All published articles of this journal are available on ScienceDirect.

A Randomized Control Study on the Effectiveness of Holistic Health Practice Program on a Group of Baccalaureate Nursing Students
Abstract
Background:
From adolescents transitioning into professional healthcare team members, nursing students need to face different kinds of challenges during their journey of nursing study. Are nursing students ready and prepared to take care of themselves before taking care of others?
Aim:
Few studies were found on the holistic health of nurses in Macao. This study aims to explore the health status of a group of first-year undergraduate nursing students and to investigate whether a holistic health practice program can enhance their holistic health, self-esteem, and self-efficacy after they participate in the program.
Methods:
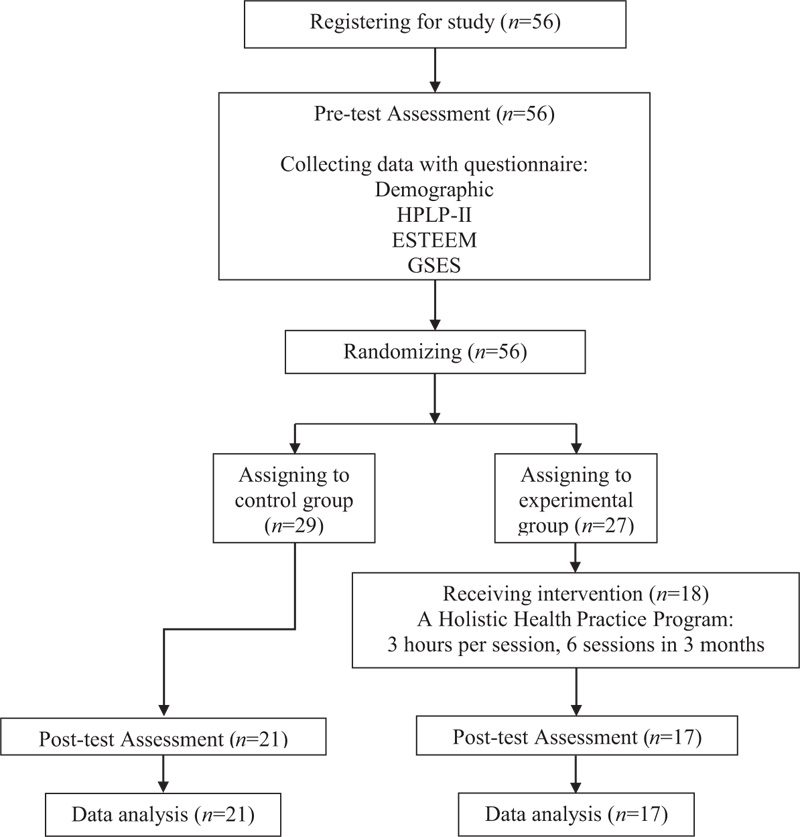
A randomized control study was used. Students in both the experimental and control groups filled in an online pre-test questionnaire, which consisted of some demographic information and the following measurement tools including, the Health Promotion Lifestyle Profile-II (HPLP-II), the Self-Esteem Scale (ESTEEM), and the General Self-Efficacy Scale (GSES). The experimental participants had to undergo an additional 6-sessions program on holistic health practice. After the intervention, all participants in both groups were invited to complete an online post-test questionnaire, which was the same as the one used in pre-study.
Results:
Results showed that participants’ physical activity was the lowest score in 6 domains, followed by their health responsibility. On the other hand, their spiritual growth scored the highest. The study found that participants who had attended the holistic health practice program had significantly enhanced their holistic health, self-esteem, and self-efficacy.
Conclusion:
This study provided some ground data of the holistic health status of nursing students in Macao. It also demonstrated that the Holistic Health Practice Program is effective in promoting holistic health, self-esteem, and self-efficacy among junior nursing students.
1. INTRODUCTION
Nursing students nowadays need to face many challenges during their course of study. Challenges may come from stressors related to their education, clinical placement, financial problem, self-confidence to perform certain nursing skills [1], and self-esteem related to the nursing profession [2]. One of the core challenges of nursing students is to take care of themselves at first and then care for others since it is the goal for all nursing students in the world [3].
