree, 4 = Neither Agree, 5= Slightly Agree, 6 = Moderately Agree, 7 = Strongly Agree [18].
Reliability and Validity of MBI inside Iranian society have been recognized.MBI reliability was evaluated using Cronbach’s alpha coefficient, the outcomes of which are as follows: EE (0.71), DP (0.78) and PA (0.72). Content validity of MBI was evaluated using lawsh's technique and content validity index [19].
Part III: Short Form 12 (SF12) questionnaire
This questionnaire tool used to assess Quality of life by means of the Medical Outcome Study Short Form consist of 12 items or SF-12 [20]. This is a shortened version of the SF-36 assessing eight dimensions: physical limitation, physical functioning, general health, physical pain, social functioning, vitality, mental health, and emotional limitation. These were brief into two scales: a physical component score (PCS) and a mental component score (MCS), in agreement with the strategies for the SF-12 instrument [21] Together scores ranged between 0 and 100, with scoring higher indicate health better. These SF12-based summaries have been revealed to reproduce precisely both the PCS and the MCS derivative from the full SF-36 [22].
3.3. Data Collection Procedure
A Pilot study was implemented by the researcher after the preparing of the tools on 10% of the nurses to test the applicability of the questionnaire; then, essential changes were performed according to the results of the pilot study. After the permission of hospitals directors to conduct the study. Data were collected by the researcher collects data using self-administered questionnaire to collect data from nurses in the above-mentioned setting. Data were gathered in the period of time between June of 2019 until July of the same year. Researchers reviewed demographic information to sure that the nurses met the inclusion criteria. A questionnaire distributed at morning, evening, or night shifts and researchers went to the department of the considered hospital, delivered their permits and spoken the purposes of the research and then offered them questionnaires to complete a questionnaire by themselves. After gathering the questionnaires, incomplete cases were excluded. The time spent to complete the questionnaire was 3-5 minutes as observed.
3.4. Statistical Analysis
Data were fed to the computer and analyzed using IBM SPSS software package version 20.0. (Armonk, NY: IBM Corp) Qualitative data were described using the number and per cent. Quantitative data were described using the range (minimum and maximum), mean, and standard deviation. Significance of the obtained results was judged at the 5% level. The used tests were chi-square test for categorical variables, to compare between different groups, Monte Carlo correction (correction for chi-square when more than 20% of the cells have expected count less than 5, Pearson coefficient to correlate between two normally distributed variables and Spearman coefficient to correlate between two distributed abnormally quantitative variables.
3.5. Ethical Consideration
Consent from the Regional Ethics Research Committee of Qassim University planned hospitals, and nurses were attained. Numerous strategies were used to keep the nurse's rights, who decided to participate in this study. First verbal, oral consent of the nurses was got preceding to the administration of the questionnaire. The nurses were knowledgeable of the purpose of the study, and that they had the right reject to participate. Also, the volunteer nature of participation was tense, as well as privacy. Also, the nurses were stated that they could refrain from responding to any queries, and they can dismiss at any time. The anonymity of the nurses was kept at all times.
4. RESULTS
Table 1 presented that the highest percentage of the studied sample was less than 40 years old, most of them (93.5%) were female, (50%) were single and, most of them with a nursing bachelor (97.6%), 50% of the nurses were partially satisfied with income and more than half of the nurses have not children (60.6%).
