All published articles of this journal are available on ScienceDirect.

The Development and Psychometric Evaluation of a Questionnaire on the Nurses’ Recognition of Elder Abuse by Family Caregiver
Authors Info & Affiliations
Abstract
Introduction:
Exploring the nurses’ recognition of elder abuse and related signs may lead to the knowledge of development solutions through the In-Service programs. To develop an instrument for the assessment of nurses’ recognition of elder abuse by family caregivers within the Iranian context and psychometrically evaluate its reliability and validity.
Methods:
The sequential combination exploratory mixed methods design was used to develop the questionnaire format, which involved two sections: the quantitative and qualitative step. The qualitative step included probing the Nurses’ recognition of elder abuse by family caregivers in two steps including the literature and related tools review and semi-structured interviews with nurses. The quantitative step was accomplished in two parts. The validity of questionnaire was checked using face, content, construct, and formal validity; and the reliability was probed using cronbach’s alpha reliability. The analyzed data were categorized into 67 items (three main groups namely evident signs of abuse, elder’s potential to get abused, and family caregiver’s potential to abuse and 6 sub-groups including inadvertency, physical abuse, financial misconduct, psychological abuse, sexual abuse, and risk factors). Three components from the exploratory content analysis gained 58.8% variance totally. The cronbach’s alpha for the 3 components were 0.79, 0.76, and 0.78, respectively.
Results:
The questionnaire on the nurses’ recognition of elder abuse by family caregiver can be applied to a wide variety of settings because of the broad range of methods utilised to generate items and domains, its comprehensive consideration of the principles of elder abuse, and its initial reliability and validity.
1. INTRODUCTION
Elder abuse is one of the domestic violence subcategories, which may bring irreparable damages like death [1], depression, anxiety, and chronic pain [2], frequently referring to the treatment centers as well as hospital admission [3]. Besides, the treatment cost and overall budget of elder abuse treatment are considerably high with an estimation of about 5.3 billion dollars spent in the United States each year for this purpose [4, 5]. Moreover, there are also social costs like prosecution, punishment, and rehabilitation of abused elder [6, 7]. The frequent referrals to the treatment centers as well as getting hospitalized also increase the workload of medical and nursing care. Nevertheless, to provide high quality and comprehensive care services alongside supportive, mental, and legal actions, nurses are required to have sufficient knowledge about this phenomenon [4, 8, 9] as the early diagnosis of elder abuse signs and symptoms is effective in developing early medical interventions and preventing the side effects [10]. However, despite being an important member of the treatment staff, nurses’ recognition and knowledge about the subject is not enough in this context [11, 12]. Mondiraghlou et al (2006) have shown that the medical and emergency ward staffs are not aware of how to recognize, report, and treat the elder abuse phenomenon and how to approach an abused elder [11]. According to another study, only 40% of 131 nurses working in the emergency wards of 5 hospitals in South Korea were aware of elder abuse [13].
| Comments and experiences of the participants | Code | Construct |
|---|---|---|
| I have frequently seen that the attendants of elders argue on the properties while they are still alive. Once, the first child of a confused elder brought a stamp paper to have his father’s finger print on a financial document during the hospital night shift. | Seizing the properties of elders without their knowledge. | Financial abuse |
| Elderly’s properties are seized without his/her awareness. | ||
Moreover, several studies have shown that the nurses’ knowledge on the elder abuse phenomenon is limited and most of the experiences are gained from the clinical settings, co-worker’s experiences, media, and social networks. For instance, 39.1% of participants gained knowledge about the phenomenon from radio and TV channels in the study conducted by Dedli et al [14]. Thus, lack of knowledge or having limited and false information can challenge the process of taking care of the elder.
1.1. Background
At present, the nursing curriculum in Iran offers a four year baccalaureate in nursing [15]. Nursing curriculum is defined as the totality of the philosophical approaches, curriculum outcome statements, overall design, courses, teaching-learning strategies, delivery methods, interactions, learning climate, evaluation methods, curriculum policies, and resources [16].