During the transition from adolescents to professional healthcare team members, first-year nursing students experienced uncertainty with many of the nursing theories and concepts [4], and are inclined to drop out during their first-year or second-year of nursing study [5]. Despite that, nursing students still need to learn to develop their coping strategies to survive all these challenges during their education and clinical placement [4]. Studies found that nursing students lack physical activity [6, 7], therefore healthy lifestyle should be promoted among nursing students and incorporated into the nursing curriculum [7]. Are first-year nursing students able and ready to face the challenges during their nursing journey? Do they adopt healthy lifestyle behaviors before caring for others?
2. BACKGROUND
This study was carried out in a nursing school of a publicly-funded higher educational institute in Macao. The first-year nursing students of the public nursing school needed to complete core courses such as fundamental nursing, basic health assessment, anatomy, microbiology, pathophysiology, and pharmacology. Several studies had recommended promotion of healthy lifestyles and interpersonal communication skills to first-year nursing students, which could in-turn improve their self-esteem and self-efficacy in nursing study performance [4, 8-10]. However, physical education is an elective course for first-year nursing students in this program and is only arranged in the second semester in year one of the study, whereas, nutrition and applied psychology are subjects in the second year of the nursing curriculum. What is their health status holistically when they start to learn to be a nurse? There is an obvious knowledge gap in these areas therefore, this study aims to explore and investigate whether a holistic health practice program could help improve the holistic health, self-esteem, and self-efficacy and health promoting behaviors of baccalaureate nursing students.
What is health? Health was originally defined by the World Health Organization (WHO), in 1948, as a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmary [11]. In 1998, the spiritual dimension was added when describing health [12]. Later, different organizations and authors had added spiritual dimension when defining health from a holistic perspective. Holistic health is a goal and an approach of how one’s body, mind, and spirit get connected to one’s environment, in order to reach the maximum level of well-being [13]. Itharat et al. (2017) reviewed that a holistic approach can adjust hormones and immune system to defend against stress, anxiety, and depression, by breaking negative thinking and providing deep spiritual and emotional healing to the impaired human body function systems [14]. Luk (2013) emphasized the spiritual dimension in holistic care and stated that holistic care was the caring to meet the whole person’s needs in physical (nutritional and biological), psycho-social, cultural, and spiritual aspects, in order to maintain a healthy well-being [15].
Since holistic health is a comprehensive view of the whole person’s wellness including physical, psychosocial, and spiritual dimensions, not many tools have been developed for its measurement. The Health Promotion Lifestyle Profile (HPLP) consists of 6 domains covering assessment of a person in a holistic perspective and is widely used to explore the healthy lifestyles of participants throughout the world. It was also frequently used by researchers to investigate the healthy lifestyles of nurses and college students in Macao [16-18]. The 6 domains of the HPLP cover [19]:
1) Physical dimension including physical activity and nutritional habits;
2) Psychological dimension including health responsibility and stress management;
3) Social dimension including interpersonal relations and
4) Spiritual dimension including spiritual growth.
Therefore, the Chinese version of HPLP-II was adopted as one of the measurements in this study.
3. AIM
The aim of the study is to explore the holistic health status of nursing students and to investigate whether a holistic health practice program could help improve their health promoting behaviors, self-esteem, and self-efficacy.
4. METHODS
4.1. Design
A randomized control study method was used. Nursing students were invited to join the study on a voluntary basis by signing a consent form with detailed information concerning the current study. They were randomly divided into two groups by using block randomization: control group and experimental group. Students in both the experimental and control groups were asked to fill in an online pre-test questionnaire, which included demographic information, and the measurement (i.e. HPLP-II, ESTEEM and GSES) to determine their health promoting lifestyle, self-esteem, and self-efficacy, respectively. In addition, only the students in the experimental group had to participate in a 6-session program of holistic health practice, introducing physical health (enhancing physical activity, nutrition, and sleep), mental health (managing stress), social health (interpersonal relationship), and spiritual health (pursuing meaning of life) to them. Participants must meet the 80% attendance criterion of the program in order to take part in the post-test of this survey. Furthermore, after 6 sessions, all participants in both groups were invited to complete an online post-test questionnaire, which had the same content as the online pre-test questionnaire.