| Socio-demographic data | No. | % |
| Gender | ||
| Male | 11 | 6.5 |
| Female | 159 | 93.5 |
| Age | ||
| < 40 | 102 | 60.0 |
| 30–39 | 54 | 31.8 |
| > 40 | 14 | 8.2 |
| Level of Education | ||
| BSc | 166 | 97.6 |
| MSc or PhD | 4 | 2.4 |
| Marital status | ||
| Single | 85 | 50.0 |
| Married | 81 | 47.6 |
| Divorced | 2 | 1.2 |
| Widowed | 2 | 1.2 |
| Nationality | ||
| Saudi | 21 | 12.4 |
| Non-Saudi | 149 | 87.6 |
| Satisfaction with income | ||
| Satisfied | 40 | 23.5 |
| Partially satisfied | 85 | 50.0 |
| Dissatisfied | 44 | 25.9 |
| Partially dissatisfied | 1 | 0.6 |
| Number of children | ||
| None | 103 | 60.6 |
| One child | 37 | 21.8 |
| Two or more children | 30 | 17.6 |
Table 2 displayed that nearly two-thirds (64.1%) of the nurses had working experience from 1-6 years. More than half of them (54.1%) Very much interesting with the job, 71.8% of them were working for more than 40 hours/week. Regarding the number of Sleeping hours, it was found that 68.8% of them had slept for 8 hours per day, while 90% of them first job at critical care setting. This table showed that in relation to work-related health more than half of them (57.6%) had ≥one-day sick leave during the last 12 month. Other occupational-related characteristics are shown in Table 2.
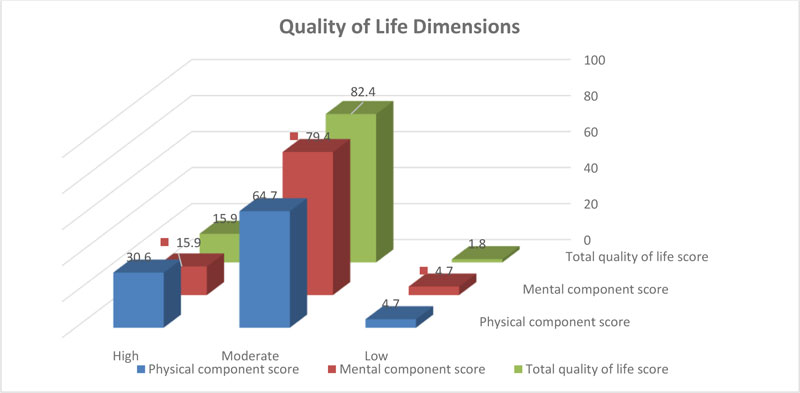
Fig. (1) indicated that a moderate level of quality of life of the studied nurses at physical, mental component score and total score of quality of life.
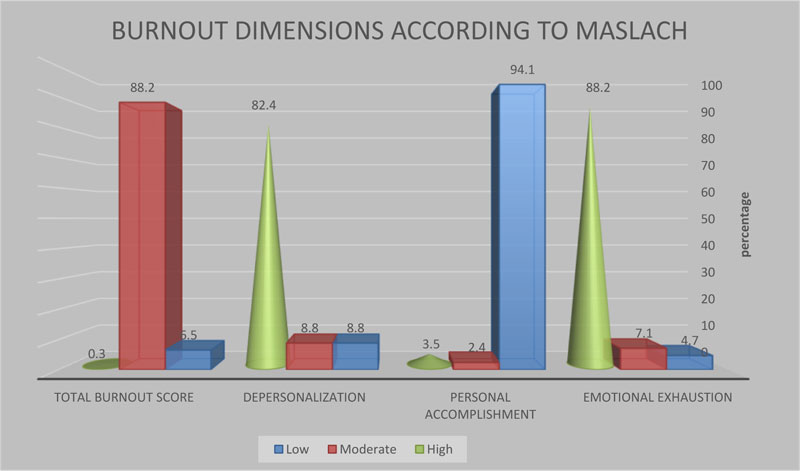
Fig. (2) revealed that according to Maslach burnout, found that the highest percentage of the nurses had a high level of burnout in emotional exhaustion and depersonalization dimension (88.2%, 82.4% respectively). Also, 94.1% of the nurses had a low level of burnout in personal accomplishment. In addition, most of the nurses have a moderate level in burn out in the total burnout score.