There is no syllabus for elder abuse, influensive factors and probable outcomes defined in the Iranian nursing curriculum. There is no in-service training provided for the nurses to receive regarding neither the elder abuse concept and the caring style nor the case-report process [10]. Several studies have defined the lack of a reliable and standard instrument, as one of the most important barriers in recognizing the elder abuse cases [17, 18].
Therefore, the issue is not known as an educational priority for nurses in health care providing systems point of view while the risk of misdiagnosis and arbitrary actions of nurses increase [19]. Meanwhile nurses can play an important role in recognizing the phenomenon and deploying well-timed and appropriate interventions due to their close encounter with the elderlies. Hence, they can not be easily ignored as the factors decreasing the elder abuse side-effects and treatment costs as well as increasing quality of life for elder abuse cases [20]. Therefore, probing the level of nurses’ recognition of elder abuse and its signs and symptoms can be useful in providing the knowledge upgrading initiatives by the in-service programs.
Available data suggest that the overall elder abuse prevalence in Iran is 56.4% with confidence interval of 95% (35.1-75.5%) [21]. It is concluded that; Iranian's nurses encounter with and take care of elderlies patients who have experienced abuse. In this context, using valid and reliable tools can be effective; however, existing papers and databases provide only a limited number of such tools, while most of them are made by researchers and are not psychometrically analyzed [5, 22, 23]. Therefore, the lack of appropriate tool has made us design and develop the questionnaire on the nurses’ recognition of elder abuse by family caregivers.
2. METHODS
The sequential exploratory mixed methods design was adopted to develop the questionnaire in this study, which involved two steps: qualitative and quantitative study. The study was conducted in Mazandaran province, Iran in 2016.
2.1. Step One: Qualitative Study
The nurses’ recognition of elder abuse by family caregivers was probed in two parts including the literature and related tools review and field work (semi-structured interviews with nurses) for the qualitative step. Several keywords, such as elderly, physical abuse, financial misconduct, psychological abuse, sexual abuse, inadvertency, misbehavior risk factors, nurses’ recognition of misbehavior and psychometrics were searched in Scopus, Ovid, Proquest, ScienceDirect, Pub Med, and CINHAL databases without setting any specific time-limit for the literature search. Finally, 82 papers were selected for the study. The textual content analysis was used for analyzing the papers. The data analysis process was started by studying papers carefully. Afterwards, a list of items for the final data check was prepared. For the next step, 23 items each covering a different aspect of elder abuse were selected.
The field work step consisted of data gathering from the detailed interviews determining the nurses’ recognition of elder abuse. Five geriatric nursing masters and 3 nursing PhD were selected as participants. All the participants with sufficient subject knowledge willingly joined the study. The sampling was purposive. Participants were selected on the basis of age, gender, working experience, graduation date, and the experience in caring for the elderly with different kinds of abuse to gain the maximum variability. Detailed semi-structured interviews were used for the data gathering. The interview guide questions like “What do you know about elder abuse signs and symptoms?”, “What kind of factors may put the elders at a risk of elder abuse in your opinion?”, “What are the threatening specifications of a caregiver putting the elder at a risk of abuse?”, “Can you give me some details of an elder being abused if you have the experience of threatening with such a patient?”, and “What are the actions that should be taken when a nurse faces the elder abuse phenomenon in your opinion?” were asked. In the interview, all the questions came sequentially according to the earlier response and the interview guide. Probing questions like “What do you mean?” or “Could you please give more details?” were designed, if needed. At the end, the participants were asked to state any missed detail or point, and subsequently they were informed about the possibility of further interviews. For conducting the interviews, empty rooms in a clinical set-up were selected, and the interviews lasted for 20 to 25 minutes. The data saturation appeared when the codes became repetitive, and no new category or subcategory was created. The interviews were transcribed for the data analysis, and the open coding was done by carefully reading the texts. Fifty five initial codes were extracted in this step. Categorizing and recognizing the differences and similarities were done by studying the extracted codes frequently. The relationship between the categories was determined as the data analysis proceeded. Finally, the extracted codes were organized in 3 themes.
The codes extracted from the literature review and field work were compared in the final analyzing step, and the similarities and differences between the codes were probed. Afterwards, drafting of the items according to the categories and subcategories was done to create the final concept of nurses’ recognition of elder abuse by family caregivers format Table 1.