4.1.1. Intervention – The holistic health practice program
The holistic health practice program comprised of 6 sessions, which were conducted within 3 months, one session biweekly, with 3 hours per session. The dates of the 6 sessions were set on Saturdays, to avoid overlapping with the classes of the nursing school. The 6 sessions included: (1) the assessment of holistic health and designing a personal health promoting program; (2) maintaining physical health by enhancement of healthy diet and nutrition, physical activity and sleep; (3) developing mental health and managing life stress; (4) promoting social health by enhancing interpersonal relationship; (5) understanding spiritual health and pursuing the meaning of life; and, (6) group presentation of their pursued health promoting program. This holistic health practice program covered the whole human body well-being including physical, mental, social, and spiritual health aspects. The program is designed by the Nethersole Institute of Continuing Holistic Health Education, a unit under the Alice Ho Miu Ling Nethersole Charity Foundation, a charity foundation for the promotion of holistic health to the healthcare staff in Hong Kong. The program was conducted by their staff who were experienced healthcare professionals including 2 nurses and a medical social worker. The holistic health practice program is described in Table 1.
| Session (Date) | Topics | No. of Hours |
|---|---|---|
| 1 (7/9/2019) | Assessment of holistic health and designing a personal health promoting program | 3 |
| 2 (21/9/2019) | Maintaining physical health by enhancement of healthy diet and nutrition, physical activity and sleep | 3 |
| 3 (5/10/2019) | Developing mental health and managing life stress | 3 |
| 4 (19/10/2019) | Promoting social health by enhancing interpersonal relationship | 3 |
| 5 (2/11/2019) | Understanding spiritual health and pursuing meaning of life | 3 |
| 6 (9/11/2019) | Group presentation of their pursued health promoting program | 3 |
4.2. Participants and Sampling
The inclusion criteria of the participants of this study were those who have not acquired knowledge related to health, hence only “freshmen” who are the new students in the first-year nursing program could be recruited. A total of 64 first-year nursing students of a nursing school in the publicly-funded higher educational institute were invited to join, and 56 out of 64 students were willing to participate in the study. They were randomly assigned with 27 participants in experimental group and 29 participants in control group. A flow chart of the sampling process is presented in Fig. (1).
4.3. Ethical Consideration
Ethical approval was obtained from the nursing school before carrying out the study. Participation in the study was voluntary and anonymous, and all participants were invited after they were informed about the purpose and procedure of the study. They had the right to withdraw at any time during the study. Participants signed an informed consent form before completing the online questionnaire. Confidentiality was guaranteed.
4.4. Data Collection
Data collection was done in the public nursing school. All participants had signed an informed consent after a briefing of the details of the study by the principal investigator. Then, the participants were asked to complete the online pre-test questionnaires by themselves within the date from 30/8/2019 to 7/9/2019. After the 3-month intervention, all participants from the experimental and control groups were again requested to fill in the online post-test questionnaire by themselves within the period from 9/11/2019 to 19/11/2019.
4.5. The Measurements
The online questionnaires for the pre-test and post-test were the same in content, which included demographic information and the measurements tools (i.e. HPLP-II, ESTEEM & GSES) to determine the health promoting behaviors, self-esteem, and self-efficacy of the participants, respectively.
4.5.1. The Chinese version of Health Promotion Lifestyle Profile-II (HPLP-II)
HPLP-II is composed of 52 items with 6 domains: health responsibility (9 items), physical activity (8 items), nutritional habits (9 items), spiritual growth (9 items), interpersonal relations (9 items), and stress management (8 items). Each item contains a score from 1 (never) to 4 (routinely) in a 4-point Likert scale, and each domain contains a single domain score, that is the sum of the total score of each item within each domain. The maximum score of the 6 domains added together is 208. The forward and backward translation of the HPLP-II had been performed by Teng, Yen & Fetzer in 2010 [20]. A study of enrolled nurse students in Hong Kong using the Chinese version of HPLP-II showed a high reliability with Cronbach’s alpha ranging from 0.81 to 0.84 for the 6 domains, and 0.92 for the total score of HPLP-II [21].
4.5.2. The Chinese version of Rosenberg Self-Esteem Scale (ESTEEM)
Rosenberg Self-Esteem Scale (RSES) is composed of 10 items used to measure the self-esteem with a 4-point Likert scale from strongly disagree (1) to strongly agree (4), with 5 items representing positive self-esteem, and 5 items representing negative self-esteem. The highest score of the scale is 40, and the lowest score is 10. This scale had been reported a Cronbach’s alpha of 0.75 in a study conducted with nursing assistants [22]. The Chinese version of Rosenberg Self-Esteem Scale (ESTEEM) had been developed by Shek with an acceptable reliability [23], which had reported a Cronbach’s alpha of 0.78 in a study among Chinese adolescents [24].