This (Table 3) illustrated that relation between burnout and socio-demographic data. Found that slightly more than half 55.6% of the Saudi nurses had high burnout while 90% of the non-Saudi nurses had moderate burnout that only statistically significant relation between burnout, age and then burnout and nationality (p-value 0.044, 0.003 respectively) . Regarding gender found that most of nurses female had a high level of burnout. While nearly two-thirds of the nurses had low to moderate level of burnout among age less than 40 years old. Also, most of them were non-Saudi nationality have low to moderate level of burnout 90.0%. Concerning marital status found that majority of them were single, have a low level of burnout while 55.6% of the married have a high level. However, 55.6% of the high level of burnout were partially satisfied with income. Moreover, found that the majority of the studied nurses had moderate burnout level in all sociodemographic data.
| Occupationally Related Characteristics | No. | % |
| Work-related variables | ||
| Years of Experience | ||
| 1–6 Years | 109 | 64.1 |
| 7–10 | 31 | 18.2 |
| 11–15 | 24 | 14.1 |
| ≥ 16 years | 6 | 3.5 |
| Interest in the job | ||
| Very little | 5 | 2.9 |
| Little | 25 | 14.7 |
| Very much | 92 | 54.1 |
| Much | 48 | 28.2 |
| Working hours/week | ||
| ≥ 16 | 24 | 14.1 |
| ≤ 40 | 24 | 14.1 |
| ➢ 40 | 122 | 71.8 |
| Shift working hours | ||
| 8 hours | 168 | 98.8 |
| 12 hours | 2 | 1.2 |
| Number of Sleeping hours | ||
| ≥ 8 | 53 | 31.2 |
| 8 | 117 | 68.8 |
| First job in critical care | ||
| Yes | 153 | 90.0 |
| No | 17 | 10.0 |
| Time working in critical care (n = 153) | ||
| > 5 years | 80 | 47.1 |
| ≤ 5 years | 73 | 42.9 |
| Work rhythm (n = 153) | ||
| Night or day | 96 | 62.7 |
| Night versus day | 57 | 37.3 |
| Wish to change department | ||
| Yes | 35 | 20.6 |
| No | 135 | 79.4 |
| Work-related health | ||
| ≥ 1 sick leave during the last 12 months | 98 | 57.6 |
| At least one sick leave in the last 12 months | 72 | 42.4 |
| Physical activity and lifestyle | ||
| Regular sport activity | ||
| Yes | 37 | 21.8 |
| No | 133 | 78.2 |
| Smoker | ||
| Yes | 5 | 2.9 |
| No | 165 | 97.1 |
| Consumption of coffee | ||
| Yes | 121 | 71.2 |
| No | 49 | 28.8 |
| If yes number of cups of coffee per day (n = 121) | ||
| 4 cups of coffee per day | 109 | 90.1 |
| > 4 cups of coffee per day | 12 | 9.9 |
| Socio-demographic data | burnout | χ2 | MCP | |||||
|
Low (n = 11) |
Moderate (n = 15) |
High (n = 9) |
||||||
| No. | % | No. | % | No. | % | |||
| Gender | ||||||||
| Male | 1 | 9.1 | 8 | 5.3 | 22 | 22.2 | 4.242 | 0.077 |
| Female | 10 | 90.9 | 142 | 94.7 | 7 | 77.8 | ||
| Age | ||||||||
| < 40 | 7 | 63.6 | 93 | 62.0 | 2 | 22.2 | 8.743* | 0.044* |
| 30–39 | 3 | 27.3 | 47 | 31.3 | 4 | 44.4 | ||
| > 40 | 1 | 9.1 | 10 | 6.7 | 3 | 33.3 | ||
| Level of Education | ||||||||
| BSc | 11 | 100.0 | 146 | 97.3 | 9 | 100.0 | 0.412 | 1.000 |
| MSc or PhD | 0 | 0.0 | 4 | 2.7 | 0 | 0.0 | ||
| Marital status | ||||||||
| Single | 7 | 63.6 | 75 | 50.0 | 3 | 33.3 | 7.948 | 0.257 |
| Married | 4 | 36.4 | 72 | 48.0 | 5 | 55.6 | ||
| Divorced | 0 | 0.0 | 1 | 0.7 | 1 | 11.1 | ||
| Widowed | 0 | 0.0 | 2 | 1.3 | 0 | 0.0 | ||
| Nationality | ||||||||
| Saudi | 1 | 9.1 | 15 | 10.0 | 5 | 55.6 | 11.126* | 0.003* |
| Non-Saudi | 10 | 90.9 | 135 | 90.0 | 4 | 44.4 | ||
| Satisfaction with income | ||||||||
| Satisfied | 2 | 18.2 | 37 | 24.7 | 1 | 11.1 | 3.537 | 0.937 |
| Partially satisfied | 6 | 54.5 | 74 | 49.3 | 5 | 55.6 | ||
| Dissatisfied | 3 | 27.3 | 38 | 25.3 | 3 | 33.3 | ||