2.2. Rigor
The data gathered in the qualitative step were carefully checked in order to fit the Guba & Lincoln criteria of credibility, dependability, confirmability, and transferability [24]. Enough sample size capable of getting the data saturation was used in both qualitative and quantitative step [25].
2.3. Questionnaire’s Validation
The psychometric evaluation of 78-itemed questionnaire was done in this step, which included the validity and reliability phases. The validity phase included the validation of face, content and, construct.
2.4. Face Validity
The face validity was checked in both qualitative and quantitative methods. It is considered as a degree in which the questionnaire appears effective in terms of its stated aims qualitatively. Ten nurses were asked to comment on difficulty, relevancy, and ambiguous levels to check the face validity qualitatively. Afterwards, the item impact method was applied to decrease or remove the inappropriate items and determine each item’s important as a quantitative method. Likert 5-point scale (absolutely important to absolutely unimportant) was used to study each item, and the nurses were asked to determine the importance of each item according to their experience.
2.5. Content Validity
Both qualitative and quantitative methods were used to check the content validity. Five nursing faculty members with sufficient working experience in both the clinical and theoretical settings were asked to comment on the grammar, wording, allocation, and scaling of the items. Two indices of CVI and CVR were used to check the content validity quantitatively.
2.6. Content Validity Ratio (CVR)
Lawash model (1975) was used to determine the CVR [26] in this study. Ten subject matter experts (nursing faculty members with the working experience in clinical settings, tool making, and teaching geriatric nursing subjects) were asked to check the necessity of items according to a 3-point scale including necessary, helpful but not necessary, and unnecessary. Later, the results were compared with the scale of Lawash. The minimum value of CVR according to the Lawash’s table and the number of experts (all responded to the questions) was set to 0.80. The item was considered necessary with a statically significant level (p<0.05) if the outcome number was larger than the table’s number. CVRstrict was used in this study which means that only the necessary options were kept in the CVR formula.
2.7. Content Validity Index (CVI)
The CVI was promoted initially by Waltz and Bausell (1981) [27]. Ten experts (the same people helped in CVR determination) were asked to check if each item fits in the Likert 4-point scale (from absolutely relevant to irrelevant) in order to determine the content validity of each item and to ensure whether the items were designed properly to create the constructs. In this study, the S-CVI was calculated.
2.8. Construct Validity
The construct validity is considered as a degree in determining the questionnaire’s efficiency in the created constructs [28]. The factor analysis was used to study the internal relationship between the variables and explore the categories of items that were tightly related [25]. Kaiser-Meyer-Olkin and Bartlett sphericity tests were used before extracting the components to ensure that the items were appropriately designed to analyze different factors. The KMO value of 0.7 or higher was considered as the condition of sample size sufficiency in the content analysis. Bartlett test of sphericity was used to check the level of correlation between the questionnaire’s items in a way that the merging of items is possible. According to the previous study, the required sample size for content analysis varies from 5 to 10 for each item [29]. Four hundred samples were used in this study for the exploratory content analysis. The exploratory factor analysis, analysis of the main components of Scree plot to estimate the appropriate number of factors, eigenvalues equal to and/or more than 1 and varimax rotation were used. The score of 0.5 was considered as the minimal factor load for each item of extracted components from the content analysis.
2.9. Reliability
The reliability of this study was checked using the internal consistency and stability methods. Cronbach’s alpha was used in the internal consistency method, and the minimum alpha was considered to be 0.6 [30]. The Test-retest and Interclass Correlation Coefficient (ICC) were used to check the stability by asking 25 nurses to fill the questionnaire two times in two weeks interval. The acceptable minimum for ICC was set at 0.4 [31].
3. RESULTS
Three main categories including “evident signs of abuse”, “elder’s potential to get abused”, and “family care giver’s potential for abusing” as well as 6 sub-categories including “inadvertency”, “physical abuse”, “financial misconduct”, “psychological abuse”, “sexual abuse”, and “risk factors” were extracted in the qualitative step. The 78-itemed questionnaire became a 71-itemed one after the face validity checks in which 5 qualitative and 2 quantitative items with scores less than 1.5 were eliminated .