4.5.3. The Chinese version of General Self-Efficacy Scale (GSES)
GSES is composed of 10 items which are rated by a 4-point Likert scale from (1) not at all true, (2) barely true, (3) moderately true, and (4) exactly true. GSES is widely used to measure self-efficacy in various countries with high internal consistencies, and it had demonstrated excellent internal consistency in Chinese version with a Crobach’s alpha of 0.91 [25].
5. RESULTS
5.1. Demographic Information
52 out of 56 participants (93% response rate) completed the online pre-test questionnaire in this study, including 13 male nursing students and 39 female nursing students, aged 17 years old or above. Almost 80% of participants reported they had no religion; whereas 14% declared they were Buddhist, 2% were Christian, 2% were Catholic, and 2% others. Demographic data of the participants is shown in Table 2. Chi-square test was performed with the demographic data of experimental and control group, and no statistical difference was detected. Details of the Chi-square test of demographic data are presented in Table 3.
5.2. Holistic Health Status
The Chinese version of HLPL-II was used to explore the 6 domains of the holistic health of the participants: health responsibility, physical activity, nutritional habits, spiritual growth, interpersonal relations, and stress management of participants. Results found that the mean of physical activity was the lowest score (mean=17.15) among the 6 domains, followed by health responsibility (mean=18.6), stress management (mean=20.19), nutritional habits (mean=21.23), interpersonal relationship (mean=23.13), and spiritual growth (mean=23.25). The mean score of total HPLP-II was 123.58. Details of each mean, standard deviation, minimum, and maximum scores of the 6 domains of HPLP-II are presented in Table 4.
5.3. Intervention – The Holistic Health Practice Program
38 out of 52 participants (73% response rate), who had filled the pre-test questionnaire, completed the post-test questionnaire in this study. Seventeen participants were from the experimental group and 21 participants were from the control group. There was a significantly positive increase in all 6 domains of HPLP-II (P<0.005), as well as self-esteem (P<0.01) and self-efficacy (P<0.01) in the experimental participants when comparing their pre-test and post-test results. In contrast, there was no significant difference in comparing the pre-test and post-test results of the control group, except for self-esteem, which showed a significant difference (P<0.05). Details of paired t-test of scores of the 6 domains of HPLP-II, ESTEEM, and GSES of the two groups are presented in Tables 5 and 6.
| - | - | n=52 | % |
|---|---|---|---|
| Gender | Male | 13 | 25.0 |
| - | Female | 39 | 75.0 |
| Age | 17 | 4 | 7.7 |
| - | 18 | 28 | 53.8 |
| - | 19 | 13 | 25.0 |
| - | 20 | 5 | 9.6 |
| - | >=21 | 2 | 3.8 |
| Religious | Christian | 1 | 1.9 |
| - | Catholic | 1 | 1.9 |
| - | Buddhist | 7 | 13.5 |
| - | Nil | 42 | 80.8 |
| - | Others | 1 | 1.9 |
| - | - | Experiment group (n=17) |
Control group (n=21) |
χ2 | - | ||
|---|---|---|---|---|---|---|---|
| Gender | Male | 4 | (23.53%) | 3 | (14.29%) | 0.53 | NS |
| - | Female | 13 | (76.47%) | 18 | (85.71%) | - | - |
| Age | 17 | 1 | (5.88%) | 2 | (9.52%) | 3.96 | NS |
| - | 18 | 10 | (58.82%) | 10 | (47.62%) | - | - |
| - | 19 | 3 | (17.65%) | 6 | (28.57%) | - | - |
| - | 20 | 1 | (5.88%) | 3 | (14.29%) | - | - |
| >=21 | 2 | (11.77%) | - | - | - | - | |
| Religious | Catholic | 1 | (5.88%) | - | - | 3.40 | NS |
| - | Buddhist | 3 | (17.65%) | 2 | (9.52%) | - | - |
| - | Nil | 12 | (70.59%) | 19 | (90.48%) | - | - |
| - | Others | 1 | (5.88%) | - | - | - | - |
| Subscales | Mean | SD | Min | Max |
|---|---|---|---|---|
| Health responsibility | 18.62 | 4.01 | 11 | 31 |
| Physical activity | 17.15 | 4.23 | 8 | 27 |
| Nutritional habits | 21.23 | 3.83 | 12 | 32 |
| Spiritual growth | 23.25 | 4.83 | 14 | 35 |
| Interpersonal relations | 23.13 | 4.28 | 12 | 34 |
| Stress management | 20.19 | 3.58 | 13 | 28 |
| 6 Domains (Total) | 123.58 | 18.28 | 88 | 170 |
| Experimental Group | Mean (SD) | N | t | df |