| Partially dissatisfied | 0 | 0.0 | 1 | 0.7 | 0 | 0.0 | ||
| Number of children | ||||||||
| None | 7 | 63.6 | 93 | 62.0 | 3 | 33.3 | 6.292 | 0.133 |
| One child | 1 | 9.1 | 34 | 22.7 | 2 | 22.2 | ||
| Two or more children | 3 | 27.3 | 23 | 15.3 | 4 | 44.4 | ||
Table 4 shown that the relation between burnout and occupational data found that there were no significant statistical differences in burn out level for all occupational characteristics except years of experience have significantly nurses had 1-6 experience years (72.7%) have low level of burnout while 33.3% of nurses have high level of burnout for more than 16 years of experience. Also, found a significant relationship between the level of burnout and wish of nurses don't wish to change department 90.9% have a low level, and 66.7% of nurses wish to change department has a high level of burnout. While the highest percentage of the nurses for >40 working hours/week had a moderate level of burnout, 100% of nurses have severed burnout for shifting working for 12 hours, and 72.7% of the nurses have low level of burnout very much interest in the job.
Table 5 shows negative significant correlation between emotional exhaustion and mental component score. In addition, there was a significant negative correlation between mental component score and a total score of burnout. Also, negative correlation between total burnout and total quality of life score
(Table 6) shown that there were negative significant correlation between burnout and satisfaction with income and also between interest in job and quality of life, in addition, there was a positive significant correlation between the quality of life and satisfaction with income. Also, there was a positive significant correlation between burnout and interest in the job.
| Occupational Characteristics | Burnout | χ2 | MCP | |||||
|
Low (n = 11) |
Moderate (n = 15) |
High (n = 9) |
||||||
| No. | % | No. | % | No. | % | |||
| Work-related Variables | ||||||||
| Years of Experience | ||||||||
| 1–6 Years | 8 | 72.7 | 99 | 66.0 | 2 | 22.2 | 18.448* | 0.002* |
| 7–10 | 0 | 0.0 | 28 | 18.7 | 3 | 33.3 | ||
| 11–15 | 3 | 27.3 | 20 | 13.3 | 1 | 11.1 | ||
| ≥ 16 years | 0 | 0.0 | 3 | 2.0 | 3 | 33.3 | ||
| Interest in the job | ||||||||
| Very little | 1 | 9.1 | 4 | 2.7 | 0 | 0.0 | 9.422 | 0.100 |
| Little | 0 | 0.0 | 21 | 14.0 | 4 | 44.4 | ||
| Very much | 8 | 72.7 | 80 | 53.3 | 4 | 44.4 | ||
| Much | 2 | 18.2 | 45 | 30.0 | 1 | 11.1 | ||
| Working hours/week | ||||||||
| ≥ 16 | 1 | 9.1 | 23 | 15.3 | 0 | 0.0 | 5.362 | 0.184 |
| ≤ 40 | 3 | 27.3 | 18 | 12.0 | 3 | 33.3 | ||
| > 40 | 7 | 63.6 | 109 | 72.7 | 6 | 66.7 | ||
| Shift working hours | ||||||||
| 8 hours | 1 | 9.1 | 1 | 0.7 | 0 | 0.0 | 5.091 | 0.219 |
| 12 hours | 10 | 90.9 | 149 | 99.3 | 9 | 100.0 | ||
| Number of Sleeping hours | ||||||||
| ≥ 8 | 4 | 36.4 | 46 | 30.7 | 3 | 33.3 | 0.389 | 0.858 |
| 8 | 7 | 63.6 | 104 | 69.3 | 6 | 66.7 | ||
| First job in critical care | ||||||||
| Yes | 11 | 100.0 | 133 | 88.7 | 9 | 100.0 | 1.155 | 0.582 |
| No | 0 | 0.0 | 17 | 11.3 | 0 | 0.0 | ||
| Time working in critical care (n = 153) | ||||||||
| > 5 years | 3 | 27.3 | 72 | 54.1 | 5 | 55.6 | 2.934 | 0.246 |
| ≤ 5 years | 8 | 72.7 | 61 | 45.9 | 4 | 44.4 | ||
| Work rhythm (n = 153) | ||||||||
| Night or day | 6 | 54.5 | 82 | 61.7 | 8 | 88.9 | 2.949 | 0.237 |
| Night versus day | 5 | 45.5 | 51 | 38.3 | 1 | 11.1 | ||
| Wish to change department | ||||||||
| Yes | 1 | 9.1 | 28 | 18.7 | 6 | 66.7 | 10.088* | 0.004* |
| No | 10 | 90.9 | 122 | 81.3 | 3 | 33.3 | ||
| Work-related health | ||||||||