Two items were reviewed in the content validity check and all the possible changes were applied. The quantitative survey of content validity was based on the CVR and CVI methods. Two items including “elder’s anxious look at the caregiver before answering nurse’s questions” and “elder’s race as a risk factor for being abused” were eliminated using CVR method. Two other items were also ignored after receiving a score of 0.73 and 0.75, respectively, in CVI method. The mean content validity score (S-CVI) for all the remaining items was equal to 0.91 in the next step.
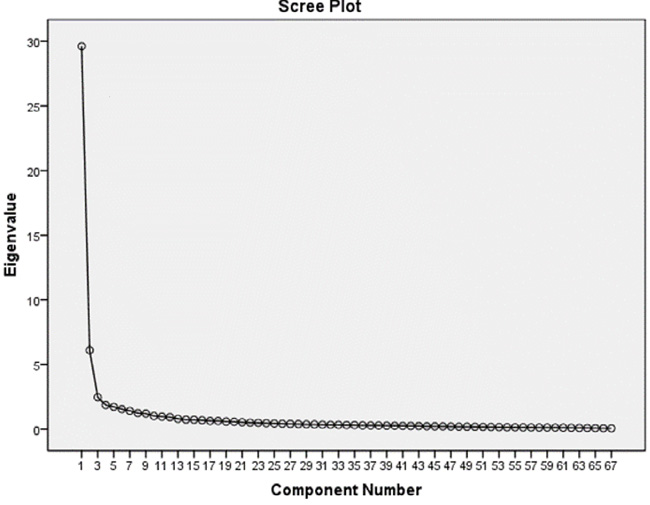
A 67-itemed questionnaire based on Likert 5 point scale (5 for strongly agree and 1 for strongly disagree) was prepared for the exploratory content analysis phase. A sufficient number of samples needed for the factor analysis using KMO equal to 0.985 were included in this study, collecting enough data for the analysis. Bartlett’s test was also statistically significant with the number of 20810.938 (p<0.001) which means that significant correlation exists between the items for the content analysis. To determine the number of components in Scree plot, eigenvalues were used. The Scree plot showed that 3 components are enough for exploring the factors affecting the nurses’ recognition of elder abuse by family caregivers (Fig. 1).
Afterwards, the extraction of the factor structure of the questionnaire by the principle component analysis using orthogonal rotation or varimax rotation (Eigen value>1) was carried out. The factor load of each item was considered to be minimum 3 in the factors matrix and rotated matrix. Three components having 58.8% variance according to the Scree plot were considered for this questionnaire.
3.1. The 1st Component
This component included 38 items related to the evident signs of abuse. The highest load factor was observed for the item “elder’s funds are managed by the caregiver, despite the elder’s ability of self-management and not having any intellectual or cognitive problem” and the minimum was for the item “elders are referred to the emergency ward repeatedly due to accidents”. The variance ratio for this component before the factor rotation was 44.186, which turned to 23.087 after it.
3.2. The 2nd Component
Twenty one items were included in this component stating the elder’s potential to get abused. The highest load factor was observed for the item “ elder has dementia or Alzheimer” and the minimum was observed for the item “elder lives in the remote areas”. The variance ratio for this component before the factor rotation was 9.106, which turned to 18.998 after it.
3.3. The 3rd Component
This component included 8 items stating the family care giver’s potential for abusing. Most of the load factor in this component was related to the item “the caregiver has child abuse experience from his/her parents” and the minimum load factor was related to the item “the caregiver is not skillful enough for caring an elder”. The variance ratio for this component before the factor rotation was 3.681, which turned to 14.888 after it. All the components were named according to their items after extraction, and the level of compatibility of each with the concepts and aspects of the questionnaire was studied Table 2.