Sig. (2-tailed) |
|
|---|---|---|---|---|---|---|
| Health responsibility | pre-test | 18.76 (3.85) | 17 | -3.811 | 16 | .002** |
| post-test | 23.24 (4.53) | 17 | ||||
| Physical activity | pre-test | 16.94 (3.34) | 17 | -3.913 | 16 | .001** |
| post-test | 20.82 (4.88) | 17 | ||||
| Nutritional habits | pre-test | 20.94 (3.19) | 17 | -5.948 | 16 | .000*** |
| post-test | 26.53 (2.85) | 17 | ||||
| Spiritual growth | pre-test | 23.35 (4.40) | 17 | -5.550 | 16 | .000*** |
| post-test | 28.82 (3.91) | 17 | ||||
| Interpersonal relations | pre-test | 23.00 (4.83) | 17 | -6.427 | 16 | .000*** |
| post-test | 28.18 (3.92) | 17 | ||||
| Stress management | pre-test | 19.88 (3.33) | 17 | -6.202 | 16 | .000*** |
| post-test | 24.94 (3.13) | 17 | ||||
| Total 6 domains | pre-test | 122.88 (15.24) | 17 | -6.316 | 16 | .000*** |
| post-test | 152.53 (14.56) | 17 | ||||
| Control Group | Mean (SD) | N | t | df |
Sig. (2-tailed) |
|
| Health responsibility | pre-test | 17.57 (3.34) | 21 | -2.086 | 20 | .050 NS |
| post-test | 19.19 (5.22) | 21 | ||||
| Physical activity | pre-test | 16.33 (3.77) | 21 | -.801 | 20 | .432 NS |
| post-test | 17.00 (4.55) | 21 | ||||
| Nutritional habits | pre-test | 20.67 (3.28) | 21 | -1.503 | 20 | .148 NS |
| post-test | 21.52 (3.60) | 21 | ||||
| Spiritual growth | pre-test | 22.90 (5.68) | 21 | -.786 | 20 | .441 NS |
| post-test | 23.71 (5.27) | 21 | ||||
| Interpersonal relations | pre-test | 23.14 (4.91) | 21 | -1.131 | 20 | .272 NS |
| post-test | 23.95 (4.88) | 21 | ||||
| Stress management | pre-test | 20.48 (3.70) | 21 | -1.347 | 20 | .193 NS |
| post-test | 21.57 (3.87) | 21 | ||||
| Total 6 domains | pre-test | 121.10 (17.83) | 21 | -1.551 | 20 | .136 NS |
| post-test | 126.95 (23.15) | 21 | ||||
| Experimental Group | Mean (SD) | N | t | df |
Sig. (2-tailed) |
|
|---|---|---|---|---|---|---|
| ESTEEM | pre-test | 26.59 (3.43) | 17 | -3.542 | 16 | .003** |
| post-test | 29.24 (3.23) | 17 | ||||
| GSES | pre-test | 24.29 (4.78) | 17 | -3.227 | 16 | .005** |
| post-test | 28.18 (2.58) | 17 | ||||
| Control Group | Mean (SD) | N | t | df |
Sig. (2-tailed) |
|
| ESTEEM | pre-test | 24.48 (6.02) | 21 | -2.092 | 20 | .049* |
| post-test | 25.81 (5.84) | 21 | ||||
| GSES | pre-test | 21.48 (4.30) | 21 | -1.539 | 20 | .139 |
| post-test | 22.67 (5.58) | 21 | ||||
6. DISCUSSION
6.1. Holistic Health Status
This study has added new information on the holistic health status in terms of health promoting behaviors of the first-year nursing students in a Macao public educational institute. Chi-square test showed that there was no difference in their demographic background, which may affect the intervention of the program. Physical activity was found to be the lowest mean score among the 6 domains. This finding was similar to the study of Luk et al. 2014, which investigated the healthy lifestyle of enrolled nursing students in Hong Kong using the Chinese version of HPLP-II. In this study, the subjects’ physical activity was also the lowest, whereas spiritual growth was ranked the highest among the 6 domains in HPLP-II [21]. One possible reason is that the lecture classes of first-year nursing students were mostly scheduled in the morning, as a result, students could get part-time jobs after school for financial reasons [26] and this may affect how much free time they had for physical activity. Secondly, previous studies showed that nursing students had too many presentations and assignments as part of their study requirement [27, 28], which could be a reason why they seldom have time for physical activity. Moreover, studies found that peer groups influenced students' preference to undertake physical activity [29, 30]. However, first-year nursing students may not yet start to establish strong peer relationships in class, and as a result, they lack peer support and company to carry out physical activity. Encouragement to take part in physical activity should be provided to first-year nursing students. Further studies such as focus groups or in-depth interviews can be performed to further explore this phenomenon among nursing students.