| ≥ 1 sick leave during the last year | 6 | 54.5 | 85 | 56.7 | 7 | 77.8 | 1.525 | 0.509 |
| At least one sick leave in the last 12 months | 5 | 45.5 | 65 | 43.3 | 2 | 22.2 | ||
| Physical activity and lifestyle | ||||||||
| Regular sport activity | ||||||||
| Yes | 4 | 36.4 | 31 | 20.7 | 2 | 22.2 | 1.746 | 0.412 |
| No | 7 | 63.6 | 119 | 79.3 | 7 | 77.8 | ||
| Smoker | ||||||||
| Yes | 2 | 18.2 | 3 | 2.0 | 0 | 0.0 | 6.176 | 0.055 |
| No | 9 | 81.8 | 147 | 98.0 | 9 | 100.0 | ||
| Consumption of coffee | ||||||||
| Yes | 9 | 81.8 | 106 | 70.7 | 6 | 66.7 | 0.691 | 0.729 |
| No | 2 | 18.2 | 44 | 29.3 | 3 | 33.3 | ||
| If yes number of cups of coffee per day (n = 121) | ||||||||
| 4 cups of coffee per day | 8 | 88.9 | 95 | 89.6 | 6 | 100.0 | 0.384 | 1.000 |
| > 4 cups of coffee per day | 1 | 11.1 | 11 | 10.4 | 0 | 0.0 | ||
| Burnout dimension | Quality of life dimensions | Total QOL score | ||||
| Physical component score | Mental component score | |||||
| r | p | r | p | r | p | |
| Emotional exhaustion | -0.098 | 0.202 | -0.388* | < 0.001* | -0.368* | < 0.001* |
| Personal accomplishment | -0.097 | 0.206 | -0.124 | 0.107 | -0.145 | 0.058 |
| Depersonalization | 0.117 | 0.127 | -0.091 | 0.236 | -0.027 | 0.723 |
| Total burnout score | -0.067 | 0.387 | -0.374* | < 0.001* | -0.343* | < 0.001* |
| Associated factors | Quality of life | Burnout | ||
| rs | p | rs | p | |
| Socio-demographic | ||||
| Age | 0.140 | 0.069 | 0.042 | 0.584 |
| Level of education | 0.088 | 0.253 | -0.095 | 0.217 |
| Satisfaction with income | 0.173* | 0.024* | -0.246* | 0.001* |
| Number of children | 0.113 | 0.144 | -0.062 | 0.423 |
| Occupationally related characteristics | ||||
| Years of experience | 0.061 | 0.428 | 0.089 | 0.250 |
| Interest in the job | -0.220* | 0.004* | 0.151* | 0.049* |
| Working hours/week | 0.044 | 0.566 | 0.005 | 0.946 |
| Shift working hours | -0.017 | 0.829 | 0.100 | 0.195 |
| Number of sleeping hours | -0.026 | 0.735 | 0.063 | 0.418 |
| Time working in critical care | -0.093 | 0.253 | -0.048 | 0.554 |
| Work-related health | -0.037 | 0.636 | 0.051 | 0.513 |
| Number of cups of coffee per day | -0.006 | 0.945 | 0.047 | 0.607 |
5. DISCUSSION
Burnout remains a chief working problem, in nursing and the sector of health in general, with many consequences that affect the nurses so that the study to investigate burnout, associated factors and effect on the quality of life. Among the sociodemographic data studied, only age and nationality were found to be significantly associated with burnout. Our findings support previous studies which showed that causes such as age, significantly correlated with burnout among nursing [23]. Although some studies in contrast with finding [24]. Our findings explained that moderate quality of life level at physical, mental component score and total score of quality of life. Besides the highest mean at a physical component score of quality of life. It may be nurses in these units have an additional hard working setting due to many factors such as having to contract with patients in discomfort, several health problems. This result not in line with [25] found that 78-81% high nurses scored on burnout and low on QOL. Nurses working in Internal Medicine and General Wards had slightly higher scores on burnout compared to nurses of Gynaecology / Obstetrics ward lead to job dissatisfaction, burnout, and they planned to leave the job.