| Factor 1 | Factor 2 | Factor 3 | Items |
|---|---|---|---|
| .567 | 1. The elder refers to the emergency ward repeatedly due to accidents. | ||
| .643 | 2. There is contradiction in elder’s reasons about contusions. | ||
| .660 | 3. Elder’s and caregiver’s reasons for illness or disease symptoms are in contrast. | ||
| .598 | 4. The caregiver prevents elder mentioning the reasons of disease or illness to the treatment staff. | ||
| .656 | 5. The caregiver prevents any private talk between the elder and treatment staff. | ||
| .614 | 6. The elder starts the treatment process late, despite his/her access to the treatment and care centers. | ||
| .649 | 7. The initiation of the treatment and rehabilitation process is significantly delayed; despite elder’s financial ability and access to the treatment and care centers. | ||
| .629 | 8. Lab reports show low or high consumption of drugs at home. | ||
| .708 | 9. Bruise, scratch, wound, burn, and other physical signs showing the elder has been limited or imprisoned are visible. | ||
| .636 | 10. The elder is suffering from oral venereal ulcers. | ||
| .673 | 11. The elder has broken bone frequently. | ||
| .630 | 12. The elder has sexually transmitted diseases or genital tract infections with unknown reasons. | ||
| .645 | 13. The elder is complaining about vaginal or rectal bleeding. | ||
| .657 | 14. Blood or other body fluids are visible on the elder’s clothes. | ||
| .687 | 15. The elder or the caregiver evades from giving the reason of blood or other body fluids on the elder’s clothes. | ||
| .670 | 16. The elder or the caregiver gets distressed or talking defensively about the reason of blood or other body fluids on the elder’s clothes. | ||
| .734 | 17. The caregiver has inappropriate relationship with the elder, e.g. not responding to the elder’s questions, reviling or humiliating the elder. | ||
| .752 | 18. The caregiver beats the elder. | ||
| .737 | 19. The elder is stressful while contacting his/her children. | ||
| .778 | 20. The elder is afraid of his/her caregiver. | ||
| .755 | 21. The caregiver threatens the elder about sending him/her to the old age home or other places. | ||
| .734 | 22. Elder’s comment or personality is ignored by the caregiver in presence of treatment staff or other patients. | ||
| .778 | 23. the caregiver declares personal satisfaction for discharging the patient, despite the elder’s choice and financial ability of receiving diagnosis and treatment services | ||
| .730 | 24. The elder’s properties are seized by the caregiver without his/her awareness. | ||
| .794 | 25. Elder’s funds are managed by the caregiver, despite the elder’s choice of self-management and having no intellectual or cognitive problem. | ||
| .779 | 26. Elder’s money or other valuable items are disappeared. | ||
| .726 | 27. Elder’s seal or signature feigned by the caregiver. | ||
| .714 | 28. Elder’s money or properties are taken for caring him/her. | ||
| .685 | 29. The elder looks like having no self-confidence or seems to be disappointed. | ||
| .613 | 30. The elder loses weight in a short period of time. | ||
| .647 | 31. Dehydration, diarrhea or malnutrition symptoms are visible in the elder’s face. | ||
| .576 | 32. The elder is not in good personal hygiene conditions. | ||
| .690 | 33. Bedsore or bladder infection symptoms are found on the elder’s body. | ||
| .708 | 34. The caregiver makes the elder wear clothes unsuitable for the season. | ||
| .655 | 35. Cigarette burn symptoms are visible on the elder’s body. | ||
| .673 | 36. No mental, psychological and financial supports are provided for the elder when he/she is in the treatment center. | ||
| .715 | 37. No visit is managed for the long periods of time. | ||
| .625 | 38. The caregiver is not willing to provide glasses, hearing aids or dentures. | ||
| .534 | 39. The elder lives in remote areas. | ||
| .549 | 40. The elder lives lonely at home. | ||
| .671 | 41. Elder has a blaming personality. | ||
| .675 | 42. Elder has aggressive behaviors when in contact with others. | ||
| .713 | 43. The elder usually insults his/her caregiver. | ||
| .704 | 44. The elder is usually complaining about his/her caregiver unreasonably. | ||
| .683 | 45. The elder is not able to participate in family decision makings. | ||
| .643 | 46. The elder is not able to manage his/her financial assets. | ||
| .663 | 47. The elder is not physically available to handle daily activities. | ||
| .646 | 48. The elder has chronic diseases. | ||
| .650 | 49. The elder has psychological disorders, e.g. depression and anxiety. | ||
| .775 | 50. The elder has dementia or Alzheimer. | ||
| .587 | 51. The elder is addicted to illegal drugs or alcohol. | ||