In addition, health responsibility was ranked the second-lowest among the 6 domains in the study. This may be due to their lack of health knowledge in improving their personal health since they were only freshmen in their first year of nursing study. Supports from school teachers and peers in sharing health knowledge could be an advantage to these first-year nursing students in improving their health responsibility. On the other hand, spiritual growth was ranked the highest among the 6 domains in this study. One possible reason is that nursing students enjoy the process of helping and respecting others, as well as bringing hope to support significant others. These behaviors may help nursing students enhance their own spiritual growth [31, 32] at the same time.
However, there was no significant difference found when comparing the mean scores of the 6 domains between gender, age, and religion. The reason may be due to the small sample size in certain groups (i.e. male: n=13; age <18 years old: n=4; with religion: n=10). Therefore, no significant relationship was found with the demographic data in this study.
6.2. Effectiveness of the Holistic Health Practice Program
This Holistic Health Practice Program, including the essential components of physical, psychosocial, and spiritual aspects of holistic health, is found to be effective in promoting healthy lifestyles. This result is consistent with other studies for the promotion of health in different health aspects. Previous studies emphasized that encouraging nursing students to promote and enhance their healthy lifestyles was essential to nursing students [4, 33], and interpersonal communication course could significantly help first-year nursing students to improve their self-efficacy [10]. Wills & Kelly (2017) found 3 types of interventions which could encourage nursing students to promote healthy lifestyles: (1) education and training sessions, (2) pulse accelerometer, and (3) online personal wellness goal-setting tool. These interventions should be embedded in the nursing curriculum and delivered within the course of the nursing program [33]. The focus of this program not only helps participants assess and reflect on their holistic health, but also encourages them to develop a health promotion plan to achieve better health. The findings of this study showed that the intervention could significantly enhance the health promoting lifestyle, self-esteem, and self-efficacy of the experimental participants who had undergone a 3-month holistic health practice. Nursing schools should consider integrating the program in the formal nursing curriculum for the promotion of holistic health of first-year nursing students. Or as an alternative, it can be tailor-made as an extracurricular course to enhance the holistic health of the students.
7. LIMITATION
There are only two nursing schools in Macao offering baccalaureate nursing training, and only one school agreed to participate in the study, leading to relatively small sample size. Furthermore, with a drop out rate around 30% in the experimental group, only 17 participants successfully completed the entire program. One possible reason may be due to the mid-term test of their current nursing program. Nevertheless, the results showed a significant difference in the effectiveness of the program, which can be regarded as a pilot study and it will be worth replicating for all nursing students in Macao.
CONCLUSION
This study explored the holistic health, self-esteem, and self-efficacy of Macao first-year nursing students and provided the ground data for further study in the holistic health of nursing students. Study findings showed that physical activity was the lowest score among the 6 domains in the HPLP-II. Nurse educators should encourage first-year nursing students to do more physical activity and school management need to consider incorporating more physical activity into the nursing curriculum, as a support for nursing students to access physical activity during their nursing learning journey.
This study also demonstrated that a Holistic Health Practice Program was effective in promoting healthy lifestyles, self-esteem, and self-efficacy of nursing students. A holistic health practice program is recommended to be integrated into the current nursing curriculum, in order to enhance nursing students' holistic health, self-esteem, self-efficacy, and to better prepare them to become healthy professional nurses in the future.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study is approved by “School of Health Sciences and Sports of Macao Polytechnic Institute, Macao".
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Informed consent has been obtained from all the participants.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENT
Authors would like to show appreciation to trainers from the Nethersole Institute of Continuing Holistic Health Education for providing the training to the participants and the support from the Alice Ho Miu Ling Nethersole Charity Foundation.