In the present study, among the three burnout dimensions in critical nurses showed high levels of Emotional Exhaustion EE and Depersonalization DP and low levels of burnout in personal accomplishment. This result congruent with [24-26]. While [27] inconsistent with the present result, found that emotional exhaustion lower level scores, however, personal accomplishment higher scores. It may be the changes between the studies may originate from settings of study and regional or sociocultural features. Such results approve with [28] which proposes that maladaptive managing with extreme stresses and reduction of one’s resources will effect in emotional exhaustion first, then depersonalization and decreased accomplishment personal follow. While our study is similar to other studies with great emotional exhaustion was showed in the 31 percentage of the participant nurse's low personal accomplishment was showed in the 38 percentage, and 24 percentage of more depersonalization [29]. Some authors reported that hospital nurses often believe they have too much workload, which may lead to tension at work [30].
Our findings can be compared to other Studies conducted in sub-Saharan Africa among physicians, nurses, and other healthcare personnel with prevalence rate estimates reaching from 40 to 80% [31]. While, among healthcare personnel in Arab countries, high burnout prevalence was assessed in the MBI subscales of personal accomplishment (13.3–85.8%) depersonalization (9.2–80.0%), and emotional exhaustion (20.0–81.0%) [5]. Finally, great prevalence rate of burnout has been described among pediatric nurses (21–39%) [31] and emergency room (26%) [32].
In addition, examining the relationship between sociodemographic variables and burnout illustrated that female higher burnout than male ranged from low to moderate. Burnout is often designated as a condition that mainly affects women. This result inconsistent with results found that do not have any relation between burnout and to female sex [33]. Concerning the relation between marital status and burnout found that married nurses have higher burnout levels compared to nurses single with insignificant relation. These finding similar in it may be married nurses sense less emotionally expended by the occupation, are additional caring towards patients and sense more satisfied by their profession. While single nurses, on the other hand, do not have to expression those problems. So, they can be fewer prone to burnout. Employed women are also commonly accountable for household responsibilities, and so this result imitates the evident effort of integration home and family requirements with those at work. The present study is inconsistent with [34]. Found that marital status predisposed significantly nurses’ to exhaustion emotionally and explained that marital nurses have support from partners to deal with difficulty or stress.
Present study results revealed that more than half 55.6% of the Saudi nurses had high burnout while 90% of the non-Saudi nurses had moderate burnout with statistically significant between burnout and nationality (p-0.003 respectively) .our study agreement with [5] found that nationality was significant associated with burnout . In addition, other researcher disagreement [35] found that non-Saudi nurses were significantly significant more disposed to great Emotional exhaustion than Saudi nurses. While, nearly two-thirds of the nurses had low to moderate level of burnout among age less than 40 years old. This result in the line with [36] found that older age merely correlated with lower physical capacity to work, and greater burnout associated with lower physical and psychological ability to work.