| .582 | 52. The elder has no relationship with family members, friends and neighbors. | ||
| .730 | 53. The elder is not able to solve his/her problems in a conversation. | ||
| .680 | 54. The elder hardly gets any changes in the daily routines and environment. | ||
| .637 | 55. The elder has experienced changes like solitude after losing his/her partner, disablement or house movements. | ||
| .633 | 56. The elder is physically disabled; e.g. blindness or deafness. | ||
| .771 | 57. The elder has experienced abuse or disrespect. | ||
| .675 | 58. The elder is financially dependent on his/her caregiver. | ||
| .645 | 59. The elder is mentally and emotionally dependent on his/her caregiver. | ||
| .677 | 60. The caregiver has not enough knowledge regarding elder caregiving. | ||
| .680 | 61. The caregiver is usually unsatisfied of keeping the elder. | ||
| .708 | 62. The caregiver suffers from the personality disorder or psychological problems. | ||
| .712 | 63. The caregiver is under high caring pressure (physical, mental, social or financial) due to caring from the elder. | ||
| .641 | 64. The caregiver is not skillful enough for caring an elder. | ||
| .677 | 65. The caregiver is addicted to illegal drugs or alcohol. | ||
| .724 | 66. The caregiver has child abuse experience from his/her parents. | ||
| .688 | 67. The caregiver is not able to properly serve the elder due to working long hours or in hard conditions outside. |
| Study areas | Number | Cronbach's Alpha | ICC |
|---|---|---|---|
| Evident signs of abuse | 38 (1-38) | 0.79 | 0.616 |
| Elderly’s potentials to get abused | 21 (39-59) | 0.76 | 0.368 |
| Family care giver’s potentials for abusing | 8 (60-67) | 0.78 | 0.552 |
| Total | 67 | 0.85 | 0.608 |
The total internal consistency of the questionnaire was found to be 0.98 in the reliability check. No item was removed in checking the consistency of each item in comparison to the questionnaire. The Test-retest method was used for probing the stability. The results showed that the scores of first and second tests were statistically significant (P<0.001), approving the repeatability of the subscales and the questionnaire besides showing high stability Table 3.
The questionnaire included three subscales including “evident signs of abuse”, “elder’s potential to get abused”, and “family caregiver’s potential for abusing”. The scoring scale in this questionnaire was based on the five-point Likert scale denoting strongly agree score with 5 to strongly disagree score with 1. The total score varied from 1 to 335, where the score 1-83 denoted weak recognition; 84-167 denoted medium recognition; 168-251 denoted good recognition; and 252-335 denoted excellent recognition of elder abuse by the nurses.
4. DISCUSSION
The present study involved the designing and development of a questionnaire with 67 items and three subscales on the nurses’ recognition of elder abuse by family caregivers, which was further checked for the reliability and validity. This questionnaire showed acceptable formal validity. The ratio of content validity to content validity index was also appropriate. The exploratory factor analysis was applied to all the 67 items to determine the construct validity. The KMO scale and Bartlett test also approved the factor analysis model. The eigenvalues proved the multifactorial specification of the questionnaire. Each item showed a fair relationship with one of the subscales and the structural validity degree of mean correlation seemed to be reasonable as indicated by the load factor of each item. The statistically significant relationship between the subscales and total score of the questionnaire was observed. The construct validity of the tool was approved according to the compatibility within the phrases resulted by the factor analysis and the definition and recognition aspects of the nurses’ recognition of elder abuse phenomenon by family caregivers.
Factor analysis has been used to determine the validity of the structure of elder abuse induced by family carers questionnaire by Heravi Karimavi (2010), Neale (1991), Cohen (2006) et al. [32-34]. Given the different definitions of the elder abuse, the number and naming of factors are different in this research, and none of the scales can distinguish between different types of abuses. Although the scale designed by Heravi et al. (2010) is somewhat in terms of dimensions similar to current study, but subscales ‘risk factors of elder abuse and sexual abuse’, have not been investigated [32]. While in current study, the items 10 and 16-12 examined the symptoms of sexual abuse. A scale developed by Cohen et al. (2006) can only identify the risk factors of elder abuse induced by family caregivers and can not identify signs of abuse in Iranian elderlies [33].