Also there was the relationship significantly between nursing personality, depersonalization and sex. This result inconsistent with [37] who found married nurses have higher levels of burnout compared to single nurses states. While [25], who found unmarried nurses do not have to face those issues. Therefore, they may be less prone to burnout. Also, the relationship between Occupational related characteristics and the burnout experienced by nurses. In this respect, there were statistically significant differences in interest of job between burnout of nurses. This finding is supported by other studies [38].
Regarding Relation between burnout and occupational characteristics found that years of experience have significantly low effect on burnout particularly for nurses had 0-6 experience years (72.7%) have low level of burnout 33.3%7-10 than more years of experience. This result in line with [38] found that the relationship between the length of employment and burnout seems with explanations that burnout complains may decline when persons become older. These relations may be explained by the development of improved managing strategies by additional experienced nurses, as together variables are closely connected with experience in professional.
The result of this study found that negative significant correlation between total Burnout score and Total quality of life score. Our results are similar to [39].These results were in agreement with [40] reported who conduct a study on a cross-sectional study for 322 clinical nurses employed in hospitals in Tehran and finding a statistically significant negative relationship between personal accomplishment and emotional exhaustion with nurses quality of life. In addition, we agree with the results of numerous studies [41, 42]. Also, other results explored burnout between nurses is considered to be malicious and negative. It harms both mental and physical health systems and stops the development of the nursing profession [43].
Regarding the correlation between emotional exhaustion and the physical component score of quality of life found no significant negative correlation. This result was in correspondence with prospective studies implemented with health workers display that exercise physically assistances mental health. Prior results also account that the more the strength of physical exercises, the lesser the levels of burnout, anxiety and depression, because exercises improve mental energy and decline work exhaustion by neurotransmitters release, such as serotonin, which leads a sensation of wellbeing. Moreover, it is a defensive factor for various chronic disorders, such as cardiovascular diseases [44, 45].
With regard to correlation between total burnout score and total quality of life score our study revealed that negative correlation between burnout and quality of life as higher burnout was correlated with lower quality of life. Which was consistent with previous research [46]. Found that negative correlation between Work-related burnout is with little Quality of life among nurse practitioner. Hospital/work setting was contributing variables to low Quality of life and more burnout [25]. Other studies in the same line found that a statistical significant relationship between Qality of life and burnout among nurses.
Concerning the correlation between associated factors and total score of burnout, quality of life of the nurses found that no significant correlation between age and burnout and also age and quality of life. These results were in agreement with [13] explored that not any correlations between age, burnout, working facilities and gender, there is strong evidence showing that improved levels of burnout have bad effects in quality of life in nursing occupation. Moreover, a positive correlation between interested in the job and burnout these previous studies in line with [47] found that nurses with jobs interested shown a lesser burnout. High levels of burnout might be revealing of a bad attitude to oneself and one's job, absence of interest and fulfilment towards the job, and low self-confidence. Nursing professionals are exposed to many factors that may impact professional health related quality of life. Some of these influences are connected to the work [48].
Regarding the marital status of nurses, the results of this study show that being married is a predictor of having a higher burnout, while being Widowed is a predictor of a lower burnout with no significant. Though, the studies [49] showed that being divorced was statistically significant associated to having lower burnout scores, although this study analyzed medical personnel only. The marital status factor is connected to the insight of social support. Possibly, in the work setting, the apparent social support of having a steady spouse is not an issue influencing satisfaction with work. Nursing professionals pursue support additional from spiritual beliefs [50] or co-workers than from personal relationships.
Our finding revealed that those with number of sleeping hours for 8 had higher burnout than nurse for≥8 but not statistical significant. This finding in the line with [51] reported that those with 'working day sleep hours more than 7 hours and catch-up sleep hours > 2 hours' had higher for work-related burnout (6.74 relative to those with less sleep). In general, the ideal period of sleep in terms of psychological well-being and subjectively perceived wellbeing is considered to be about 7–9 hours .38 While there is no evidence of associations between longevity [52, 53]. Even though, there is no suggestion displaying correlations between longer sleep periods and burnout, preceding studies have originate that extended sleep period (>9 hours) was related with an augmented possibility of anxiety, depression and diabetes [52, 53]. Additionally, we found that Working hours/week >40 hours had higher burnout. This finding in the same line with [54, 55]. Showed that extensive hours of work were a hazard factor for developed work-related burnout levels. Earlier studies also revealed that working above 40 hours/week and job more than 14 consecutive hours’ were independent danger factors related with burnout.
Regarding nurses working time in critical care setting for >5 years had higher burnout than nurses working for less than 5 years. This finding in agreement to other previous studies [53, 55, 56] length of service and age were not statistically significant hazards for burnout [57]. Other finding illustrated that the primary years of the occupation may be the greatest challenging years. The likely purpose behind this matter lies in the fact that older nurses experience numerous circumstances in the work setting over time and they can progressively absorb how to handle disagreeable situations. So, these nurses may experience fewer job burnout. Our findings found no correlation between working hours/week and burnout this results not agreement with [58] who found length hours work are associated with burnout when at work above 40 hours each week and is even stronger once working above 60 hours each week. Moreover, it was established that no correlation between age and total score of burnout this result inconsistent with [59].
Regarding the correlation between years of experience and burnout and also between years of experience and quality of life found that no significant correlation. These findings were in agreement with [60], who found that nurses had with working experience more burnout and a lesser QOL. Some latest also reported that once nurses primary start their jobs, their anxiety level is little. As for accountability rises and effort piles up, they start to experience stress. Many problems related to the cumulative number of patients raise the level of stress. With the passage of time, they learn to manage the situation and develop more resistant. Thus, nurses who have worked for extended periods are less disposed to burning out easily, and their QOL is kept. While concerning the correlation between having a number of children and burnout found that no correlation. This result disagreement with [61] who found that nurses were having a certain number of children connected with more EE and lesser PA scores.
CONCLUSION
The study concluded that critical nurses had a moderate level of PCS, MCS, total QOL and total burnout score. While the majority of them had a high level of burnout in EE, DP and low level of burnout in PA. In addition, the only significant relationship between burnout and age and also between burnout and nationality. While, there was a significant relationship between years of experience of nurses and burnout, and also between the change department and burnout for nurses. Moreover, a negative correlation between EE and MCS and even between MCS and total burnout. Only there was a correlation between associated factors such as satisfaction with income, interest in the job and overall burnout score and also between satisfaction with income, interest in the job and QOL of the nurses.
RECOMMENDATION
So, the prevention and reduction of burnout among main health care providers is a significant chore of directors of the health system. Strategies teaching nurses for managing with pressure and training life practices, given consultations, generating supportive environments and, psychology services, are approximate of the means that can limit the occurrence of burnout. These activities will consequence in augmented effectiveness and competence of health workers, reduction their burnout, and enhance the general wellbeing of society. Because effects of burnout are extensive with concerns not only for the individual professionally and personally, but also for healthcare systems and patient care. Additional research is required to confirm the results including the consequence of burnout and quality of life on patient.
LIMITATION
The convenience number of participants does not give the allowance to generalize this study. The study were conducted in the summer in Saudi Arabia, some nurses schedule their annual vacation this time of the year. Therefore, this affect on the number of participants.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Ethics Committee, registered at National Committee of Bio. and Med .ethics(NCBE) registration (No. H -04-Q-011) at general directorate of health affairs al- Qassim region, ministry of health KSA.
HUMAN AND ANIMAL RIGHTS
Not Applicable.
CONSENT FOR PUBLICATION
Not Applicable.
AVAILABILITY OF DATA AND MATERIALS
The authors confirm that the data supporting the findings of this study are available within the article.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest, financial, or otherwise.
ACKNOWLEDGEMENTS
The authors are thankful to the directors and the employees of the Buraidah Central Hospital at Qassim Region, Saudi Arabia for their kind support. In addition, the authors wish to thank all nurses who accepted to participate in this research project.