The item “elder’s funds are managed by the caregiver, despite being in good health, intellectual, and cognitive status” showed highest load factor in the first component. This may happen due to the financial problems and the economic pressure felt by the children [28] or the lack of awareness regarding the fact of abusing in this case. The elder’s children may consider using their parent’s funds as a basic right, leading to seizing parent’s properties without any permission. Similar conclusion has been observed in other studies as well. Sooryanarayana et al. (2011) have shown that the most prevalent type of elder abuse in Malaysia is related to the financial aspect (6.2%) [35]. The results of Karimi & Elahi (2008) have also proved that, after negligence (31.7%), financial aspect (25%) is considered as the main reason behind elder abuse in urban areas and sanatoriums [9]. In the 2nd component, the highest load factor was related to the item “elder has dementia or Alzheimer”. It is more usual to get abused due to the cognitive problems related to the Alzheimer and dementia, causing higher dependency on the caregivers [36].
The highest load factor in the third component was related to the item “the caregiver has child abuse experience from his/her parents”. The results of different studies have shown that elders are abused mostly by the family members and own children [37, 38]. Rosen et al (2016) have shown that 57% of elder abuse cases are related to the family members acting as caregivers [39].
The second and third factor with 29 items evaluates the risk factors of elder abuse. The risk factors of elder abuse are related both to the elderly and to the family caregivers. Identifying the risk factors of elder abuse helps nurses to provide interventions to prevent elder abuse. Heravi et al (2010) only identified the symptoms of elder abuse induced by family caregivers [32]. Then identification the risk factors of elder abuse can provide an opportunity for preventive interventions by nurses.
Hwalek-Sengstock Elder Abuse screening scale is also designed to investigate the risk factors of abuse, neglect, or exploitation in the elderly. The reliability of this scale (15 items) is equal to 0.855. (Cronbach's alpha:0.632) [18]. This scale has no symptoms of elder abuse. It is concluded that it can not be used by caregivers as a comprehensive scale to investigate the recognition of elder abuse.
CONCLUSION
The reliability details of our study seem to be encouraging. The reliability of the scale was checked both by the internal consistency and retest methods, thus, strengthening the reliability test results. The results showed that the questionnaire has good internal consistency. However, further analysis in bigger scales may show stronger relationships. This questionnaire, which we recommend as a mini scale, can be used both in statistical and practical studies. This questionnaire can also be helpful in analyzing the situation and needs assessment during the in-service trainings and educational interventions for the nurses; therefore, providing an easier way to increase the nurses’ abilities and skills for elderly care. The Nurses' Cognition of Elder Abuse Questionnaire was designed for Iranian family Caregivers. However, more surveys are needed in order to check the reliability of this questionnaire among the nurses with different cultures.
In this study, the sensitivity and specificity of the scale and the confirmatory factor analysis were not done using the structural equation method. Nevertheless, we believe that the careful qualitative research conducted and the exploratory analysis factor used in this study, will be used this scale in nursing care for the elderly, such as a hospital or other health centers, and even in Long-term care centers.
CONTRIBUTORS
All authors conceived and designed the study. FGh and AA managed the conduction of the collected the data. ZF and FGh supervised the analytical design and analysis which was conducted by FGh. The manuscript was drafted by ZF, and all authors contributed to critical revision and approved the final manuscript.
FUNDING
The study was funded by the Babol University of Medical Sciences. The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The main ethical considerations of this study include: receiving Babol University of Medical Sciences Ethics Committee approval, receiving informed consent, informing the participants about the aims, cooperation conditions, data gathering methods, recording the interviews and the role of both the researcher and the participant, respecting participant’s privacy, choosing the time and the place of interview according to participant’s convenience, having the right of resigning the study at any level and keeping all the data and information privately.The reference number is MUBABOL-REC 1395.34.
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for studies that are the basis of this research.
CONSENT FOR PUBLICATION
Written informed consent have been revised.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
This study was conducted with the support of Babol University of Medical Sciences with the ethic’s code of MUBABOL.REC.1395.34. We do appreciate all the patients, nurses, and the faculty members who helped us in designing the questionnaire.

